8600521
Beschreibung
Mindmap von Sara Hojabri, aktualisiert more than 1 year ago
|
|
Erstellt von Sara Hojabri
vor mehr als 7 Jahre
|
|
Skin Pathology
- Infections
- Viral
- – HPV: warts/verrucae,
Genital warts
- – Herpes zoster/simplex
- –HIV: Transient, itchy
eruption
- – HPV: warts/verrucae,
Genital warts
- Bacterial
- Abscesses, Furuncle/Boil (single hair follicle),
Carbuncle (several contiguous hair follicles)
- Mycobacteria: TB of skin, Leprosy
- Impetigo: S. aureus in kids;
Streptococcus in older, ‘scrum pox’
- Cellulitis: Swollen, hot, red, painful, S. pyogenes
- Abscesses, Furuncle/Boil (single hair follicle),
Carbuncle (several contiguous hair follicles)
- Fungal
- Superficial: Tinea: ringworm,
athletes foot; Candida: thrush
- Deeper: Tropical,
immunosuppressed
- Superficial: Tinea: ringworm,
athletes foot; Candida: thrush
- Protozoan
- Rare in temperate climate
Leishmaniasis: sandflies;
amoebiasis, trypanosomiasis
- Rare in temperate climate
Leishmaniasis: sandflies;
amoebiasis, trypanosomiasis
- Viral
- Non-Infectious
Inflammation
- Lichen Planus
- Puritic, purple, polygonal, planar papules and plaques
Destruction of keratinocytes ,1% pop, middle age
Lymphohistiocytic infiltrate at dermo-epidermal
junction; band like distribution • Lymphocytic attack
of basal layer – Bullaeformation • Postinflammatory
hypo/hyperpigmentation
- Puritic, purple, polygonal, planar papules and plaques
Destruction of keratinocytes ,1% pop, middle age
Lymphohistiocytic infiltrate at dermo-epidermal
junction; band like distribution • Lymphocytic attack
of basal layer – Bullaeformation • Postinflammatory
hypo/hyperpigmentation
- Psoriasis
- Common (1-2% pop) inflammatory condition, genetics
• Elbows, knees, scalp, mean onset 25y
Well-demarcated, pink-salmon plaque, silvery scale
Scraping off the scale reveals bleeding points
Microscopically – ↑Epidermal cell turnover – Downward
elongation of rete ridges, thinned epidermis – Dilated
vessels, polymorphs, sterile pustules
- Common (1-2% pop) inflammatory condition, genetics
• Elbows, knees, scalp, mean onset 25y
Well-demarcated, pink-salmon plaque, silvery scale
Scraping off the scale reveals bleeding points
Microscopically – ↑Epidermal cell turnover – Downward
elongation of rete ridges, thinned epidermis – Dilated
vessels, polymorphs, sterile pustules
- Urticaria
- Reaction Pattern of Hives and Wheals
Oedema of dermis: -> erythematous
and/or oedematous papule (Papule:
small elevated skin lesion < 5-10 mm),
Clinically: itching and swelling
Examples: nettles rash, hives
Histology: inflammation, separation
of collagen bundles, eosinophils,
mast cells, histamine, IgE
- Reaction Pattern of Hives and Wheals
Oedema of dermis: -> erythematous
and/or oedematous papule (Papule:
small elevated skin lesion < 5-10 mm),
Clinically: itching and swelling
Examples: nettles rash, hives
Histology: inflammation, separation
of collagen bundles, eosinophils,
mast cells, histamine, IgE
- Lichen Planus
- Eczema/Dermatitis
- ‘Bubble up / Boil over’ Reaction pattern rather than disease. Common,
10% pop (40% at some point in life) Signs: – Red (erythematous) skin –
Tiny vesicles develop Surface develops scales-> cracking, bleeding ->
discomfort – Skin becomes tender; secondary infection Variation –
Cause: contact, site Effects: Barrier damage Water loss, entry of
allergens Treatment: – Topical creams, steroids
- Underlying pathological processes – Swelling within epidermis
Separation of keratinocytes by fluid accumulation (spongiosis).
Hyperkeratosis: ↑ thickness of stratum corneum Parakeratosis:
retention of nuclei in SC: scales Inflammation: oedema
- Underlying pathological processes – Swelling within epidermis
Separation of keratinocytes by fluid accumulation (spongiosis).
