3872535
Pain & Pain Management
- What is pain?
- "An unpleasant sensory and
emotional experience, associated with
actual or potential tissue damage, or
described in terms such as damage."
- Pain is a subjective
experience rather than just
a sensation in humans
- Pain protects
- Pain protects
- Pain is a subjective
experience rather than just
a sensation in humans
- "An unpleasant sensory and
emotional experience, associated with
actual or potential tissue damage, or
described in terms such as damage."
- Types of Pain
- Acute Pain
- A normal and time limited
response to trauma or other
noxious experience, including pain
related to medical procedures and
acute medical conditions (eg. Shingles)
- A normal and time limited
response to trauma or other
noxious experience, including pain
related to medical procedures and
acute medical conditions (eg. Shingles)
- Recurrent pain
- Stems from benign causes and is
characterised by intense episodes of pain
interspersed with no pain (eg. Migraine)
- Stems from benign causes and is
characterised by intense episodes of pain
interspersed with no pain (eg. Migraine)
- Sub Acute Phase
- Transition from
acute to chronic
pain
- The time from tissue
healing (1-2 months)
to the 6 month point
currently define the
presence of chronic
pain.
- Opportunity
to prevent
transition
- Presumably changes
are occurring in the
nervous system
during this time
- The time from tissue
healing (1-2 months)
to the 6 month point
currently define the
presence of chronic
pain.
- Transition from
acute to chronic
pain
- Chronic (Non-Cancer) Pain
- Constant daily pain
for a period of 3
months or more
- Pain is present all the time,
though of varying intensity,
stemming from benign causes.
Ensures beyond the time of
normal healing eg. low back pain.
- Chronic progressive pain that
increases in intensity as the
concomitant medical condition
worsens eg. pain associated with
rheumatoid arthritis and cancer.
- Constant daily pain
for a period of 3
months or more
- Cancer-related Pain
- Evidence that
cancer pain is
under-treated
- Evidence that
cancer pain is
under-treated
- Categorisation Based on
Underlying Pathophsyiology
- Nociceptive Pain
- Pain that arises from
actual or threatened
damage to non-neural
tissue
- Pain that arises from
actual or threatened
damage to non-neural
tissue
- Nociceptive inflammatory Pain
- Part of normal
inflammatory response
to injury
- Part of normal
inflammatory response
to injury
- Neuropathic Pain
- May be caused by a lesion or dysfunction
in the peripheral and/or central nervous
system. Frequently peristent and
frequently involves spontaneous pain in
absence of an identifiable stimulus.
- May be caused by a lesion or dysfunction
in the peripheral and/or central nervous
system. Frequently peristent and
frequently involves spontaneous pain in
absence of an identifiable stimulus.
- Nociceptive Pain
- Acute Pain
- Experience of Pain
- Pain is different from other senses
as it is typically accompanied by an
emotional component
- The meaning of pain
substantially determines how
it is perceived
- Pain is heavily influenced
by the context in which it
is experienced.
- Pain has a substantial
cultural component.
- Themes of those who have
experienced Chronic Pain
- Stigma - considered
'psychologically defective'
- Loss of control of one's
life; struggling with
everyday life
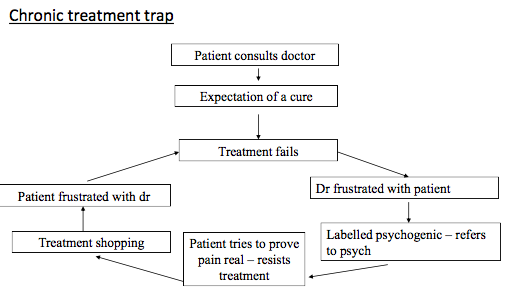
- Frustration with health
care professionals
- Lack of effective
treatments
- Perceived lack of creditability
- not being believed
- End of happiness; depression
- Erosion of relationships
- Disruption of careers;
becoming improverished
- Frustration with compensation sysetem
- Sleep problems
- Perceived lack of empathy
- Stigma - considered
'psychologically defective'
- Pain is different from other senses
as it is typically accompanied by an
emotional component
- Early Understanding of Pain
- Tissue damage causes
the sensation of pain
- Psychology involved as a
consequence of pain
without a casual influence
- Pain sensation has a
single cause
- Pain considered either psychogenic or organic
- Tissue damage causes
the sensation of pain
- Bio-Psycho-Social Model of Pain
- Physical
- Psychological
- Environmental (social)
- Need to assess all
components
- Interdisciplinary approach
- Interdisciplinary approach
- Physical
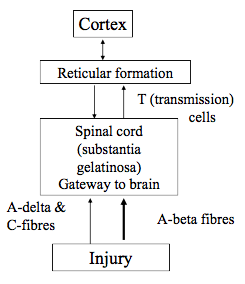
- Physiology of Pain - Gate Theory
- Neural Mechanisms
- A-delta fibres are associated with the conduct of fast,
sharp, well localised pain or pain experienced quickly.
