11464777
Graves' Disease
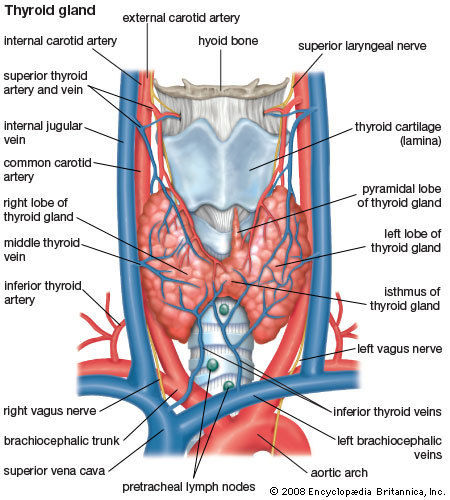
- Anatomy of thyroid gland
- 3 surfaces
- Anterolateral
- Posterior
- Medial
- Anterolateral
- Anterior relations
- Skin
- Venous arch
- Sterohyoid and sterothyroid muscles
- Skin
- Medial relations
- Larynx and tracheal
- Pharynx
- esophagus
- cricothyroid muscle
- superior laryngeal nerve
- Recurrent laryngreal nerve
- Larynx and tracheal
- Posterior relations
- Parathyroid glands
- carotid sheath
- Ansa cervicalis
- sympathetic chain
- Parathyroid glands
- Aterial supply
- Superior thyroid
- inferior thyroid
- Thyroidea ima
- Superior thyroid
- Venous drainage
- Superior thyroid
- Internal jugular
- Internal jugular
- Middle thyroid
- Internal jugular
- Internal jugular
- Inferior thyroid
- L Brachiocephalic
- L Brachiocephalic
- Superior thyroid
- 3 surfaces
- Causes of unintentional weight loss
- Addison's disease (adrenal insufficiency)
- cancer
- A disease of the gut, such
as a stomach ulcer, inflammatory
bowel disease (IBD) or coeliac disease
- Depression
- Diabetes
- Hyperthyroidism
- Addison's disease (adrenal insufficiency)
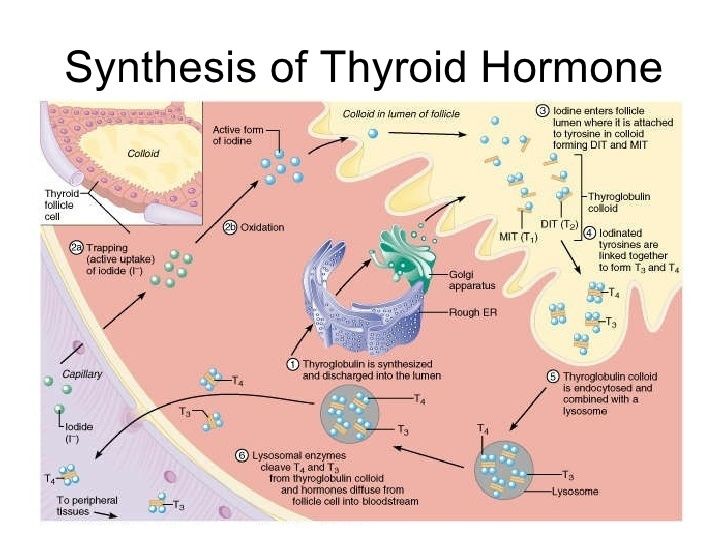
- Thyroid hormone
- Synthesis
- Transport
- Free
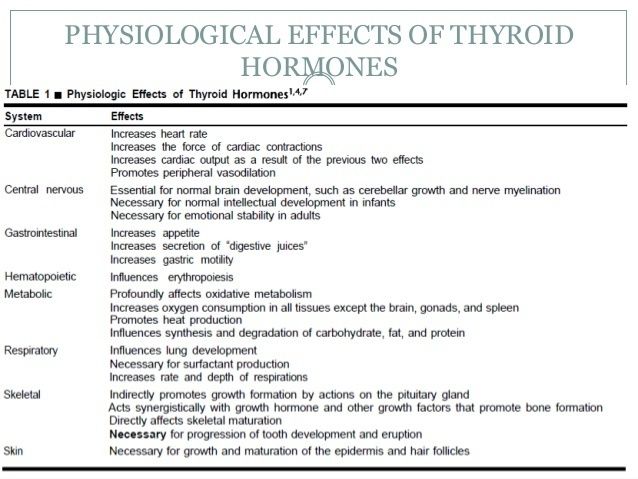
- Produce effect
- Produce effect
- bound to protein
- TBG
- Albumin
- Transthyretin
- TBG
- Free
- Regulation
- The chief stimulator
of thyroid hormone
synthesis is
thyroid-stimulating
hormone from the
anterior pituitary.
