5010096
Beschreibung
Mindmap von Heather Snaith, aktualisiert more than 1 year ago
|
|
Erstellt von Heather Snaith
vor fast 9 Jahre
|
|
Audiology - Week 2 - Types of H.L.
- WHY relates to SALT
- OBVS IMPACTS
SPEECH
DEVELOPMENT
- Critical period first 3 years -
if you don’t pick up speech
coz of hearing impairment
you get significantly behind
in lang. dev.
- Speech discrimination
= functional outcome
measure of successful
amplification
- SLT's can be first to pick
up a hearing problem,
e.g. if a child is not
producing any sounds of
a certain freq.
- Big referral
source for
audiology & vice verca
- Big referral
source for
audiology & vice verca
- Children who are
aided need big SALT
input
- OTHER INFO SLIDES
£$ ONWARDS NOT
NOTED HERE
- OBVS IMPACTS
SPEECH
DEVELOPMENT
- PITCH
- VOLUME
- VOLUME
- Consonant and sibilant sounds
higher in pitch and not so loudowel
sounds louder and lower in pitch
- Consonant and sibilant
sounds higher in pitch and
not so loud
- DEGREES OF
HEARING LOSS
(Not pitch
specific)
- Consonant and sibilant
sounds higher in pitch and
not so loud
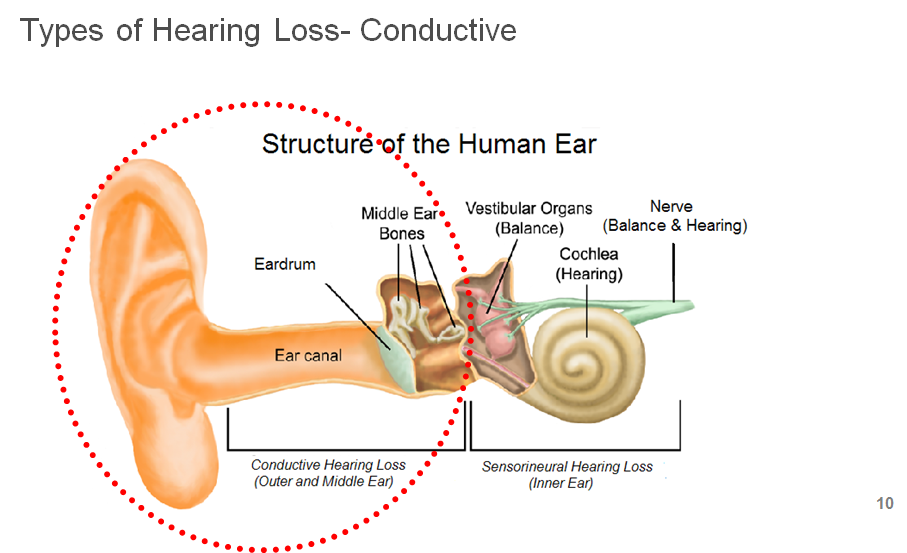
- TYPES
- CONDUCTIVE
- External Ear
- Middle Ear
- Reduces sound
conduction through
to the inner ear
- CERUMEN / WAX
- Foreign body
- Inflaammatory
swelling / debris
(otitis externa)
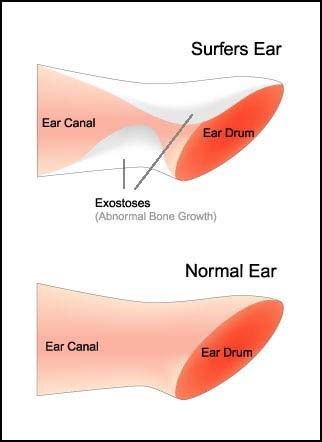
- Acquired/congenital aural atresia (absence
of canal) / exostoses (narrowing") 'surfer's
ear'
- CHRONIC / BRIEF
- AIDED / MANAGED
- OTITIS MEDIA -
Acute (Infectious)
or Chronic
(Non-infectious)
- Can be drained
(although not
cured) by grommits
- Children have small
flat tube, more prone
to block if inflamed –
more adult like after 6
years)
- More than 7 in 10
children have at
least one episode
of glue ear before
they are four years
old.
