8644630
Beschreibung
Mindmap von Fatma Shwaylia, aktualisiert more than 1 year ago
|
|
Erstellt von Fatma Shwaylia
vor fast 8 Jahre
|
|
Ahmad Can't Run
- Muscle Weakness
- Causes of muscle weakness
- Infection
- poliovirus >
poliomylitis
- Lyme disease
- poliovirus >
poliomylitis
- Neurological
- Demyelinating
disorders
- Guillain-Barré
syndrome
- Guillain-Barré
syndrome
- Demyelinating
disorders
- Medications
- Statin>
atorvastatin
(Lipitor)
- Amiodarone
(oral route)
- Statin>
atorvastatin
(Lipitor)
- Electrolyte:
Hyperkalemia
- Genetics
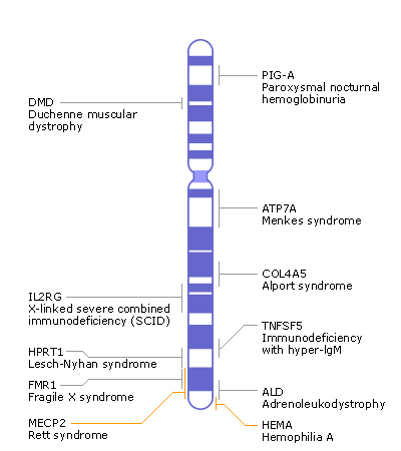
- Duchenne muscular dystrophy
- DMD Gene
- Found on xp21
- 2.2
megabases
- 79 exons
- 8 promoters
- Introns make
up 99.4% of
the entire
gene.
- Mutations
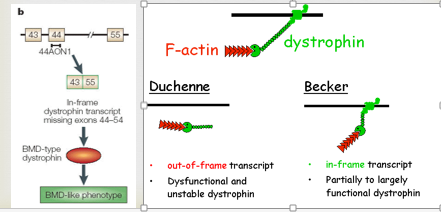
- 60% are deletions
- 5-10% duplications
- 30% point / splice site
modifications
- 60% are deletions
- 2.2
megabases
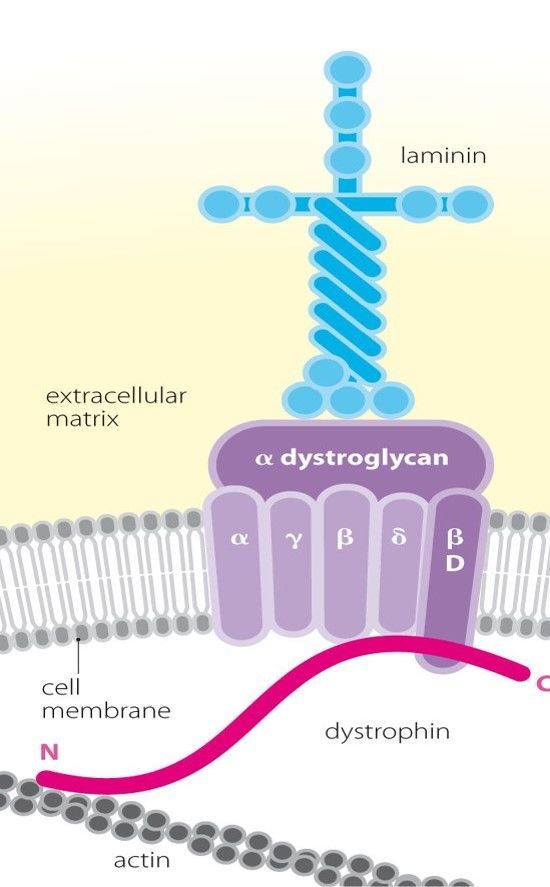
- encodes for the protein
dystrophin, found in muscle
cells and some neurons.
- Dystrophin provides strength to muscle cells by
linking the internal cytoskeleton to the surface
membrane.
- Without this structural
support, the cell membrane
becomes permeable.
