29172825
Beschreibung
Karteikarten von Cyrielle Saba, aktualisiert more than 1 year ago
|
|
Erstellt von Cyrielle Saba
vor mehr als 3 Jahre
|
|
| Frage | Antworten |
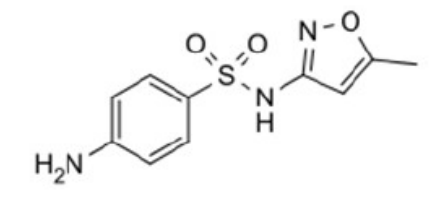
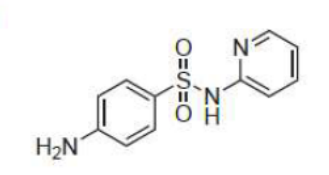
| Sulfamethoxazole Sulfonamide (bacteriostatic, compete with PABA, gram+ and -, treat UTI, orally, well absorbed from GI, PPB, deactivation by phase 2 glucu and acetylation in liver, kidney excretion, SJS, haemopoietic disorder, not for pregnancy, combined with pyrimethamine+folinic acid to treat toxoplasmosis) short/intermediate acting (6-10h) synergistic combination with trimethoprim (less resistance, oral treatment of UTI, acute exacerbations of chronic bronchitis, SE are rash , N&V) | |
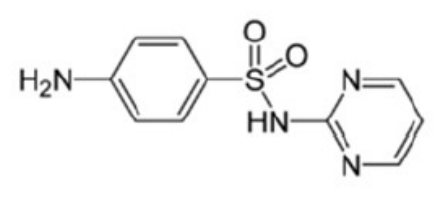
| Sulfadiazine (silver) Topical sulfonamide (bacteriostatic, compete with PABA, gram+ and -, treat UTI, well absorbed from GI, PPB, deactivation by phase 2 glucu and acetylation in liver, kidney excretion, SJS, haemopoietic disorder, not for pregnancy, combined with pyrimethamine+folinic acid to treat toxoplasmosis) short/intermediate acting (7-17h) topical antibiotic used in burns to prevent infection | |
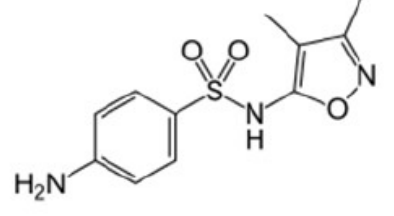
| Sulfisoxazole Sulfonamide (bacteriostatic, compete with PABA, gram+ and -, treat UTI, orally, well absorbed from GI, PPB, deactivation by phase 2 glucu and acetylation in liver, kidney excretion, SJS, haemopoietic disorder, not for pregnancy, combined with pyrimethamine+folinic acid to treat toxoplasmosis) short/intermediate acting (6-10h) | |
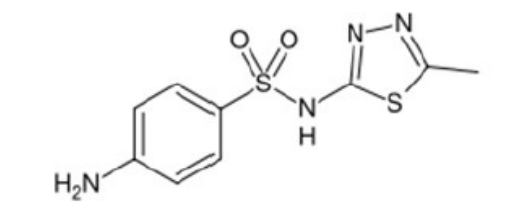
| Sulfamethizole Sulfonamide (bacteriostatic, compete with PABA, gram+ and -, treat UTI, orally, well absorbed from GI, PPB, deactivation by phase 2 glucu and acetylation in liver, kidney excretion, SJS, haemopoietic disorder, not for pregnancy, combined with pyrimethamine+folinic acid to treat toxoplasmosis) short/intermediate acting (6-10h) | |
| Sulfacetamide Topical sulfonamide (bacteriostatic, compete with PABA, gram+ and -, treat UTI, well absorbed from GI, PPB, deactivation by phase 2 glucu and acetylation in liver, kidney excretion, SJS, haemopoietic disorder, not for pregnancy, combined with pyrimethamine+folinic acid to treat toxoplasmosis) 10% topical lotion to treat acne and seborrheic dermatitis | |