- thyroid-releasing
hormone (TRH)
from the
hypothalamus
stimulates TSH
from the pituitary,
which stimulates
thyroid hormone
release.
- thyroid-releasing
hormone (TRH)
from the
hypothalamus
stimulates TSH
from the pituitary,
which stimulates
thyroid hormone
release.
- The chief stimulator
of thyroid hormone
synthesis is
thyroid-stimulating
hormone from the
anterior pituitary.
- Action
- Synthesis
- Hyperthyroidism
- types
- Associated with hyperthyroidism
- Primary
- Graves' disease
- Toxic multinodular goiter
- Hyperfunctional (toxic) adenoma
- Graves' disease
- Secondary
- Thyroid-stimulating hormone
(TSH) adenoma of the pituitary
gland
- Thyroid-stimulating hormone
(TSH) adenoma of the pituitary
gland
- tertiary
- Hypothalamic disease
- Hypothalamic disease
- Primary
- not associated with hyperthyroidism
- Subacute granulomatous thyroiditis
- Subacute granulomatous thyroiditis
- Associated with hyperthyroidism
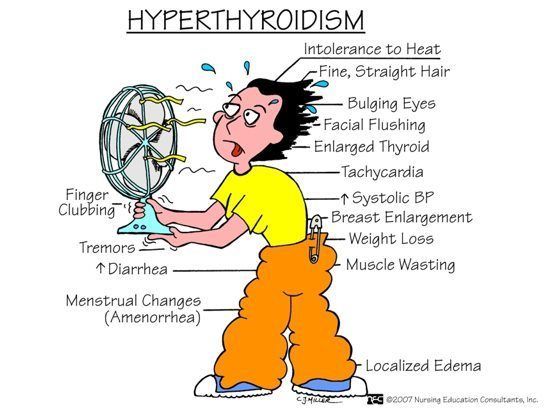
- Symptoms
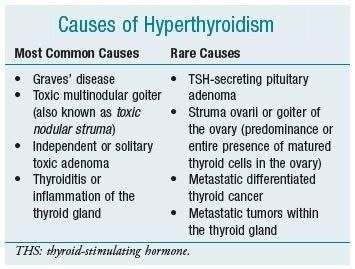
- Causes
- types
- Pathogenesis
- Defect in
suppressor T cell
function >
emergence of CD4+
cells targeted to
TSH receptors
- Intolerant CD4+ T cells
stimulate B cells-->release
Thyroid-Stimulating
Immunoglobulin (TSI)
- Immunoglobulin (TSI) TSI
binds and activates TSH
receptors on thyroid>
hyperactive thyroid gland
- Immunoglobulin (TSI) TSI
binds and activates TSH
receptors on thyroid>