- In DMD the damage to muscle
cells is so extreme that the
supply of stem cells are
exhausted and repair can no
longer occur.
- In DMD the damage to muscle
cells is so extreme that the
supply of stem cells are
exhausted and repair can no
longer occur.
- Without this structural
support, the cell membrane
becomes permeable.
- Dystrophin provides strength to muscle cells by
linking the internal cytoskeleton to the surface
membrane.
- Found on xp21
- DMD is a sever progressive X-linked inherited disease
characterized by progressive degeneration of the skeletal
muscle especially those of the shoulder and pelvic griddle.
- clinical features
- Progressive weakness
- Intellectual impairment
- Hypertrophy of the calves
- Proliferation of
connective tissue
in muscle
- Progressive weakness
- A mutation in the gene encoding for dystrophin
protein, which is Xp21 gene.
- Due to loss of dystrophin
- 1-fragile sarcolemma
- Which leads to
- 1-increased osmotic fragility of dystrophic muscles
- 2-exceesive influx of calcium ions
- 3-release of soluble muscle enzymes such as Creatine kinase.
- 4-Necrosis of the muscle cell.
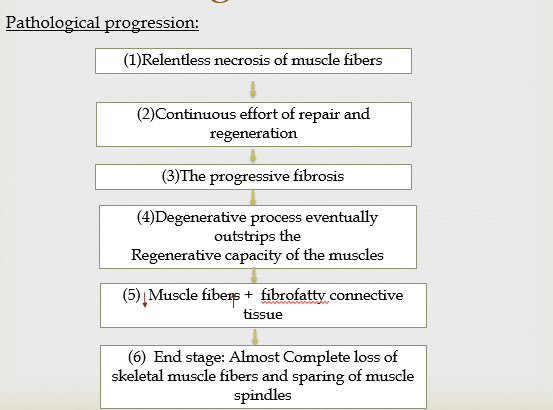
- Pathological progression
- Pathological progression
- 4-Necrosis of the muscle cell.
- 3-release of soluble muscle enzymes such as Creatine kinase.
- 2-exceesive influx of calcium ions
- 1-increased osmotic fragility of dystrophic muscles
- Which leads to
- 2-loss of interaction between
the sarcolemma and
extracellular matrix.
- 3-separation of the
sarcolemma from the
basal lamina.
- Which leads to
- 1-fragile sarcolemma
- Difference between BMD and DMD
- BMD is milder and has low levels of dystrophin due to
- BMD is milder and has low levels of dystrophin due to
- Due to loss of dystrophin
- Clinical progression
- 1-Early
- Infancy
Poor head
control
- Infancy
Poor head
control
- 2-Transitional
- Toddler
- hip weakness
and lordosis
- 3-9 years
- Gower sign and HT of calf.
- Gower sign and HT of calf.
- hip weakness
and lordosis
- Toddler
- 3-Loss of
Ambulatory
- 10-14 years
- Wheel chair
- 10-14 years
- 4-Late
- +15 years
- Respiratory-cardiac-CNS
complications
- +15 years
- 1-Early
- Complications of DMD
- Cardiac
- Arrhythmias
- -Cardiomyopathy
- Arrhythmias
- Orthopaedic problems
- -Joint contractures
- -Osteopenia
–because of
immobility but also
secondary to steroid
treatment
- -Scoliosis
- -Joint contractures
- Infectious
- Pulmonary infections
- Pulmonary infections
- Pulmonary
- Respiratory insufficiency with
decreased total lung capacity,
decreased residual lung volume
- Respiratory insufficiency with
decreased total lung capacity,
decreased residual lung volume
- Cardiac
- With an incidence of one in 5,000 boys,
which are 200 per million births.
- clinical features
- Investigations
- Serum Creatine Kinase
- used to detect i (myositis) or
(myopathies) such as muscular
dystrophy
- A high CK generally indicates
that there has been some recent
muscle damage but will not
indicate its location or cause.
- to detect if Ahmad has any
muscular disorder since he already
had muscle weakness and pain.