| Sulfadoxine Sulfonamide (bacteriostatic, compete with PABA, gram+ and -, treat UTI, orally, well absorbed from GI, PPB, deactivation by phase 2 glucu and acetylation in liver, kidney excretion, SJS, haemopoietic disorder, not for pregnancy, combined with pyrimethamine+folinic acid to treat toxoplasmosis) Ultra-long acting (7-10 days) used with pyrimethamine to treat malaria (but high resistance) | |
| Sulfasalazine Sulfonamide (bacteriostatic, compete with PABA, gram+ and -, treat UTI, orally, well absorbed from GI, PPB, deactivation by phase 2 glucu and acetylation in liver, kidney excretion, SJS, haemopoietic disorder, not for pregnancy, combined with pyrimethamine+folinic acid to treat toxoplasmosis) prodrug: reductive metabolism by gut bacteria-->converts it to sulfapyridine and 5-ASA (mesalamine) | |
| Mesalamine (5-ASA) from Sulfasalazine anti-inflammatory agent low gut absorption to treat ulcerative colitis and Crohn's disease | |
| Sulfapyridine from Sulfasalazine Antibiotic | |
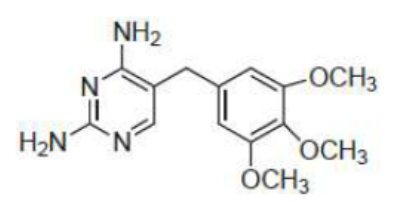
| Trimethoprim diaminopyrimidine derivative antimetabolite (compete with dihydrofolic acid on dihydrofolate reductase) (bacteriostatic) - oral / IV inhibits reduction of DHF to THF-->inhibits bacterial DNA synthesis bigger affinity for DHFR used as single agent for oral treatment of uncomplicated UTI + anaerobic infections low protein binding SE: folate deficiency-->megaloblastic anaemia (reversed by folinic acid supplement), rash, nausea synergistic combination with sulfamethoxazole: less resistance, oral treatment of UTI, acute exacerbations of chronic bronchitis, SE are rash , N&V | |
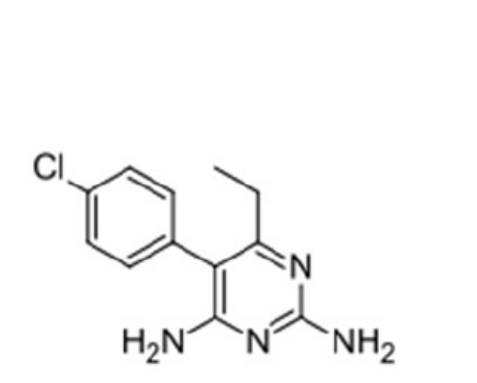
| Pyrimethamine diaminopyrimidine derivative compete with dihydrofolic acid on dihydrofolate reductase inhibits reduction of DHF to THF-->inhibits bacterial DNA synthesis orally bioavailable highly plasma protein bound given with a sulfonamide and folinic acid (bcz can cause megaloblastic anemia) to treat toxoplasmosis combined with sulfadoxine to treat malaria (but high resistance) combined with dapsone to treat and prevent pneumonia | |
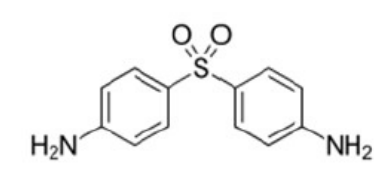
