10816494
Beschreibung
Karteikarten von Jonathan Cash, aktualisiert more than 1 year ago
|
|
Erstellt von Jonathan Cash
vor etwa 7 Jahre
|
|
| Frage | Antworten |
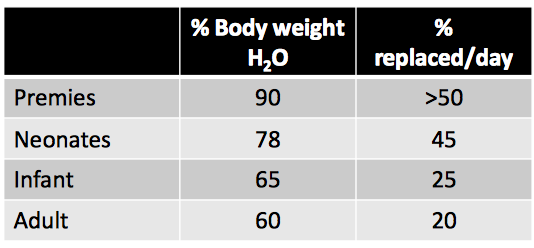
| Children and water | |
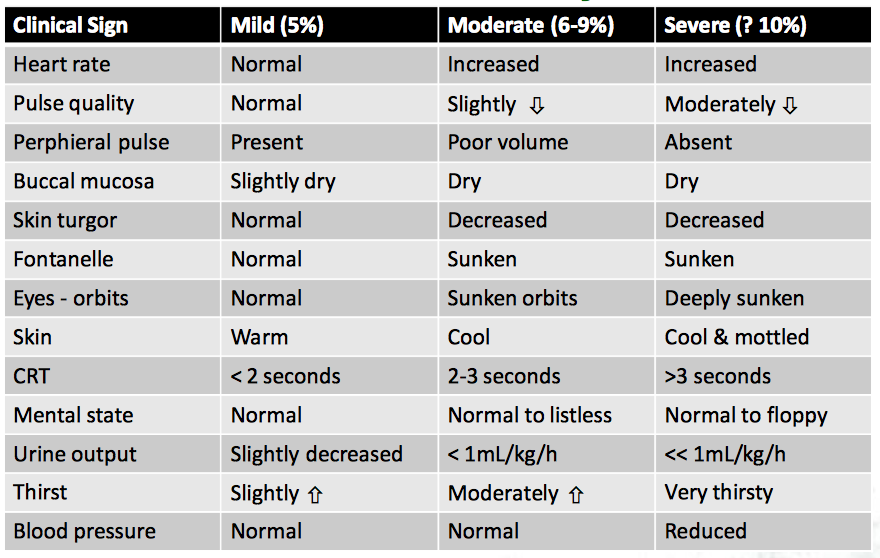
| Presentation of Dehydration | |
| Management | •Where possible oral rehydration therapy is preferable • Assess BGL and manage hypoglycaemia 2 mL/kg of 10% glucose • If IV fluid replacement indicated10-20mL/kg as a bolus • Boluses of IV fluids should be given as an IV push • Consider calculating fluid deficit • Fluid deficit = % loss of body weight x body weight • ? need for oral paracetamol for pain and pyrexia: 20mg/kg • Consider the need for ondansetron: 0.1mg/kg IV |
| Estimation of weight (kg) | • ≤ 12 months: 5kg • 1- 9 years: (age in years +4)x2 • 10-14 years: age in years x 3 |
| Some consideration of A and P | • Infant more dependant on heart rate for cardiac output • Less able to increase contractility of heart due to less actomyosin filaments, fewer mitochondria and smaller myocardial nor- adrenaline stores • Ventricle less compliant needing higher atrial pressures for ventricular filling • More dependent on extracellular concentration of Ca2+ • Storage and release of Ca2+ from myocardial sacroplasmic reticulum is less efficient • Total body water and ECF proportionally greater in first six months |
| Some consideration of A and P (b) | • Renal blood flow and glomerular filtration rate is less per unit BSA • Infant kidney less able to concentrate urine and handle Na+ load • Infant less able to acidify urine reducing ability to compensate for hyperchloraemic acidosis 2o to over infusion of Cl- • Infant tolerates more tachycardia and hypotension than adult • The capacity of the heart and brain for anaerobic metabolism is greater than adult • Limited glycogen stores exists hence hypoglycaemia develops readily in the physiologically stressed child • Less underlying co-morbidities and disease state |
{kind=link}
{kind=link}
Möchten Sie mit GoConqr kostenlos Ihre eigenen Karteikarten erstellen? Mehr erfahren.