- to detect if Ahmad has any
muscular disorder since he already
had muscle weakness and pain.
- A high CK generally indicates
that there has been some recent
muscle damage but will not
indicate its location or cause.
- used to detect i (myositis) or
(myopathies) such as muscular
dystrophy
- Electromyography
- is a diagnostic procedure to assess the
health of muscles and the nerve cells
that control them (motor neurons).
- EMG translates electrical signals
of our muscles into graphs, sounds
or numerical values
- The doctor has ordered electromyography
because Ahmad was complaining of muscle
tenderness and weakness.
- The doctor has ordered electromyography
because Ahmad was complaining of muscle
tenderness and weakness.
- EMG translates electrical signals
of our muscles into graphs, sounds
or numerical values
- is a diagnostic procedure to assess the
health of muscles and the nerve cells
that control them (motor neurons).
- Thyroid Function Test
- blood tests that
determine the function
of the thyroid gland
- by measuring : TSH
, thyroid-stimulating
hormone (TSH) thyroid
hormone levels, thyroxine
(T4) and triiodothyronine (T3)
- Since Ahmad had muscle weakness,
the doctor wanted to check thyroid
hormones levels since they affect
many conditions in our bodies
including muscle strength
- Since Ahmad had muscle weakness,
the doctor wanted to check thyroid
hormones levels since they affect
many conditions in our bodies
including muscle strength
- by measuring : TSH
, thyroid-stimulating
hormone (TSH) thyroid
hormone levels, thyroxine
(T4) and triiodothyronine (T3)
- blood tests that
determine the function
of the thyroid gland
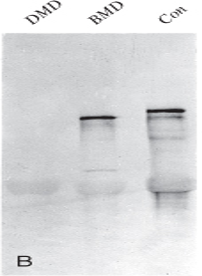
- Western Blot
- to detect and analyze proteins
- Since the doctor was suspecting DMD, he
wanted to make sure that the dystrophin
enzyme is absent .Compared it with BMD to
see how BMD is a milder form that has low
dystrophin
- Since the doctor was suspecting DMD, he
wanted to make sure that the dystrophin
enzyme is absent .Compared it with BMD to
see how BMD is a milder form that has low
dystrophin
- to detect and analyze proteins
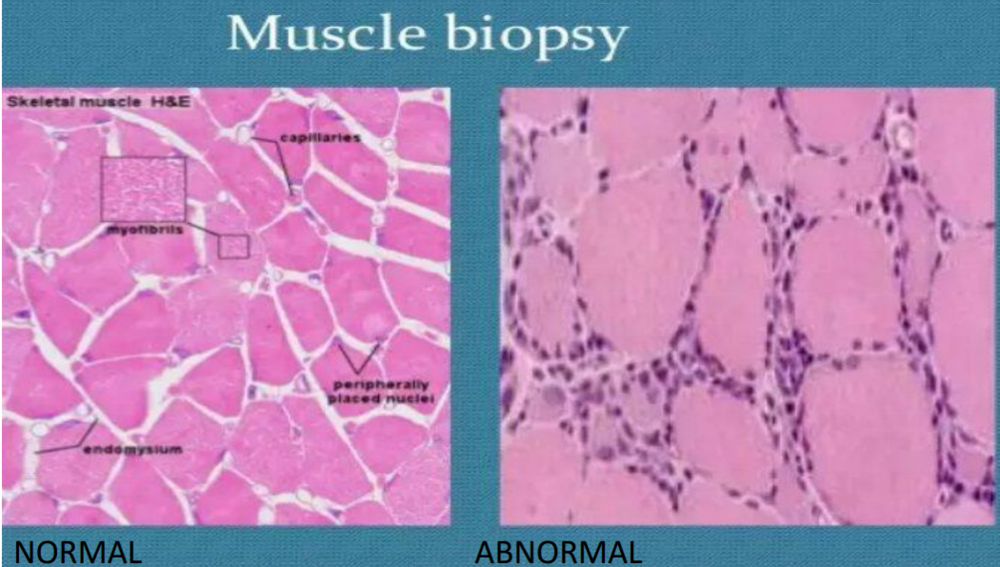
- Muscle Biopsy
- Shows myopathic changes
such as; connective tissue
proliferation, scattered
degenerating and
regenerating myofibres
- Shows myopathic changes
such as; connective tissue
proliferation, scattered
degenerating and
regenerating myofibres
- Serum Creatine Kinase
- Management
- Pharmacological
- Corticosteroids such as
prednisone, can help improve
muscle strength
- Heart medications, such as
angiotensin-converting enzyme (ACE)
inhibitors or beta blockers, if muscular
dystrophy damages the heart.