| Dapsone same MOA as sulfonamides (compete with PABA) combined with rifampicine and clofazimine to treat leprosy orally available highly plasma protein bound combined with Pyrimethamine to treat and prevent pneumonia | |
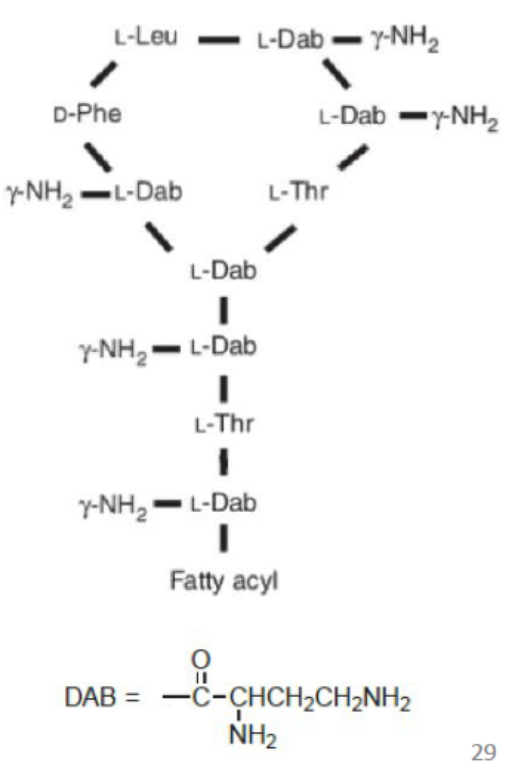
| Polymixin B bactericidal against gram - only binds to phosphate groups in bacterial cytoplasmic membranes-->membranes become permeable-->leakage of cellular molecules-->bacterial death non specific for cell membranes of any type, highly toxic--> NM blockade-->respiratory paralysis at high dose Neuro and nephrotoxicity (due to renal excretion) is used IM or IV as sulfate salt (last resort only) given topically (few SE) | |
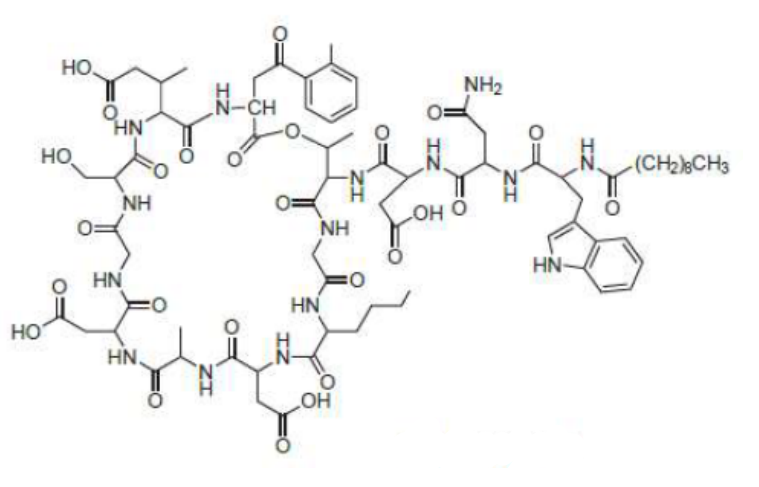
| Daptomycin cyclic lipopeptide binds to cell membranes and causes depolarization-->interrupts protein, DNA and RNA synthesis bactericidal resistance can be achieved in vitro but slow in the clinic potent against gram+ infections (MRSA and VRE too) IV over 30 mins or more SE: dose dependent myopathy due to elevated serum creatine phosphokinase renal elimination | |
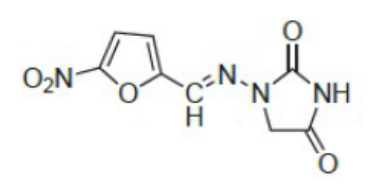
| Nitrofurantoin Nitrofuran derivative active against some gram+ and - bacteria Prodrug bactericidal oral, renally excreted concentrated in urine-->for prophylaxis/treatment of acute urinary tract infections when kidney function is not impaired t1/2=0.5h (short) SE: N&V, acute pulmonary reactions, peripheral neuropathy, hemolytic anemia, liver toxicity, fertility impairment | |
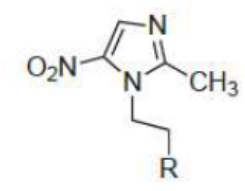
| Metronidazole orally to treat vaginal infections Prodrug by reduction of nitro group-->metabolites interfere with DNA and RNA function-->cell death parenterally to treat anaerobic infections and to treat pseudomembranous colitis due to Clostridium difficile SE: disulfiram-like adverse reactions with alcohol, allergic rashes, CNS disturbances | |
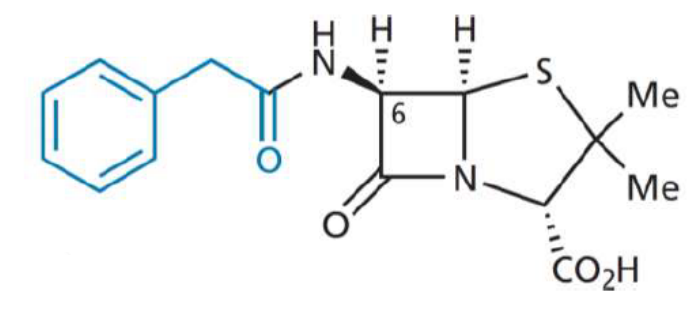
| Penicillin G Benzylpenicillin from phenylacetic acid narrow spectrum of activity sensitive to B lactamase hydrophobic-->gram +, serum protein binding-->protection but less effective bactericidal concentration (t1/2 not affected) EDG-->acid sensitive (less acid stable than Pen V)-->cannot be taken orally depot injection with procaine/benzathine aminoglycosides+B lactams=synergism EXCEPT PENICILLINS | |