- Only the 5-8%
severe/persistent
minority are cases
for treatment
- More than 7 in 10
children have at
least one episode
of glue ear before
they are four years
old.
- Children have small
flat tube, more prone
to block if inflamed –
more adult like after 6
years)
- Fluid builds up in
middle ear and
eustacian tube,
prevents the ear
drum vibrating
properly
- Eustachian tube is the 'vent' to help maintain
same pressure as other side of TM. Air in middle
ear passes into nearby cells over time. If it is not
replaced by air coming up the tube a vacuum
will form, sucking the TM inwards and fluid out
from the cells giving glue like consistency
- Most important
question: How long
have they had it? Fluctuating?
- Most important
question: How long
have they had it? Fluctuating?
- Eustachian tube is the 'vent' to help maintain
same pressure as other side of TM. Air in middle
ear passes into nearby cells over time. If it is not
replaced by air coming up the tube a vacuum
will form, sucking the TM inwards and fluid out
from the cells giving glue like consistency
- May need
temporary
hearing aids
- Can be drained
(although not
cured) by grommits
- Otosclerosis
(fusion of the
bones) e.g. after
pregnancy /
genetic
- Perforation of
T.M. (trauma,
infection /
operation)
- Ossicular
discontinuity
(trauma / birth
defect)
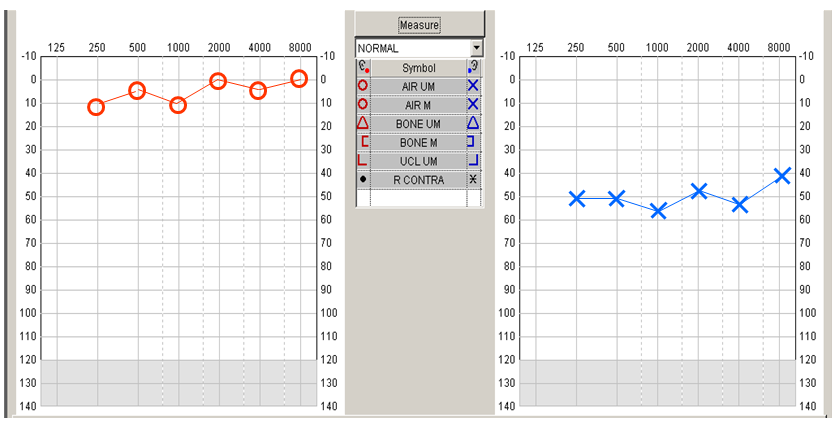
- People w conductive
HL will still have good
bone conduction
- Note raised AC
thresholds
- Then note the BC thresholds
WNL, as skipping middle
ear...
- Then note the BC thresholds
WNL, as skipping middle
ear...