- For controlling the
asthma
exacerbation
Albuterol is used.
- Corticosteroids such as
prednisone, can help improve
muscle strength
- Non pharmcological
- Physical and
occupational
therapy
- Gene therapy
- Stem cell
- Physical and
occupational
therapy
- Pharmacological
- Prognosis
- death occurs usually at about 18-20yrs of age
- The causes of death
- Respiratory failure
- Heart failure
- Pneumonia
- Aspiration
- Airway obstruction.
- Respiratory failure
- The causes of death
- dystrophy leads to progressively worsening disability
- death occurs usually at about 18-20yrs of age
- DMD Gene
- Duchenne muscular dystrophy
- Metabolic
- Glycogenoses: Acid
maltase deficiency
- Glycogenoses: Acid
maltase deficiency
- Infection
- History taking for
muscle weakness
- Introduction
- Greeting the
patient, insure
privacy
- Greeting the
patient, insure
privacy
- Duration
&Location
- progression
- Radiation
- Quality (Pain Scales
/questionnaire) &
Quantity
- Aggravating
factors
&Alleviating
factors
- Associated symptoms
- History of medication
- Family history
- Muscle Strength Scale
- Introduction
- Neurological Examination of lower limb
- Motor system
- Fasciculations and
muscle wasting
- Tone
- Clonus
- Power at
hip, knee,
ankle, and
tarsal joints
- Coordination
- Heel–shin test
- Toe–finger test
- Heel–shin test
- Fasciculations and
muscle wasting
- Sensory System
- Dermatomes
- The
superficial or
cutaneous
reflexes
- Dermatomes
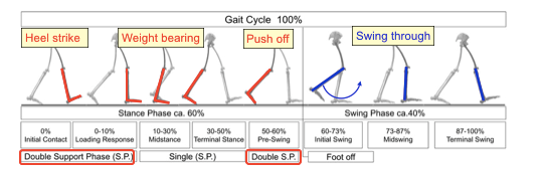
- Gait
- Gait Cycle
- stance phase
- begins with
heel strike
and ends
with push
off from the
forefoot
- begins with
heel strike
and ends
with push
off from the
forefoot
- swing phase
- begins after push
off when the toes
leave the ground
and ends with the
heel strike.
- begins after push
off when the toes
leave the ground
and ends with the
heel strike.
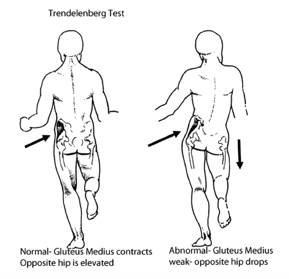
- Abnormalities
- inadequate abductor
muscles of the hip.
- Lateral trunk bending
(Trendelenburg gait, gluteus
medius gait.)
- Lateral trunk bending
(Trendelenburg gait, gluteus
medius gait.)
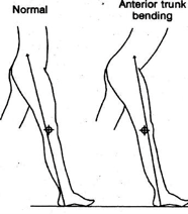
- Forward flexion of the trunk early in the
stance phase. Compensates for
inadequacy of the knee extensors.
- Anterior trunk bending
- Anterior trunk bending
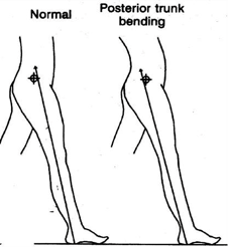
- Backward movement of the
trunk early in the stance phase.