hyperactive thyroid gland
- Intolerant CD4+ T cells
stimulate B cells-->release
Thyroid-Stimulating
Immunoglobulin (TSI)
- Defect in
suppressor T cell
function >
emergence of CD4+
cells targeted to
TSH receptors
- Immunology of Graves disease
- Polymorphisms in CTLA4
that result in reduced in
activity will have less
inhibition of the CTLs
and overstimulation that
can result in them
becoming autoreactive
- Polymorphisms in CTLA4
that result in reduced in
activity will have less
inhibition of the CTLs
and overstimulation that
can result in them
becoming autoreactive
- Histologic findings
- Lymphatic
infiltrates and
follicular
hypertrophy, with
little colloid
present
- Lymphatic
infiltrates and
follicular
hypertrophy, with
little colloid
present
- Prognosis
- Most patients become
hypothyroid and require
replacement
- On occasion, hyperthyroidism
returns because of persisting
thyroid tissue
- Surgery or radioactive iodine ablation
- Surgery or radioactive iodine ablation
- Most patients become
hypothyroid and require
replacement
- Investigations
- Blood sample
- increased serum fT3 and fT4
- decreased TSH
- increased serum fT3 and fT4
- Radioactive iodine uptake
- Ultrasound
- Blood sample
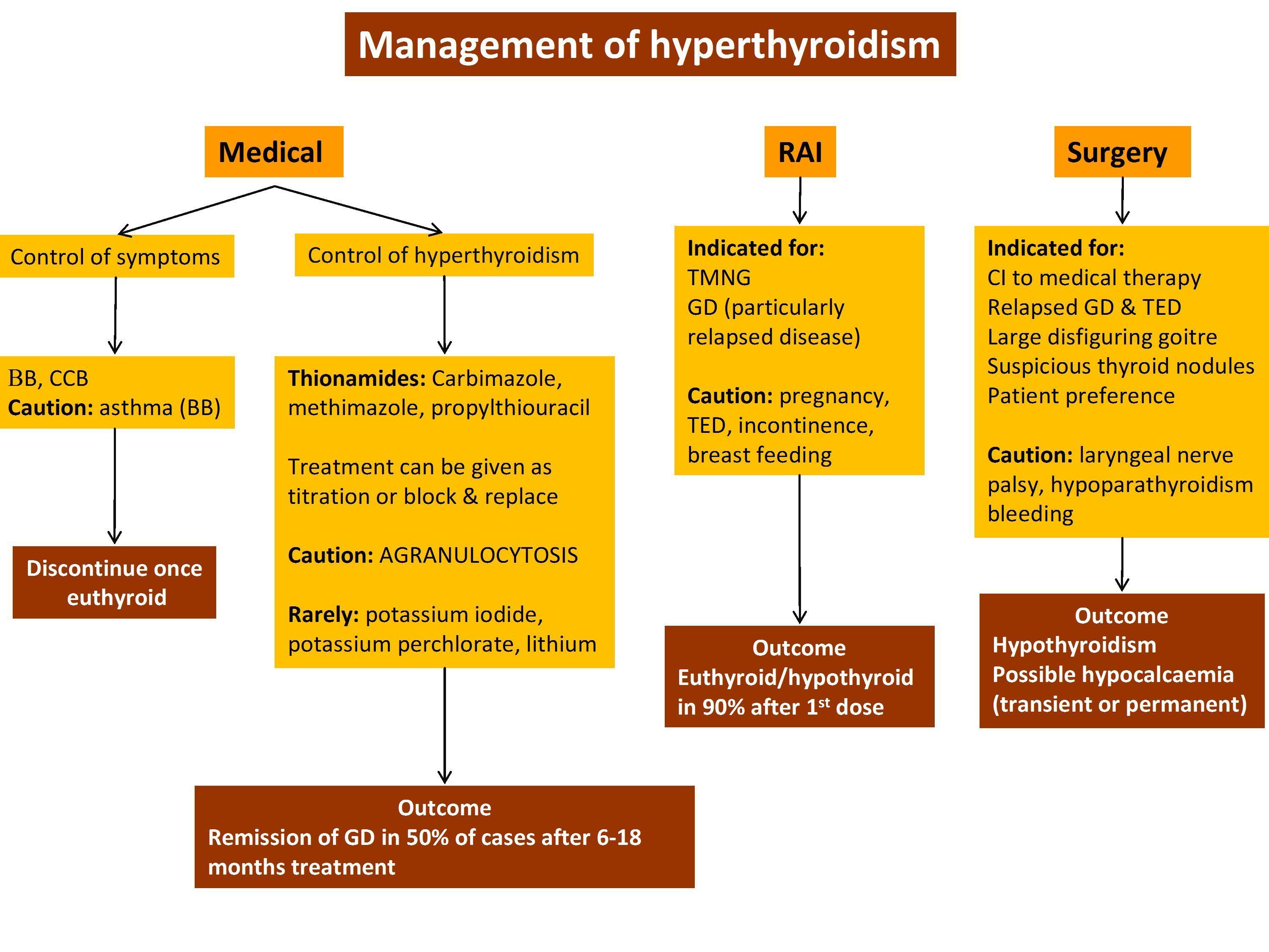
- Treatment
Medienanhänge
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Möchten Sie kostenlos Ihre eigenen Mindmaps mit GoConqr erstellen? Mehr erfahren.