- Note raised AC
thresholds
- External Ear
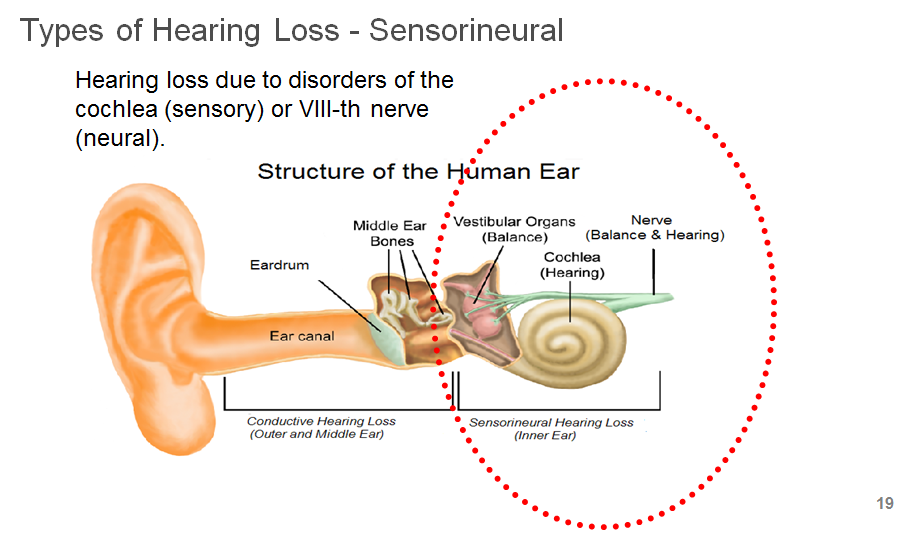
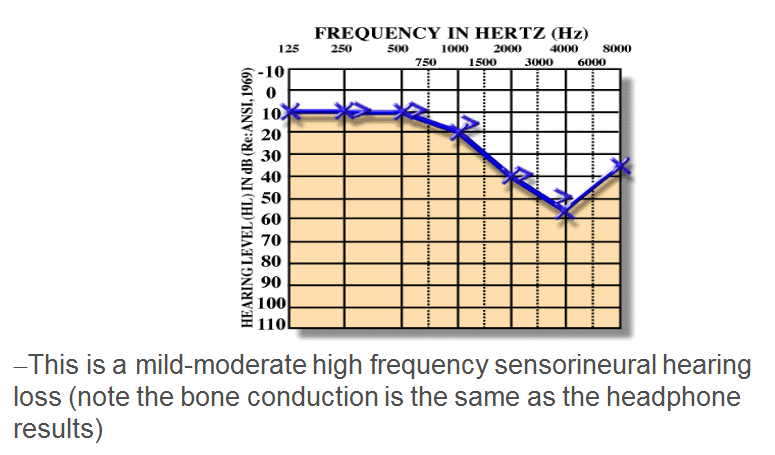
- SENSORINEURAL
- Congenital~1.5/1000
- Maternal infection -
particularly CMV, also
rubella, HSV
- CMV - usually
progressive
H.L.
- CMV - usually
progressive
H.L.
- Birth complications -
premature, asphyxia
etc...
- Genetic about 50% of
HL in children, but
most (90%) born to hearing
parents
- Maternal infection -
particularly CMV, also
rubella, HSV
- Acquired
- e.g. of
Presbycusis
(getting old)
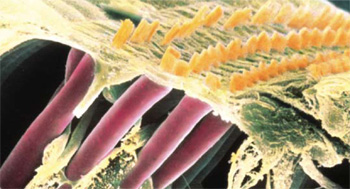
- Inner hair cells
become less
sensitive
- Inner hair cells
become less
sensitive
- Noise damage
- hair cells can
be sheared off
- Typically shows notch
/ raised thresholds
on audiogram at
3-4kHz
- Can be more
genetically
predisposed to
this
- Losses up to 50dB will be due
to outer hair cell losses.
- Hearing losses above 50dB will be due to
inner hair cell losses.
- Typically shows notch
/ raised thresholds
on audiogram at
3-4kHz
- Infection - e.g.
Meningitis, mumps
/ measles
- Meningitis, cochlea
can become ossified
(turn to bone) so
tend to put a
cochlea implant in
sooner rather than
later
- Meningitis, cochlea
can become ossified
(turn to bone) so
tend to put a
cochlea implant in
sooner rather than
later
- Ototoxic drugs
- e.g. Antimalarials
4. Chemotherapy
- Also general toxins
e.g. viruses,
bacteria,
environmental,
alcohol
- e.g. Antimalarials
4. Chemotherapy
- Trauma to
the ear
- Fracture of
the temporal
bone lead to
HL in 70-80%
cases
- Fracture of
the temporal
bone lead to
HL in 70-80%
cases
- e.g. of
Presbycusis
(getting old)
- Outer hair cells typicaly the
ones to go - provide
descrimination
- Inner hair cells are the
big workers - send signal
off to the brain, less likely
to falter
- Inner hair cells are the
big workers - send signal
off to the brain, less likely
to falter
- Inner Ear or
hearing nerve
- Usually
permanent in
nature
- Bone Conduction
thresholds and
Air Conduction
are the same -
there is no air
bone gap
- This loss is where the low
powered/high freq sibilants
and consonants lie and these
are the most important
components of speech
- "Everyone mumbles
nowerdays."