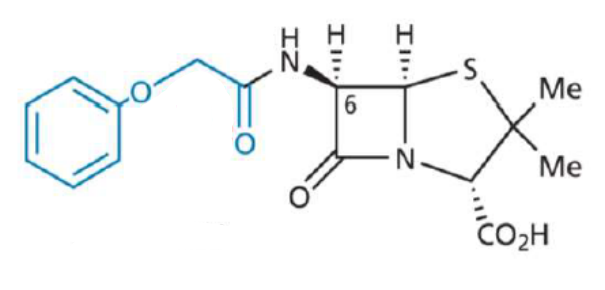
| Penicillin V Phenoxymethyl penicillin from phenoxyacetic acid narrow spectrum of activity sensitive to B lactamase hydrophobic-->gram +, serum protein binding-->protection but less effective bactericidal concentration (t1/2 not affected) EWG-->acid stable-->orally aminoglycosides+B lactams=synergism EXCEPT PENICILLINS | |
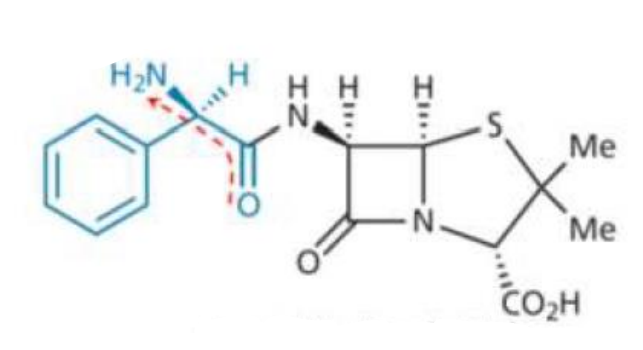
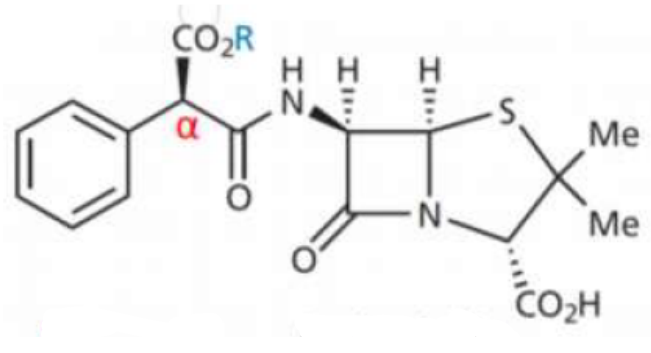
| Ampicillin Aminopenicillin a-aminobenzyl penicillin EWG-->acid stable-->orally B lactamase sensitive (more than PenG) hydrophilic-->active against gram+ (similar to Pen G) and gram - inactive against pseudomonas change gut flora at high doses-->diarrhea NH2 and COOH are ionized-->poor gut absorption; prodrugs (Pivampicillin, Talampicillin, Bacampicillin) have COOR-->better absorption aminoglycosides+B lactams=synergism EXCEPT PENICILLINS | |
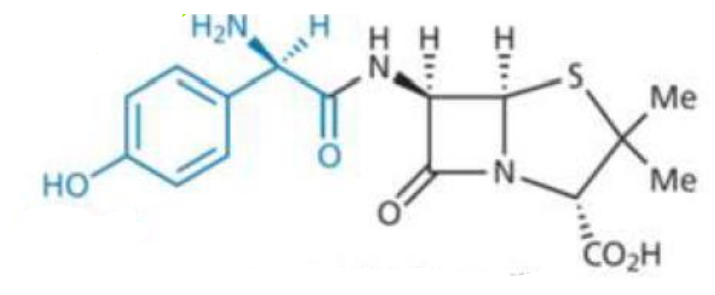
| Amoxicillin Aminopenicillin a-amino-p-hydroxybenzyl penicillin EWG-->acid stable-->orally B lactamase sensitive (more than PenG) hydrophilic-->active against gram+ (similar to Pen G) and gram - inactive against pseudomonas change gut flora at high doses-->diarrhea NH2 and COOH are ionized-->poor gut absorption aminoglycosides+B lactams=synergism EXCEPT PENICILLINS | |
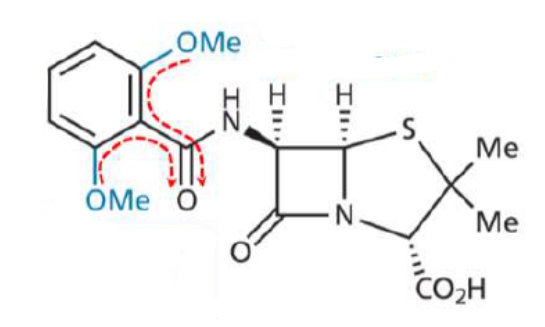
| Methicillin 2,6-dimethoxyphenyl penicillin EDG-->acid sensitive (more than Pen G)-->not orally-->injection Beta lactamase resistant hydrophobic-->gram+, serum protein binding-->protection but less effective bactericidal concentration (t1/2 not affected) Nephritis aminoglycosides+B lactams=synergism EXCEPT PENICILLINS | |
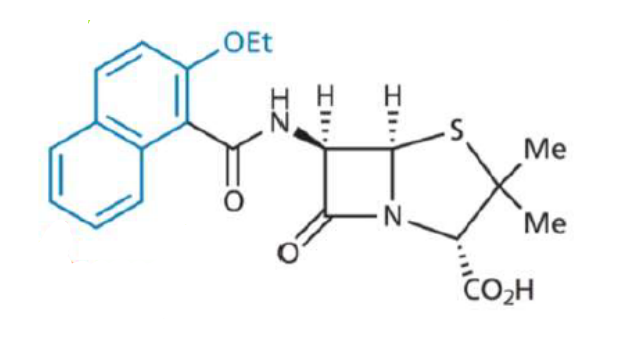
| Nafcillin EWG-->acid stable-->orally Beta lactamase resistant hydrophobic-->gram+, serum protein binding-->protection but less effective concentration (t1/2 not affected) aminoglycosides+B lactams=synergism EXCEPT PENICILLINS | |
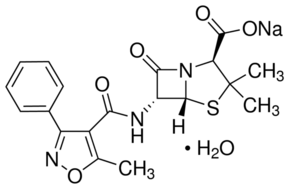
| Oxacillin EWG-->acid stable-->orally bulky-->B lactamase resistant active against resistant strains of s.aureus lipophilic-->inactive against gram-, serum protein binding-->protection but less effective bactericidal concentration (t1/2 not affected) aminoglycosides+B lactams=synergism EXCEPT PENICILLINS | |
