NDBE Oral Path Karteikarten am Diseases of Gnathic bones and TMJ, erstellt von Laura Gennaro am 21/01/2018.
|
|
Erstellt von Laura Gennaro
vor fast 7 Jahre
|
|
Schließen
|
|
Erstellt von Laura Gennaro
vor fast 7 Jahre
|
|
Idiopathic Osteosclerosis
(Enostosis, dense bone island)
Reported prevelance of idiopathic osteosclerosis
Condensing/sclerosing osteitis
Cherubism
Hypophosphatasia
Odontophosphatasia
Clinical features of hypophosphatasia
Nasopalatine duct cyst (incisive canal cyst)
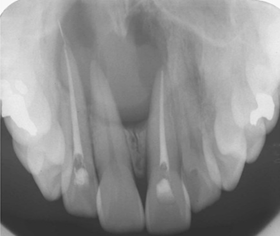
Paired incisive canals open into a single incisive foramen & transmit...
Nasopalatine duct cyst arieses from...
Nasaopalatine duct cyst differential diagnosis
Nasopalatine duct cyst management
Cyst of the incisive papilla
Surgical ciliated cyst
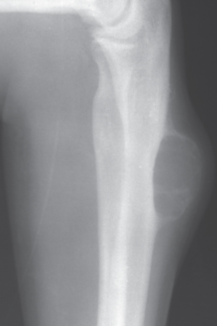
Simple bone cyst (traumatic bone cyst, idiopathic bone cavity)

Epidemiology of Simple bone cysts
Gnathic Simple Bone Cyst
Differential diagnosis of Gnathic simple bone cyst
Central Giant Cell Granuloma (CGCG)
Aggressive CGCGs characterized by...
Management & Prognosis of CGCG
Recurrent CGCG lesions
Aneurysmal bone cyst
Epidemiology of Aneurysmal Bone Cyst (ABC)
Gnathic ABC
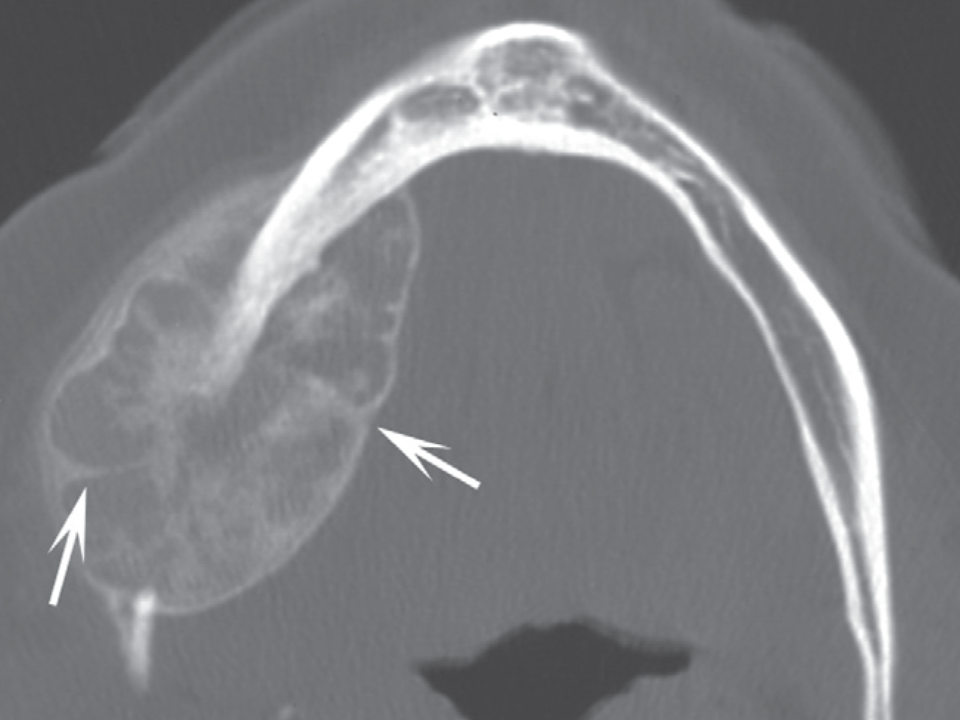
ABC clinical differential diagnosis
Management & Prognosis
Hematopoietic bone marrow defect
Myospherulosis
Cause of Myospherulosis
Presentation
Treatment
Osteonecrosis (avascular necrosis)
Medication related osteonecrosis of teh jaws (MRONJ)
What are bisphosphonates?