These fibres are small myelinated fibres which facilitate
fast transmission of information.
- A-delta fibres enter the spinal column at the dorsal horn and then
project to particular areas of the thalamus and the sensory areas of
the cerebral cortex –hence the provision of localised pain information.
- C-fibres are small nerve fibres that are un- myelinated and conduct
slow, aching, burning, long lasting and poorly localised pain.
- The C-fibres project to different areas of the brain,
including thalamic, limbic, and cortical areas. These areas
are involved in mood, emotion and motivation and so these
aspects of pain are related more to C-fibre activation.
- A-beta fibres – large diameter fibres which have been
proposed to send “non-pain” messages.
- Gate Theory
- Central assumption of the Gate Theory is that different
parts of the CNS are involved in the pain experience.
- They affect the operation of a gate-like
mechanism in the dorsal horns of the spinal
column that controls the flow of pain
stimulation in the brain.
- Pain sensations are modified as they are
conducted to the brain up the spinal column, and
they are also influenced by messages coming
down from the brain that interpret the
experience.
- When A-beta fibres fire they act to keep
the gate of the brain closed. WhenA-delta
and C-fibres fire above a certain
threshold, the gate opens and pain
messages are sent to the brain.
- Messages coming down from the
brain can also open or close the gate.
- Messages coming down from the
brain can also open or close the gate.
- Central assumption of the Gate Theory is that different
parts of the CNS are involved in the pain experience.
- A-delta fibres are associated with the conduct of fast,
sharp, well localised pain or pain experienced quickly.
These fibres are small myelinated fibres which facilitate
fast transmission of information.
- Neural Mechanisms
- Recent Understanding of Chronic Pain
- In inflammatory and neuropathic pain and pain
caused by abnormal central processing, amplification
of excitability of neurons within the CNS may occur.
- Called Central Sensitisation
- It's in greater pain experience
- It's in greater pain experience
- Called Central Sensitisation
- In inflammatory and neuropathic pain and pain
caused by abnormal central processing, amplification
of excitability of neurons within the CNS may occur.
- Neuro-chemical Basis of Pain
- Bradykinin and prostaglandins are
substances released by tissue damage.
- Bradykinin is a blood-borne neuropeptide that is
cleaved away from a large inert molecule by
enzymes a fraction of a second following injury.
- Bradykinin and prostaglandins stimulate pain
associated neurons and are considered to be
major producers of pain.
- Glutamate and Substance P are neurotransmitters
that act in the spinal cord to increase neural firings
related to pain.
- Substance P is secreted by pain fibres
and crosses the synapse to T cells,
triggering their firing.
- Opiates affect the brain - there must be
naturally occurring opiates in the body
- Led to discovery of endorphins (enkaphalins and
dynorphin) which inhibit pain fibres releasing Substance P.
- Endorphin means “the morphine within” and was
given this name as it has properties similar to
those of heroin and morphine. It is a powerful
pain killer and mood elevator.
- Naloxone, an opiate antagonist
appears to reduce pain relieving ability
of body through endogenous opioids.
- Naloxone, an opiate antagonist
appears to reduce pain relieving ability
of body through endogenous opioids.
- Endorphin means “the morphine within” and was
given this name as it has properties similar to
those of heroin and morphine. It is a powerful
pain killer and mood elevator.
- Led to discovery of endorphins (enkaphalins and
dynorphin) which inhibit pain fibres releasing Substance P.
- Bradykinin and prostaglandins are
substances released by tissue damage.
- Psychosocial Aspects of Pain
- Fordyce identified 4 aspects of Pain
- Nociception
- potential tissue damaging
energy impinging on
specialised nerve endings of
a-delta and C-fibres. i.e., input
to pain receptive nerve
endings.
- potential tissue damaging
energy impinging on
specialised nerve endings of
a-delta and C-fibres. i.e., input
to pain receptive nerve
endings.
- Pain
- perceived nociceptive input
to the nervous system.
- perceived nociceptive input
to the nervous system.
- Suffering
- negative affective (emotional) response
generated in higher nervous centres by pain
and other situations, e.g., loss.