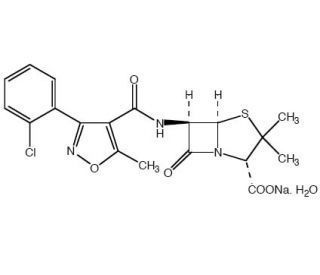
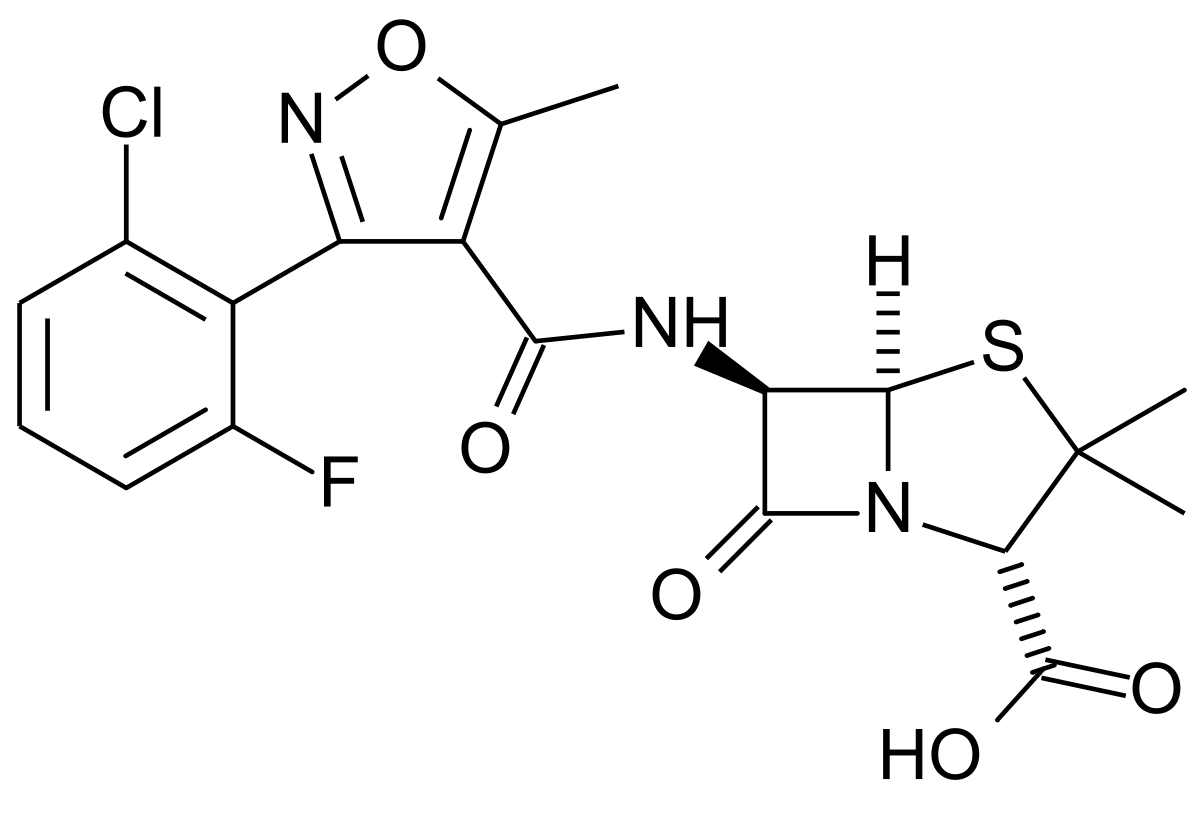
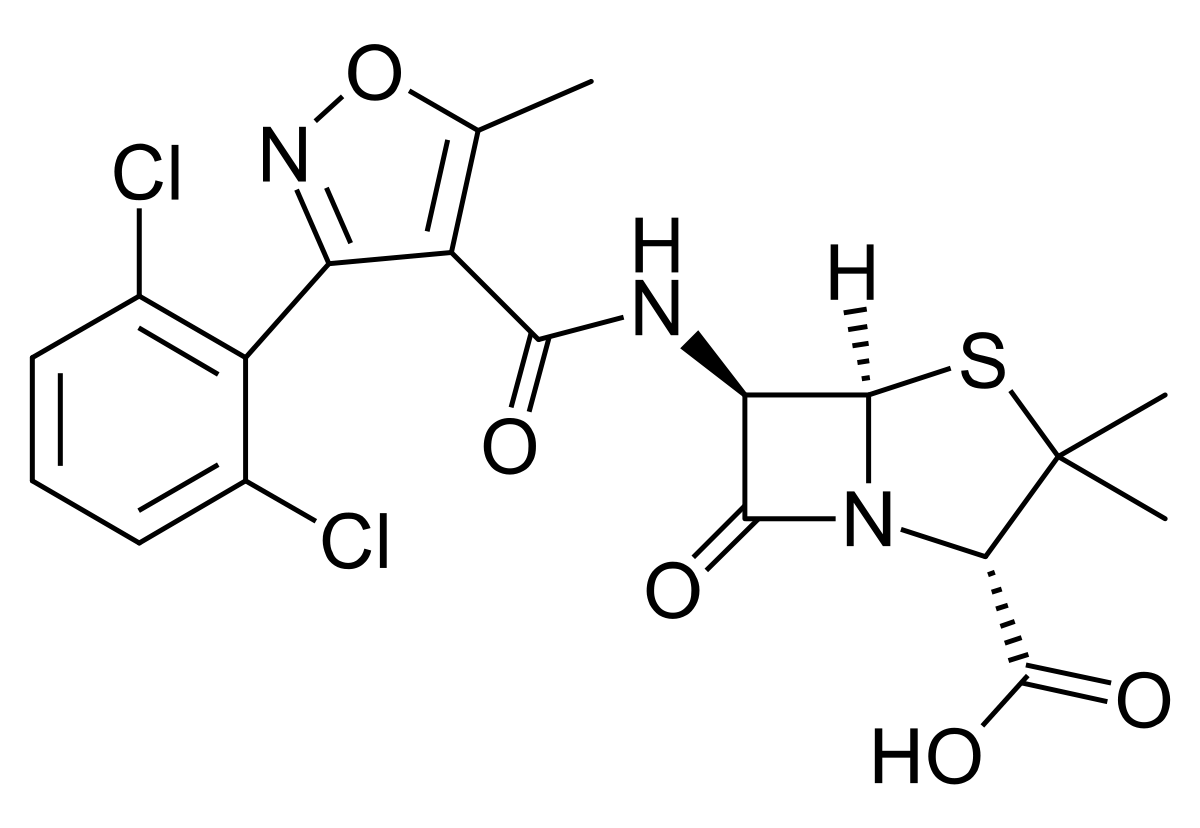
| Cloxacillin EWG-->acid stable-->orally bulky-->B lactamase resistant active against resistant strains of s.aureus lipophilic-->inactive against gram-, serum protein binding-->protection but less effective concentration (t1/2 not affected) aminoglycosides+B lactams=synergism EXCEPT PENICILLINS | |
| Flucloxacillin EWG-->acid stable-->orally bulky-->B lactamase resistant active against resistant strains of s.aureus lipophilic-->inactive against gram-, serum protein binding-->protection but less effective bactericidal concentration (t1/2 not affected) aminoglycosides+B lactams=synergism EXCEPT PENICILLINS | |
| Dicloxacillin EWG-->acid stable-->orally bulky-->B lactamase resistant active against resistant strains of s.aureus lipophilic-->inactive against gram-, serum protein binding-->protection but less effective bactericidal concentration (t1/2 not affected) aminoglycosides+B lactams=synergism EXCEPT PENICILLINS | |
| Carbenicillin (R=H) - Indanyl carbenicillin (R=indanyl; prodrug to carbenicillin, orally) carboxypenicillin not bulky-->B lactamase sensitive less active against gram+ and more active against - BECAUSE OF HYDROPHILIC COOH ALPHA TO COOH active against pseudomonas acid unstable-->injection BECAUSE OF DECARBOXYLATION REACTION (to produce benzylpenicillin=penicillin G) aminoglycosides+B lactams=synergism EXCEPT PENICILLINS | |
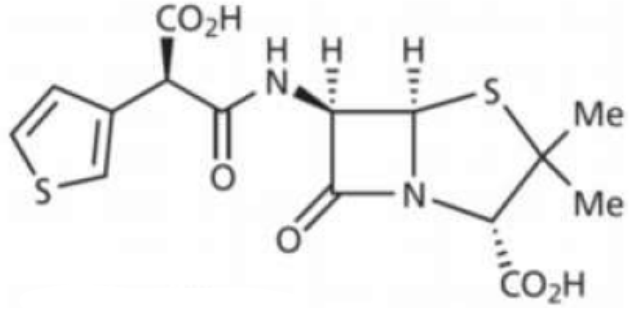
| Ticarcillin carboxypenicillin not bulky-->B lactamase sensitive less active against gram+ and more active against - BECAUSE OF HYDROPHILIC COOH ALPHA TO COOH active against pseudomonas aminoglycosides+B lactams=synergism EXCEPT PENICILLINS | |
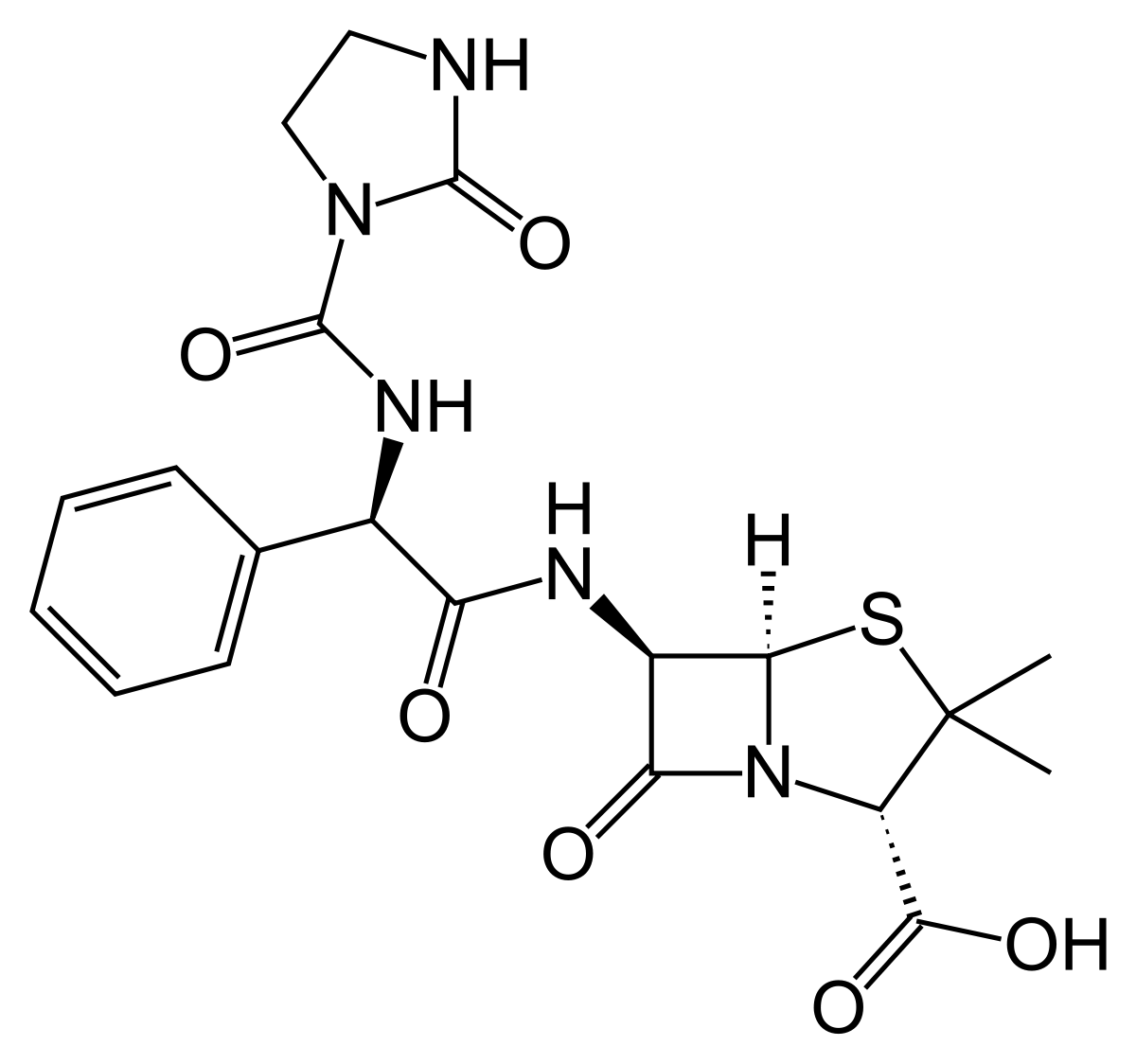
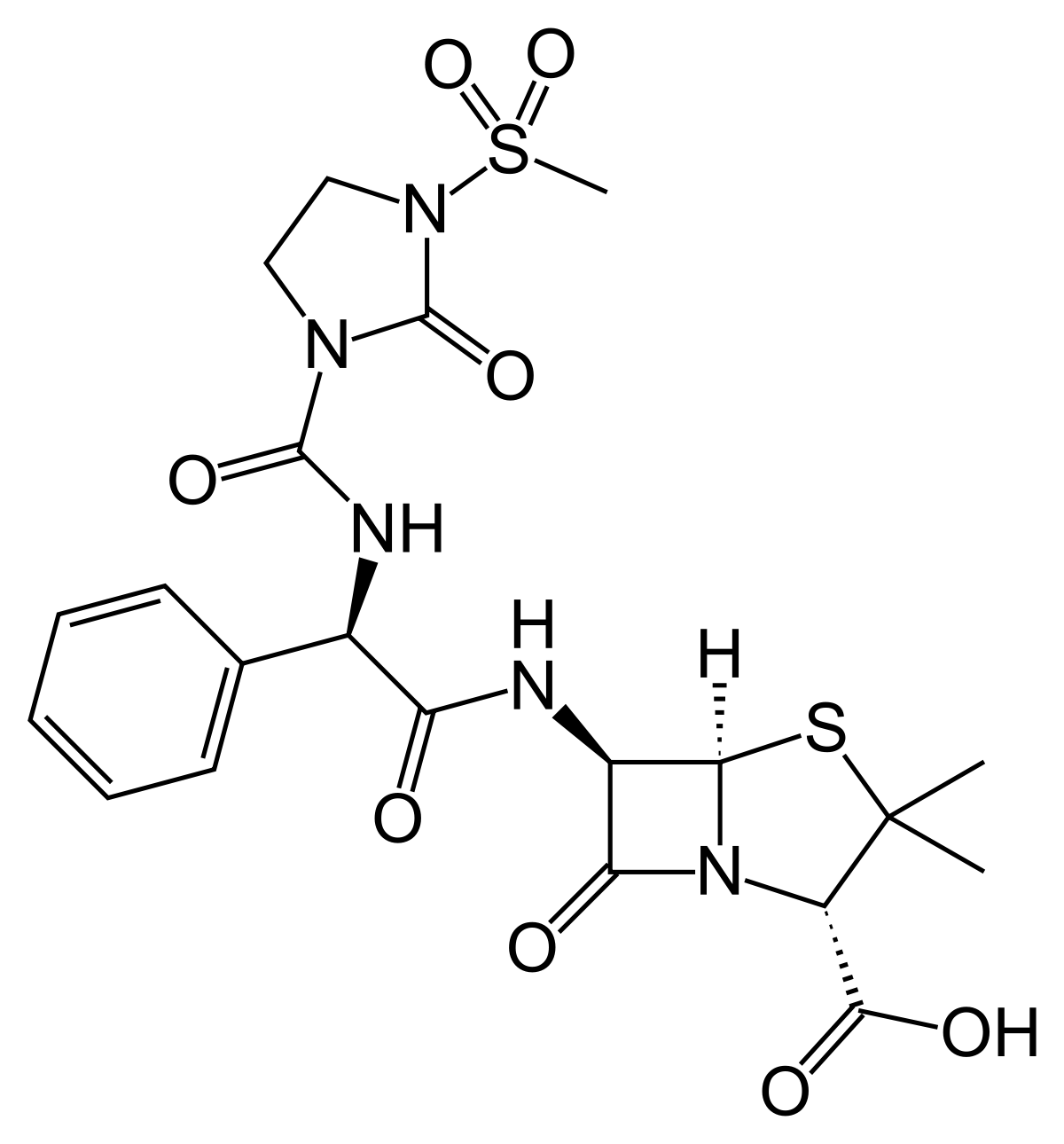
| Azlocillin Ureidopenicillin urea-->hydrophilic-->more active against gram- and pseudomonas than carbenicillin B lactamase sensitive acid stable but polar (decarboxylation)-->not absorbed orally-->IV/IM aminoglycosides+B lactams=synergism EXCEPT PENICILLINS | |
| Mezlocillin Ureidopenicillin urea-->hydrophilic-->more active against gram- and pseudomonas than carbenicillin B lactamase sensitive acid stable but polar (decarboxylation)-->not absorbed orally-->IV/IM aminoglycosides+B lactams=synergism EXCEPT PENICILLINS | |