- "Everyone mumbles
nowerdays."
- FACTORS AFFECTING SPEECH: Severity,
frequency and relevant speech sounds,
cause (temp/permanent), progressive,
aided, aided thresholds and
descrimination
- Find out if children
are wearing their
hearing aids
- Find out if children
are wearing their
hearing aids
- Congenital~1.5/1000
- TEMPORARY / PERMANENT
- CONDUCTIVE
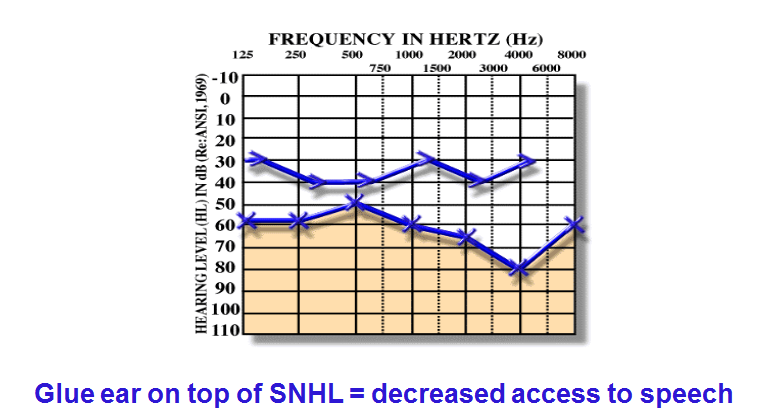
- MIXED H.L.
- 'NON ORGANIC' / Faking it
- Person displays a
deficit, where no
true hearing loss
exists
- Typified by lack of
co-operation / difficulty
concentrating on listening
tasks
- Scale anything
from
phsycosematic -
attention
seeking
- Variable,
unreliable
results
- Person displays a
deficit, where no
true hearing loss
exists
- AUDITORY NEUROPATHY
- Outer hair cell function of
inner ear preserved,
damage to inner hair cells,
or some part of the pathway
that relays signals to the
brain
- Damage to
inner hair
cells
- Connection
between inner
hair cell and
nerve
- Damage to
auditory
nerve
- Functional
deficit varies
greatly
- Lots of SLT
- Outer hair cell function of
inner ear preserved,
damage to inner hair cells,
or some part of the pathway
that relays signals to the
brain
- CENTRAL AUDITORY PROCESSING DISORDER
- Hearing is normal but child
has difficulty differentiating,
locating and recognising
sounds
- Really tricky to
diagnose - may be
highlighted by SALT
- Struggle with hearing,
particularly in
background noise
- Difficulty
following
oral
instructions
- Diff understanding
rapid / degraded
speech
- Is it possible this
could relate to
SLI?
- Hearing is normal but child
has difficulty differentiating,
locating and recognising
sounds
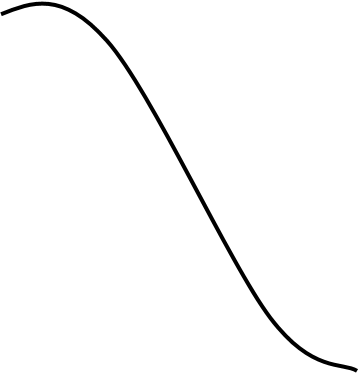
- AUDIOGRAM CONFIGURATIONS:
- Presbycusis
- Conductive - e.g.
glue ear /
Meniere’s
- Congenital -
long term
'cookie bite'
(may be hard to
aid)
- All freq
(should aid
well)
- Noise exposure - dip
at 3-4kHz
- Presbycusis
Medienanhänge
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Möchten Sie kostenlos Ihre eigenen Mindmaps mit GoConqr erstellen? Mehr erfahren.