Compensates for inadequacy of
hip extensors.
- Posterior trunk bending
(Gluteus maximus (Lurch)
gait)
- Posterior trunk bending
(Gluteus maximus (Lurch)
gait)
- The legs are not different in length when
measured but are unable to adjust to the
appropriate length during the gait cycle.
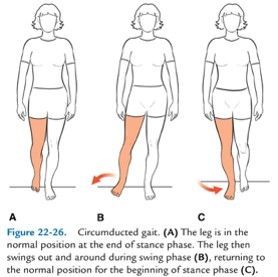
- The long limb is circumducted
during the swing phase.
Circumduction may also be used
to advance the swinging leg in the
presence of weak hip flexors
- Swing-out gait (circumduction gait)
- Swing-out gait (circumduction gait)
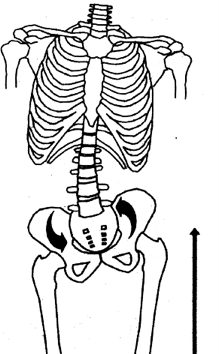
- The pelvis is lifted on the side
of the swinging leg (normal) by
contraction of the spinal
muscles and the lateral
abdominal wall.
- Hip hiking
- Hip hiking
- Exaggerated hip and knee
flexion to lift the foot higher
than usual for increased
ground clearance.
- Steppage gait
- Steppage gait
- Going up on the toes of the stance
phase leg. Results in exaggerated
upward movement of the trunk.
Seen in Weak hamstring
- Vaulting
- Vaulting
- A rhythmic
disturbance in which
as short a time is
possible is spent on
the painful limb, and a