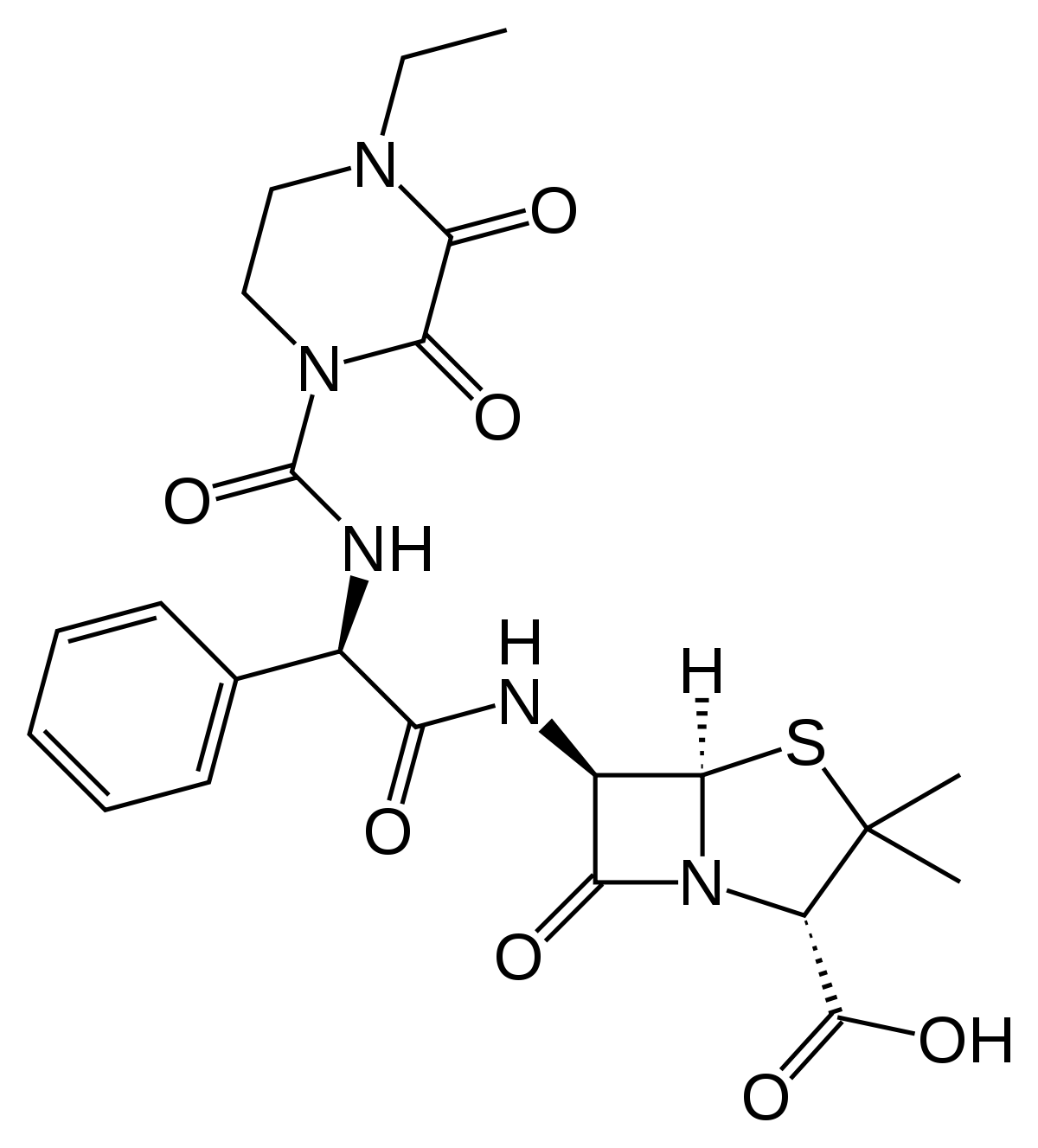
| Piperacillin Ureidopenicillin urea-->hydrophilic-->more active against gram- and pseudomonas than carbenicillin B lactamase sensitive acid stable but polar (decarboxylation)-->not absorbed orally-->IV/IM aminoglycosides+B lactams=synergism EXCEPT PENICILLINS | |
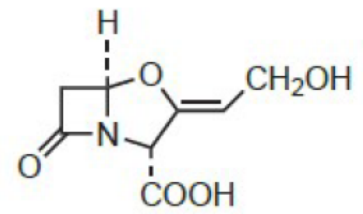
| Clavulanic acid irreversible inhibitor of most B-lactamase mold product has only weak intrinsic AB activity oxapenam core no 6-amino substitution +amoxicillin=augmentin +ticarcillin | |
| Sulbactam and Tazobactam B lactamase inhibitors weak affinity to PBP (no AB effect) ox of S to sulfone (increase potency) and no C6 substitution sulbactam+ampicillin tazobactam+piperacillin (against pseudomonas) | |
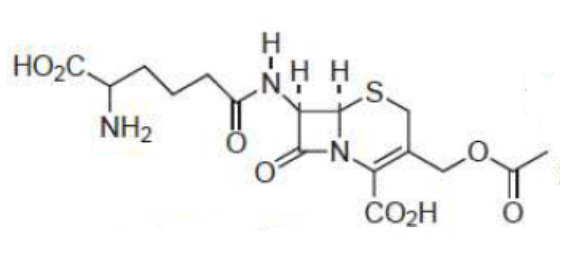
| Cephalosporin C (lead compound) same MOA as penicillin inhibits cell wall cross linking) Disadvantages: polar due to side chain-->hard to isolate and purify; 1/1000 of AB property of PenG; not absorbed orally Advantages: non toxic, less allergic, more acid stable, more stable to B lactamase, better ratio of activity against gram -&+ unstable in aq solution so formulated as salts and contain sodium bicarbonate (keep injection frozen before use) aminoglycosides+B lactams=synergism | |
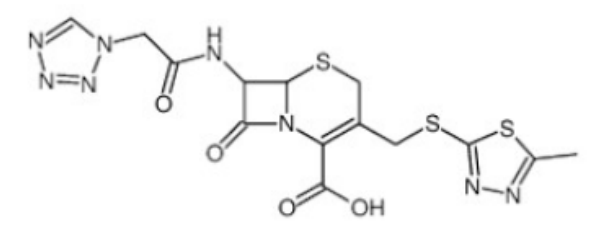
| Cefazolin first generation-->gram+ parenterally renal excretion via tubular secretion aminoglycosides+B lactams=synergism | |
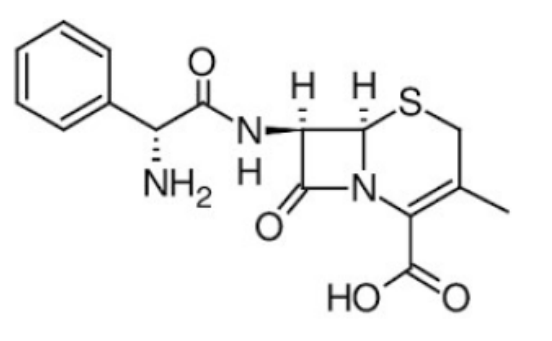
| Cefalexin first generation-->gram + orally (7-phenylglycine ampicillin like side chain and methyl at C3) less potent but less metabolized bcz methyl is bad LG have lower activity than penicillin but broader spectrum B lactamase sensitive renal excretion via tubular secretion aminoglycosides+B lactams=synergism | |
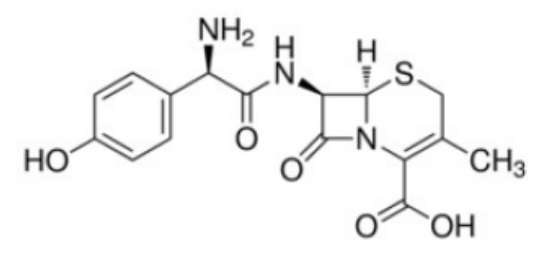
| Cefadroxil first generation-->gram + orally (7-phenylglycine amoxycillin like side chain and methyl at C3) less potent but less metabolized bcz methyl is bad LG have lower activity than penicillin but broader spectrum B lactamase sensitive renal excretion via tubular secretion aminoglycosides+B lactams=synergism | |
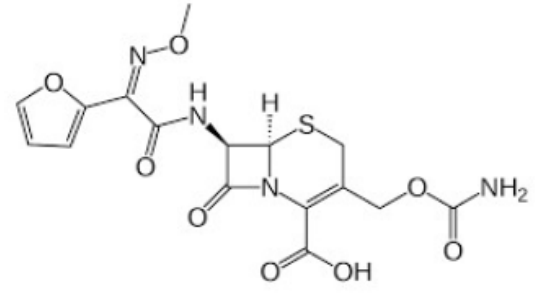