Hyperkeratosis: ↑ thickness of stratum corneum Parakeratosis:
retention of nuclei in SC: scales Inflammation: oedema
- ‘Bubble up / Boil over’ Reaction pattern rather than disease. Common,
10% pop (40% at some point in life) Signs: – Red (erythematous) skin –
Tiny vesicles develop Surface develops scales-> cracking, bleeding ->
discomfort – Skin becomes tender; secondary infection Variation –
Cause: contact, site Effects: Barrier damage Water loss, entry of
allergens Treatment: – Topical creams, steroids
- Blistering (Bullous) Disorders
- Pemphigus
- Rare auto-immune blistering disorder • Middle-aged (40-60y) • Fatal if untreated
– Serum electrolyte loss, infection • Intra-epidermal blister – Location varies with
type • Circulating auto-antibodies (IgG) directed at components of intercellular
bridges w/in epidermis – epidermisfallsapart – loose keratinocytes
- Rare auto-immune blistering disorder • Middle-aged (40-60y) • Fatal if untreated
– Serum electrolyte loss, infection • Intra-epidermal blister – Location varies with
type • Circulating auto-antibodies (IgG) directed at components of intercellular
bridges w/in epidermis – epidermisfallsapart – loose keratinocytes
- Dermatitis herpetiformis
- Young adults (20-40y), rare – Knees, elbows •
Blister at dermo-epidermal junction – Very
pruritic: rarely see intact blister • Associated
with coeliac disease • Granular IgA deposit on
BM
- Young adults (20-40y), rare – Knees, elbows •
Blister at dermo-epidermal junction – Very
pruritic: rarely see intact blister • Associated
with coeliac disease • Granular IgA deposit on
BM
- Bullous Pemphigoid
- Elderly, > 60 yr, 0.7/100,000 • Self- limiting • Blister at
dermo-epidermal junction • Circulating auto-antibodies
(IgG) on BM – Immunofluorescence • Antigen-antibody
complex – Degranulation of mast cells, eosinophils
- Elderly, > 60 yr, 0.7/100,000 • Self- limiting • Blister at
dermo-epidermal junction • Circulating auto-antibodies
(IgG) on BM – Immunofluorescence • Antigen-antibody
complex – Degranulation of mast cells, eosinophils
- Pemphigus
- Epidermal Cell Conditions
- Malignant Epidermal
Neoplasms
- SCC (#2)
- Keratoacanthoma
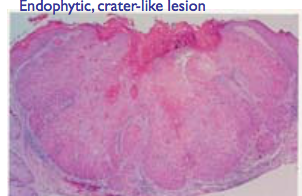
- Variant of SCC • Clinically benign and regresses •
Crater-like symmetrical architecture – Keratin debris
• Most common site is face – Sun damaged skin
- Variant of SCC • Clinically benign and regresses •
Crater-like symmetrical architecture – Keratin debris
• Most common site is face – Sun damaged skin
- Arises from keratinocytes of upper layers of epidermis • Common- 15% skin malignancies •
Locally invasive, metastasise late • Elderly, face, hands, M>F – Chronic sun exposure, in situ
lesions – Chemicals eg tar, oil, ionising-irradiation • Grossly – Roughened keratotic areas,
papules, nodules, ulcers or horns • Histologically – Disorganised keratinocytes, malignant
cytology • T reatment – Surgical excision, more resistant to radiotherapy than BCC
- Keratoacanthoma
- BCC (#1)
- • Arises from basal keratinocytes of epidermis • Common,70% skin malignancies • Slow growing,
locally very invasive, rarely metastasise • Face, elderly, pale skin – Chronic sun exposure • Grossly –
Ulcerated irregular lesion, raised pearly border (Rodent ulcer) – Prominent, dilated blood vessels
(telangectasia) • Histological – Clumps of cells surrounded by rim of cells with nuclei line up like a
picket fence (palisading). • Treatment – Local excision +/- radiotherapy
- • Arises from basal keratinocytes of epidermis • Common,70% skin malignancies • Slow growing,
locally very invasive, rarely metastasise • Face, elderly, pale skin – Chronic sun exposure • Grossly –
Ulcerated irregular lesion, raised pearly border (Rodent ulcer) – Prominent, dilated blood vessels
(telangectasia) • Histological – Clumps of cells surrounded by rim of cells with nuclei line up like a
picket fence (palisading). • Treatment – Local excision +/- radiotherapy
- SCC (#2)
- Benign Epidermal
Neoplasms
- Skin tags
- – Fibroepithelial polyp,
friction -Pedunculated, benign
- – Fibroepithelial polyp,