correspondingly
longer time is spent
on the pain-free side.
- Antalgic gait
- Antalgic gait
- In parkinsonism
- Shuffling gait
- Shuffling gait
- A rhythmic disturbance
where the timing alters
from one step to the next.
Also occurs in drunk
people.
- Ataxic gait
- Ataxic gait
- The long limb is circumducted
during the swing phase.
Circumduction may also be used
to advance the swinging leg in the
presence of weak hip flexors
- inadequate abductor
muscles of the hip.
- stance phase
- Gait Cycle
- Motor system
- Causes of muscle weakness
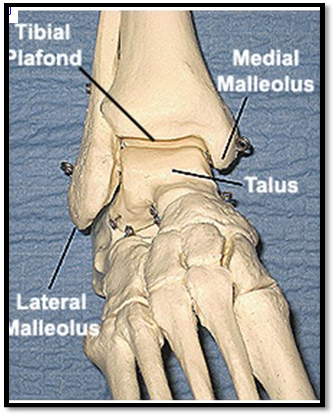
- Foot and ankle joint
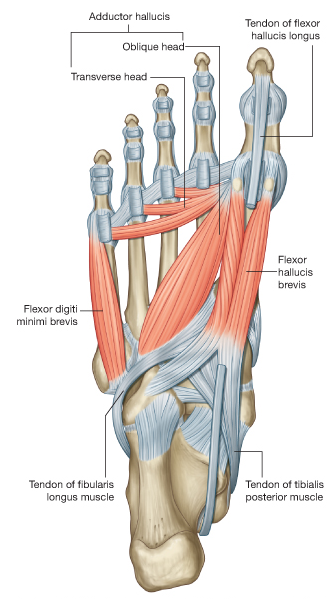
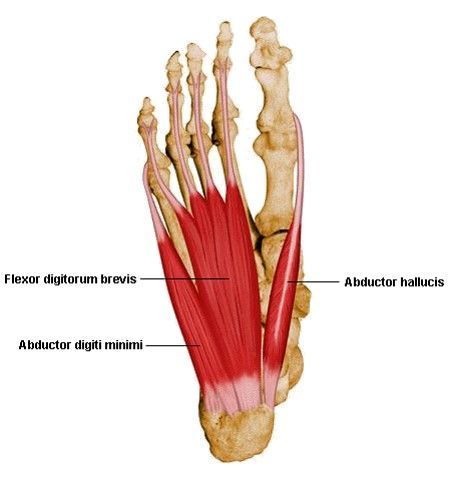
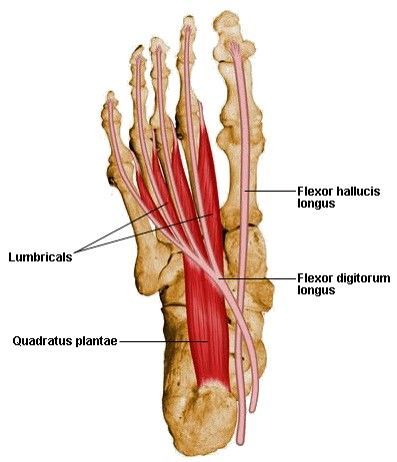
- Foot Anatomy
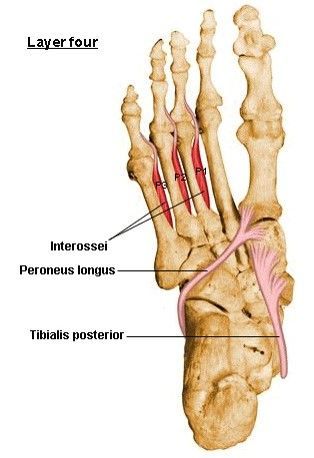
- Muscles
- Layer 1
- Layer 2
- Layer 3
- Layer 4
- Muscle
Development
nutrients
- Calcium
- Iron
- Vitamin D
- Magnesium
- Vitamin B12
- Zine
- Omega 3
- Vitamin C
- Vitamin
B1
- Proteins
- Calcium
- Layer 1
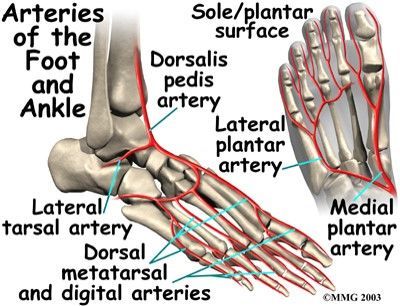
- Arteries
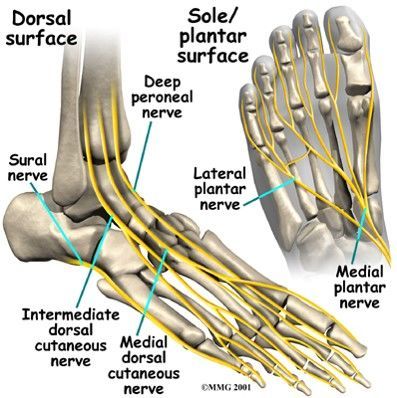
- Nerves
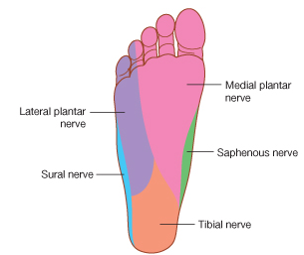