When are bisphosphonates administered?
IV bisphosphonates every 3-4 weeks for bone metastases
(zoledronate/zometa; pamidronate/aredia)
IV bisphosphonates once yearly for osteoporosis
(zoledronate/reclast)
Oral bisphosphonates taken daily/weekly/monthly for osteoporosis
(alendronate/fosamax; risedronate/actonel; ibandronate/bonvia)
What is denosumab?
When is denosumab administered?
Subcutaneous administration of denosumab every 6months for osteoporosis
(Prolia)
Subcutaneous administration of denosumab every 4 weeks for bone metastases
(Xgeva)
MRONJ Risk Factors: site
MRONJ Risk Factors: Duration of dose
MRONJ Risk Factors: Age
MRONJ: Other risk factors
Diagnosis of MRONJ
Stage 0 MRONJ
S
Stage 2 MRONJ
Stage 3 MRONJ
Treatment of MRONJ
MRONJ & dental considerations
Osteoradionecrosis
Osteoradionecrosis of the jaws
Majority of Osteoradionecrosis of the Jaws occur...
Management of Osteoradionecrosis of the jaws
Prevention represents best course of action (Osteoradionecrosis)
Spontaneous sequestration (osteonecrosis)
Other causes of osteonecrosis
Fibrous dysplasia
Fibrous dysplasia manifestation
Fibrous dysplasia variable phenotypic expressions
Monostotic FD (85-90%)
Fibrous dysplasia variable phenotypic expressions
Polyostotic FD (10-15%)
Fibrous dysplasia variable phenotypic expressions
McCune-Albright Syndrome (<5%)
Extent of disease (FD) correlates w
Radiographic appearance of FD
Craniofacial fibrous dysplasia
Fibrous dysplasia Diagnosis & Management
Cemento-ossifying fibroma
Cemento-ossifying fibroma Radiographic appearance
Aggressive (juvenile) ossifying fibromas
-Trabecular ossifying fibroma
Aggressive (juvenile) ossifying fibromas
-Psammomatoid ossifying fibroma
Gigantiform cementoma
Cemento-osseous dysplasia
Cemento-osseous dysplasia
Takes months/years to develop & radiographic appearance depends on maturity of lesion
Cemento-osseous dysplasia most frequently occurs in...
Periapical COD
Focal COD
Multifocal COD
Florid COD
Management of COD
Osteoma
Osteoma Diagnosis
Bones/areas affected by Osteoma
Osteoid osteoma & osteoblastoma
Osteoid Osteoma
Osteoblastoma
Osteosarcoma
Osteosarcoma survival
Osteosarcoma of Gnathic bones
What percent of mandibular and maxillary osteosarcomas recur
Radiographic appearance of Gnathic Osteosarcoma
Osteosarcoma, Codman triangle, & 'sunburst' appearance
Surface osteosarcomas
Periosteal osteosarcoma
Parosteal osteosarcoma
Chondrosarcoma
Chondrosarcoma statistics
Chondrosarcoma Precursor lesions
Low/intermediate grade Chondrosarcoma
High-grade chondrosarcoma
Mesenchymal chondrosarcoma
Metastases to gnathic bones
Radiographic appearance of metastatic disease
Synovial Chondromatosis
Synoviuim
Treatment of Synovial chondromatosis
Synovial Chondromatosis characteristics