friction -Pedunculated, benign
- Squamous cell papilloma
- -HPV
-Verrucae/warts
- -HPV
-Verrucae/warts
- Seborrhoeic wart / keratosis
- Keratosis = excess keratin] • Basal cell papilloma (benign)
• Proliferation of cells that resemble basal cells •
Common in elderly, trunk – extremities, head, neck •
Rarely become malignant • Keratin-filled plugs, cysts •
Exophytic, coin-like plaques – ‘stuck-on’ appearance –
Dark, greasy-looking irregular
- Keratosis = excess keratin] • Basal cell papilloma (benign)
• Proliferation of cells that resemble basal cells •
Common in elderly, trunk – extremities, head, neck •
Rarely become malignant • Keratin-filled plugs, cysts •
Exophytic, coin-like plaques – ‘stuck-on’ appearance –
Dark, greasy-looking irregular
- Skin tags
- Pre-Malignant Epidermal
Neoplasms
- Squamous cell carcinoma is preceded by series of progressive
dysplastic changes – chronic exposure to sunlight – hyperkeratosis
– > Actinic (sun-related) keratosis • > 1 cm, tan-brown / red, rough
(sandpaper) • Hyperplasia of basal cells • Solar elastosis (blue-grey
elastic fibres)
- Squamous cell carcinoma is preceded by series of progressive
dysplastic changes – chronic exposure to sunlight – hyperkeratosis
– > Actinic (sun-related) keratosis • > 1 cm, tan-brown / red, rough
(sandpaper) • Hyperplasia of basal cells • Solar elastosis (blue-grey
elastic fibres)
- Malignant Epidermal
Neoplasms
- Melanocytes
- Freckles
(Ephilides)
- • Focal area of increased melanocyte activity •
Common, children, lightly pigmented individuals
• Fade and darken according to sun exposure
- • Focal area of increased melanocyte activity •
Common, children, lightly pigmented individuals
• Fade and darken according to sun exposure
- Lentigo
- • Common, localised, benign hyperplasia of melanocytes
• Skin, mucous membranes • Small, oval, tan-brown
patches • Do not darken in response to sunlight
- • Common, localised, benign hyperplasia of melanocytes
• Skin, mucous membranes • Small, oval, tan-brown
patches • Do not darken in response to sunlight
- Melanocytic Naevi
‘Moles’
- Malignant
Melanoma
- Tumour composed of malignant melanocytes – More correctly ‘melanocarcinoma’ – Skin,
(retina, leptomeninges) • Usually pigmented macules, papules or nodules – Visible from
early stages – Sun exposed surfaces • Excision prior to dermal invasion = cure • Aetiology
– **UV light • episodic, acute exposure with burning, fair skin – Gene mutations •
CDNK2A (TSG)germline, familial melanomas • BRAF / NRAS (oncogenes), somatic
- Can arise from any melanocyte – Expect from benign naevi: larger numbers cells • Post mitotic –
Classes of naevi with active junctional component – De novo • Prognosis – Depends on thickness
(Breslow) – Completely excised non-ulcerated melanoma < 1 mm ~ 100% cure • Clinical course –
Metastatic spread, early in development – Skin, brain, GI – Excise primary lesion
- Can arise from any melanocyte – Expect from benign naevi: larger numbers cells • Post mitotic –
Classes of naevi with active junctional component – De novo • Prognosis – Depends on thickness
(Breslow) – Completely excised non-ulcerated melanoma < 1 mm ~ 100% cure • Clinical course –
Metastatic spread, early in development – Skin, brain, GI – Excise primary lesion
- Lentigomaligna
(15%) Elderly,
face
- Superficial
spreading**(50%) • Flat,
female, leg
- Acrallentiginous (10%) •Palms /
soles of feet, most common
non- Caucasian type
- Nodular (25%) •
Pigmented nodule, may
ulcerate, male, trunk
- Tumour composed of malignant melanocytes – More correctly ‘melanocarcinoma’ – Skin,
(retina, leptomeninges) • Usually pigmented macules, papules or nodules – Visible from
early stages – Sun exposed surfaces • Excision prior to dermal invasion = cure • Aetiology
– **UV light • episodic, acute exposure with burning, fair skin – Gene mutations •
CDNK2A (TSG)germline, familial melanomas • BRAF / NRAS (oncogenes), somatic
- Malignant
Melanoma
- Freckles
(Ephilides)
Medienanhänge
{kind=link}
{kind=link}
Möchten Sie kostenlos Ihre eigenen Mindmaps mit GoConqr erstellen? Mehr erfahren.