17190275
Beschreibung
Mindmap von Thi Thanh Tuyen Pham, aktualisiert more than 1 year ago
|
|
Erstellt von Thi Thanh Tuyen Pham
vor fast 6 Jahre
|
|
IBD-Crohn's Disease
- PATHOPHYSIOLOGY
- (Mazal, 2014)
- unknown cause
- progressive, systemic autoimmune disorder
- abnormal inflammation of any parts of GI tract
- Discontinuous, “skip” lesions
- unknown cause
- (Hart & Ng, 2015)
- varied mucosal ulcerations
- burrow gut wall
- fistula
- fistula
- narrowed lumen
- obstruction
- obstruction
- cobble stone apperance
- burrow gut wall
- varied mucosal ulcerations
- (Mazal, 2014)
- DIAGNOTIC TESTS
- (Gajendran et al., 2018)
- Laboratories studies
- Serology
- CBC (anemia), C-reactive protein (CRP)
- erythrocyte sedimentation rate (ESR)
- monitor response to treatment
- monitor response to treatment
- CBC (anemia), C-reactive protein (CRP)
- Stool studies
- Serology
- Imaging
- confirm disease location and intestinal complications.
- endoscopy
- obtain tissue ->pathological evaluation
- obtain tissue ->pathological evaluation
- CT, MRI, contrast radiography
- endoscopy
- confirm disease location and intestinal complications.
- Laboratories studies
- (Gajendran et al., 2018)
- COLLABORATIVE CARE
- Nutritional therapy
- (Crohn’s and Colitis Canada, 2016, 2017)
- No special diet →customized to fit pt.
- a well-balanced diet
- Enteral feeding
- insert NG tube or stomach tube
- primary therapy
- secondary treatment: malnutrition
- primary therapy
- insert NG tube or stomach tube
- Total parenteral nutrition (TPN)
- when oral & enteral feeding is inadequate
- when oral & enteral feeding is inadequate
- supplements
- Calcium citrate, Iron, Vitamins D, and B12, Folic acid,
- Calcium citrate, Iron, Vitamins D, and B12, Folic acid,
- No special diet →customized to fit pt.
- (Karakashian & Schub, 2018)
- eliminate certain foods (e.g., bulky grains, hot spices, alcohol, milk products)
- prevent worsening diarrhea, cramping
- prevent worsening diarrhea, cramping
- eliminate certain foods (e.g., bulky grains, hot spices, alcohol, milk products)
- (Crohn’s and Colitis Canada, 2016, 2017)
- Nutritional therapy
- NURSING INTERVENTIONS
- Total parenteral nutrition (TPN)
- ( General Surgery North
York General Hospital,
2013)
- extended bowel rest
- during exacerbation; pre-operation.
- during exacerbation; pre-operation.
- NOT compatible with any other solutions
- be administered by itself
- be administered by itself
- NOT obtain blood samples from same port as TPN infusions.
- Do not abruptly discontinue
- HYPOGLYCEMIA RISK
- HYPOGLYCEMIA RISK
- extended bowel rest
- (Robertson, 2014;
General Surgery North
York General Hospital,
2013)
- RISKS
- Administration-related
- Pneumothorax; Fluid excess/ pulmonary edema.
- Monitor VS closely
- Monitor VS closely
- sepsis, embolism, catheter occlusion
- Pneumothorax; Fluid excess/ pulmonary edema.
- Formulation-related
- nutritional imbalance; electrolyte imbalance
- hypoglycemia, hyperglycemia
- monitor blood glucose
- monitor blood glucose
- nutritional imbalance; electrolyte imbalance
- Administration-related
- RISKS
- ( General Surgery North
York General Hospital,
2013)
- Patient teaching
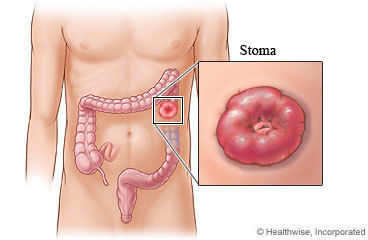
- Ostomy care
- (Crohn’s and
Colitis Canada,
2017)
- examine stoma daily
- healthy stoma
- moist, dark pink to red
- moist, dark pink to red
- skin around stoma
- no redness or sores
- no redness or sores
- healthy stoma
- Empty pouch when 1/3 full
- Change pouch & skin barrier
- if irritated->change skin barrier right away
- regularly: at least 1-2X/week
- if irritated->change skin barrier right away
- not limited to sport and work
- if physician says "all clear"
- if physician says "all clear"
- normal to experience diarrhea or constipation
- Diarrhea → avoid foods make feces more watery
- Constipated→ drinking fruit juices
- Diarrhea → avoid foods make feces more watery
- examine stoma daily
- (Crohn’s and
Colitis Canada,
2017)
- Diet
- (Crohn’s
and
Colitis
Canada,
2017)
- In remission
- eating a well-balanced diet
- no need to avoid any particular kind of food
- eating a well-balanced diet
- During flare-up
- modify diet, avoid
aggravating gut
- avoid trigger foods
- Avoid Alcohol,
Sugar,
Fructose,
Caffeine,
Greasy food
- Avoid Alcohol,
Sugar,
Fructose,
Caffeine,
Greasy food
- Eat smaller meals, q2-3h
- Avoid drinking a lot of fluid during a meal
- Reduce fat intake
- avoid trigger foods
- modify diet, avoid
aggravating gut
- In remission
- (Crohn’s
and
Colitis
Canada,
2017)
- Ostomy care
- Overall goals
(Cope, 2015)
- induce & maintain remission
- prevent complications
- induce & maintain remission
- Total parenteral nutrition (TPN)
Medienanhänge
{kind=link}
{kind=link}
Möchten Sie kostenlos Ihre eigenen Mindmaps mit GoConqr erstellen? Mehr erfahren.