| Cefuroxime parenteral second generation (+/-) methoxyimino at C7-->steric hindrance-->B-lactamase resistant intermediate metabolic stability (carbamate) renal excretion via tubular secretion aminoglycosides+B lactams=synergism | |
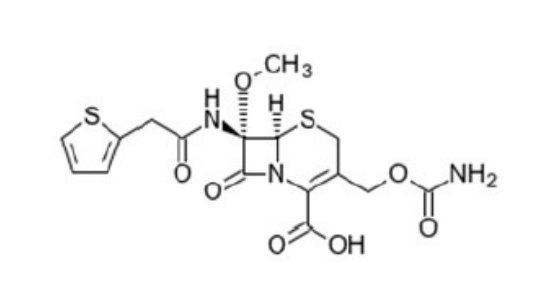
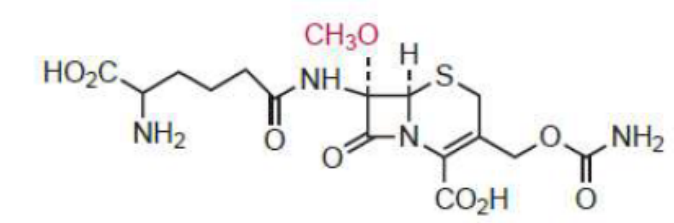
| Cefoxitin parenteral second generation (+/-) cefamycin (from Cephamycin C) 7a methoxy-->B lactamase resistant anaerobic activity intermediate metabolic stability (carbamate) renal excretion via tubular secretion aminoglycosides+B lactams=synergism | |
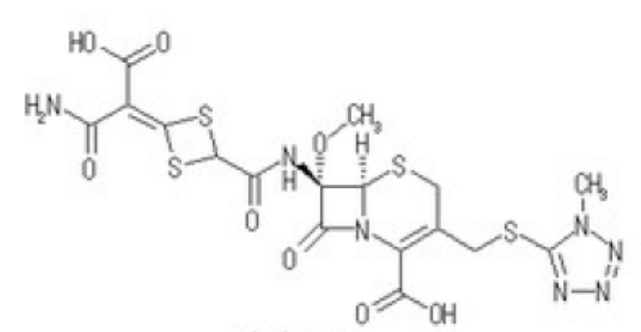
| Cefotetan parenteral second generation (+/-) cefamycin (from Cephamycin C) 7a methoxy-->B lactamase resistant anaerobic activity has MTT--> bleeding and disulfiram SE-->highest metabolic stability renal excretion via tubular secretion aminoglycosides+B lactams=synergism | |
| Cephamycin C | |
| Cefaclor like cephalexin but has Cl-->improves activity oral 2nd generation (+/-) renal excretion via tubular secretion aminoglycosides+B lactams=synergism | |
| Loracarbef oral 2nd generation (+/-) carbacephem analogue of cefaclor renal excretion via tubular secretion aminoglycosides+B lactams=synergism | |
| Cefprozil oral 2nd generation (+/-) renal excretion via tubular secretion aminoglycosides+B lactams=synergism | |
| Cefotaxime | parenteral 3rd generation (gram-) aminothiazole--> enhanced penetration of gram- and increase affinity for transpeptidase steric hindrance-->resistance to attack by B lactamase renal excretion via tubular secretion aminoglycosides+B lactams=synergism |
| Ceftizoxime | parenteral 3rd generation (gram-) aminothiazole--> enhanced penetration of gram- and increase affinity for transpeptidase steric hindrance-->resistance to attack by B lactamase renal excretion via tubular secretion aminoglycosides+B lactams=synergism |
| Ceftriaxone parenteral 3rd generation (gram-) aminothiazole--> enhanced penetration of gram- and increase affinity for transpeptidase steric hindrance-->resistance to attack by B lactamase bile excretion aminoglycosides+B lactams=synergism | |
| Ceftazidime parenteral 3rd generation (gram-) active against pseudomonas aminothiazole--> enhanced penetration of gram- and increase affinity for transpeptidase steric hindrance-->resistance to attack by B lactamase renal excretion via tubular secretion aminoglycosides+B lactams=synergism | |