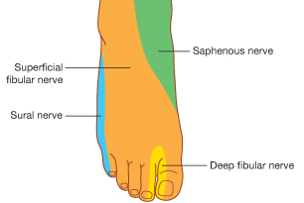
- sensory nerve supply of the foot
- sensory nerve supply of the foot
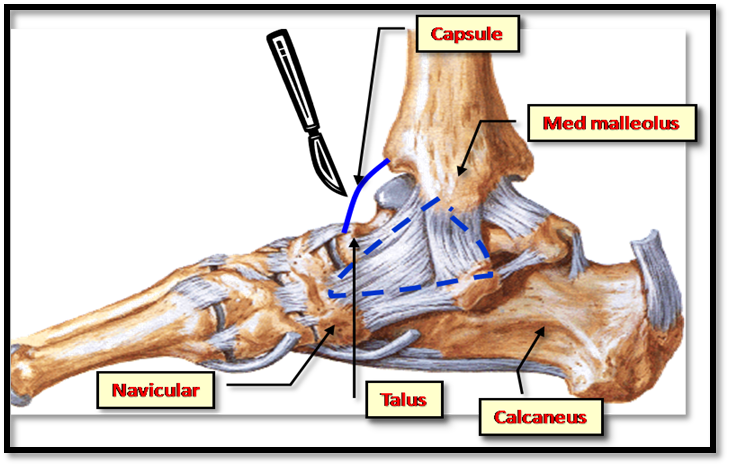
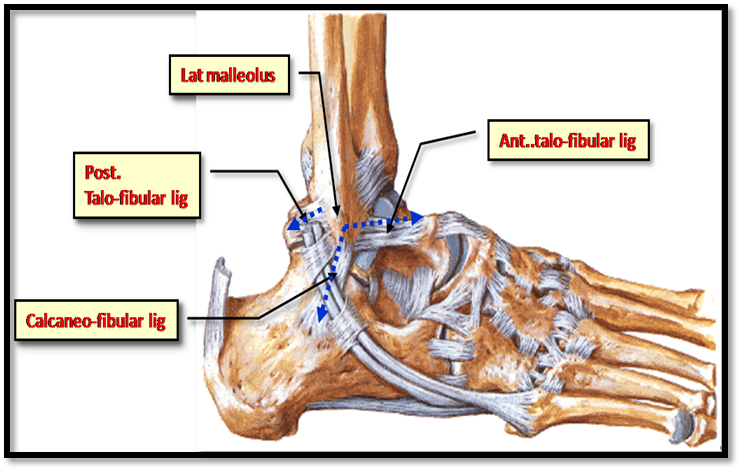
- Ligaments
- Ankle
Joint
- Bones
- Muscles
- Physical examination for
- Introduction & Consent
- HEPA
- HEPA
- Inspection
- Palpation
- Skin
Temperature
Joints
Tendons
Ligaments
- Move
- Dorsiflexion
- Plantar
Flexion
- Inversion
- Eversion
- flexion of
the great
toe
- special tests
- Inversion and
Eversion
stress test
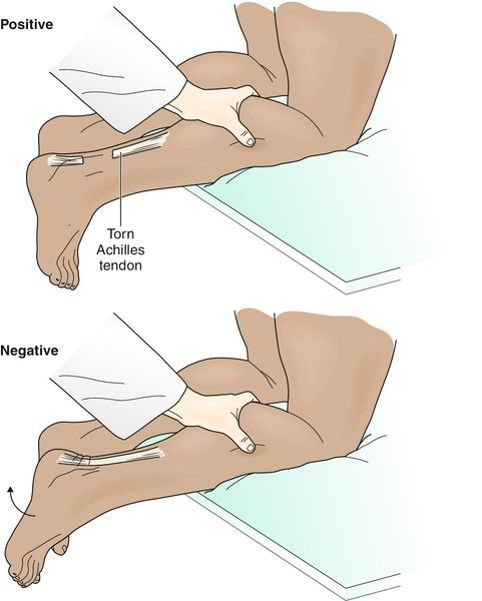
- Thompson’s
test
- for
tendoachillies
rupture
- for
tendoachillies
rupture
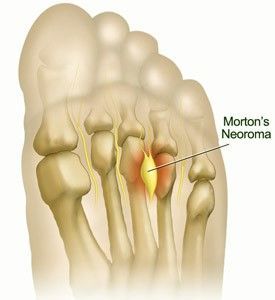
- Tests
for
Morton’s
metatarsalgia
- Inspect the footwear
- Inspect the footwear
- Test Gait
- Drapes the patient
- DR.TH
- DR.TH
- Inversion and
Eversion
stress test
- Dorsiflexion
- Skin
Temperature
Joints
Tendons
Ligaments
- SSSP
- Palpation
- Introduction & Consent
- Foot Anatomy
Medienanhänge
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Möchten Sie kostenlos Ihre eigenen Mindmaps mit GoConqr erstellen? Mehr erfahren.