- negative affective (emotional) response
generated in higher nervous centres by pain
and other situations, e.g., loss.
- Pain Behaviour
- All forms of behaviour generated by the
individual commonly understood to
reflect the presence of nociception.
- All forms of behaviour generated by the
individual commonly understood to
reflect the presence of nociception.
- Nociception
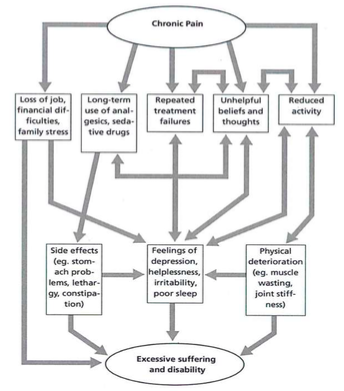
- Chronic Pain
- deep psychological consequences
- Persistent attempts to react and adapt to
pain frequently result in emotional problems
such as depression, anxiety and fear
- Affects cognition – e.g., concentration and memory;
- Affects interpersonal relationships.
- Affects interpersonal relationships.
- Affects cognition – e.g., concentration and memory;
- Persistent attempts to react and adapt to
pain frequently result in emotional problems
such as depression, anxiety and fear
- deep psychological consequences
- Fordyce identified 4 aspects of Pain
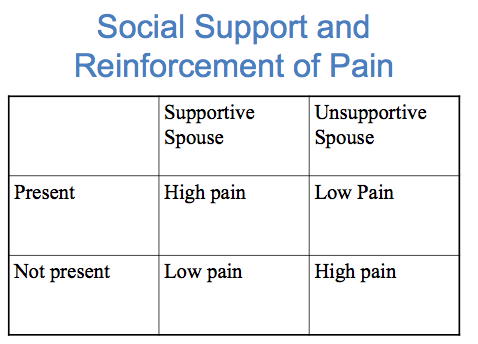
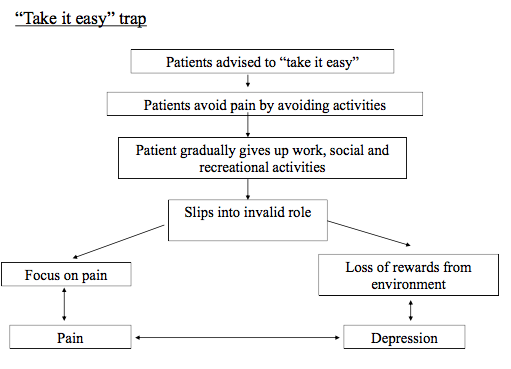
- Learning Pain Behaviours
- Pain behaviours may be reinforced, i.e., the likelihood of
their occurrence will increase if they are rewarded. E.g.,
relief from pain when ask for medication (“medication on
demand”; worker’s compensation for pain).
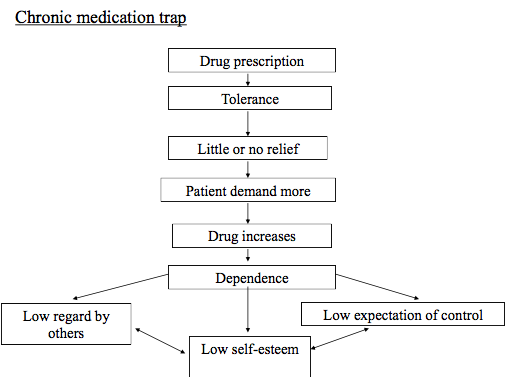
- Implication for development of inappropriate use
of pain relieving mediation, following acute pain
experience (e.g., surgery).
- Pain behaviours may be influenced by
avoidance learning. E.g., if it hurts to walk 500m
next time you only walk 400 m to avoid pain.
Causes reduction in activities engaged in.
- Pain behaviours may be influenced by
avoidance learning. E.g., if it hurts to walk 500m
next time you only walk 400 m to avoid pain.
Causes reduction in activities engaged in.
- Implication for development of inappropriate use
of pain relieving mediation, following acute pain
experience (e.g., surgery).
- Pain behaviours may be reinforced, i.e., the likelihood of
their occurrence will increase if they are rewarded. E.g.,
relief from pain when ask for medication (“medication on
demand”; worker’s compensation for pain).
- Goals of Pain Managment
- Improve understanding of persistent pain
- Improve function despite ongoing pain
- Modify perceptions of pain and suffering
- Provide coping skills and strategies
- Promote self-management
- Reduce or modify future use of health care services
- Improve understanding of persistent pain
- Improving Coping with Chronic Pain
- Behaviour therapy
- A managed approach to behavioural change
using the basic principles of operant
conditioning (learning principles).
- Increasing rewards for well behaviour and teaching increasing self-rewards;
- Decrease rewards for pain behaviour but without lack of sympathy;
- Reduce avoidance behaviour – plan for a length of time for an
activity and plan achievable but not to modest goals;
- Increase general fitness – can be positively reinforcing.
- Increasing rewards for well behaviour and teaching increasing self-rewards;
- A managed approach to behavioural change
using the basic principles of operant
conditioning (learning principles).
- Cognitive behavioural therapy
- Primary focus on changing cognitive activity to achieve
changes in behaviour, thought and emotion.
- Patients are encouraged to develop
insight into self- defeating patterns
they have fallen into;
- Develop ways of challenging these;
- Increase self-efficacy;
- Problem solving in relation to social and relationship changes.
- Patients are encouraged to develop
insight into self- defeating patterns
they have fallen into;
- Primary focus on changing cognitive activity to achieve
changes in behaviour, thought and emotion.
- Biofeedback and relaxation – learn new skills.
- Behaviour therapy
- Setting Goals
- Realistic
- Achievable
- Relevant
- Specific or concrete
- Important motivation
- Long-term/Short-term
- Long-term/Short-term
- Realistic
- Coping with Acute Pain
- Pain can be accompanied by
anxiety, stress, and physical tension,
which can exacerbate and/or
prolong the acute pain episode
- A number of psychological
strategies can be used to help
patients cope with these, as well as
thoughts and emotions that may
increase physiological arousal and
reduce the patients’ sense of control
- Pain can be accompanied by
anxiety, stress, and physical tension,
which can exacerbate and/or
prolong the acute pain episode
- Pain Information
- This helps patients understand
what is “normal” under their
particular circumstances and can
reduce anxiety.
- Patients should be given as much
information as possible about
nature of pain they might expect
from a procedure or trauma.
- Patients should be given as much
information as possible about
nature of pain they might expect
from a procedure or trauma.
- This helps patients understand
what is “normal” under their
particular circumstances and can
reduce anxiety.
- Distraction
- Tell patients that although strong,
pain signals are one of many
possible sensations that they may
notice at any given moment, and
that actively distracting from the
signal may provide some relief;
- Ask patients to gently guide their
attention to another stimulus,
such as television, music, reading,
simple puzzles, or conversations
with supportive family/friends;
- Encourage patients to
imagine a preferred place or
situation where they feel
calm and relaxed, in as much
detail as possible, pulling in
all of their senses, including
sights, sounds, smells, touch,
and taste (Guided imagery).
- Encourage patients to
imagine a preferred place or
situation where they feel
calm and relaxed, in as much
detail as possible, pulling in
all of their senses, including
sights, sounds, smells, touch,
and taste (Guided imagery).
- Ask patients to gently guide their
attention to another stimulus,
such as television, music, reading,
simple puzzles, or conversations
with supportive family/friends;
- Tell patients that although strong,
pain signals are one of many
possible sensations that they may
notice at any given moment, and
that actively distracting from the
signal may provide some relief;
- Cognitive Approaches
- Discuss the role of thoughts on patients’
sense of coping with pain, and their
relationship to physiological arousal
- Encourage patients to generate and practice
positive self-talk that emphasizes their ability
to cope with the pain
- Patients should also be reassured that the pain
episode is of limited duration, and that they can
remind themselves that it will pass.
- Patients should also be reassured that the pain
episode is of limited duration, and that they can
remind themselves that it will pass.
- Encourage patients to generate and practice
positive self-talk that emphasizes their ability
to cope with the pain
- Discuss the role of thoughts on patients’
sense of coping with pain, and their
relationship to physiological arousal
- Appropriate Use of Analgesia
- For patients that do not experience
adequate analgesia, can lead to chronic
pain
- Important to provide effective
pharmacological analgesia as soon
as possible during, or even before,
an acute pain episode
- An emphasis should be placed on taking
medications as scheduled, not only when
pain emerges, and patients’ concerns
regarding side effects, including any
addiction potential, should be addressed
- An emphasis should be placed on taking
medications as scheduled, not only when
pain emerges, and patients’ concerns
regarding side effects, including any
addiction potential, should be addressed
- Important to provide effective
pharmacological analgesia as soon
as possible during, or even before,
an acute pain episode
- For patients that do not experience
adequate analgesia, can lead to chronic
pain
Medienanhänge
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Möchten Sie kostenlos Ihre eigenen Mindmaps mit GoConqr erstellen? Mehr erfahren.