| Cefixime oral 3rd generation (gram-) renal excretion via tubular secretion aminoglycosides+B lactams=synergism | |
| Ceftibuten | oral 3rd generation (gram-) renal excretion via tubular secretion aminoglycosides+B lactams=synergism |
| Cefpodoxime | oral third generation (gram-) prodrug renal excretion via tubular secretion aminoglycosides+B lactams=synergism |
| Cefdinir oral 3rd generation (gram-) renal excretion via tubular secretion aminoglycosides+B lactams=synergism | |
| Cefditoren pivoxil | oral third generation (gram-) prodrug renal excretion via tubular secretion aminoglycosides+B lactams=synergism |
| Cefepime 4th generation (zwitterion-->gram - >+) parenterally alkoxyimino-->B lactamase resistant active against pseudomonas renal excretion via tubular secretion aminoglycosides+B lactams=synergism | |
| Cefluprenam 4th generation (zwitterion-->gram - >+) parenterally alkoxyimino-->B lactamase resistant active against pseudomonas renal excretion via tubular secretion aminoglycosides+B lactams=synergism | |
| Cefpirome, Cefclidine, Cefozopran | 4th generation (zwitterion-->gram - >+) parenterally alkoxyimino-->B lactamase resistant active against pseudomonas renal excretion via tubular secretion aminoglycosides+B lactams=synergism |
| Ceftaroline fosamil 5th generation (gram + MRSA and -) IV as ester prodrug C3 substitution has strong binding to mutated PBP-->active against MRSA renal excretion via tubular secretion aminoglycosides+B lactams=synergism | |
| Ceftobiprole medocaril 5th generation (gram + MRSA and -) IV as ester prodrug C3 substitution has strong binding to mutated PBP-->active against MRSA renal excretion via tubular secretion aminoglycosides+B lactams=synergism | |
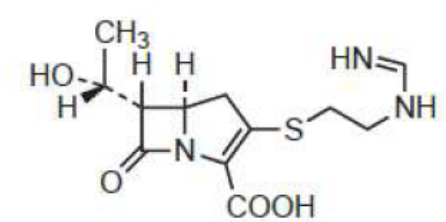
| Thienamycin Carbapenem metabolic inactivation by renal DHP-I-->short t1/2 pH dependent intermolecular aminolysis of B lactam by cysteamine side chain of other molecule-->oligomerization not absorbed by GIT-->not orally trans H: if reversed no B lactamase resistance highly active against aerobic/anaerobic gram+ and - active against pseudomonas B lactamase resistant aminoglycosides+B lactams=synergism | |
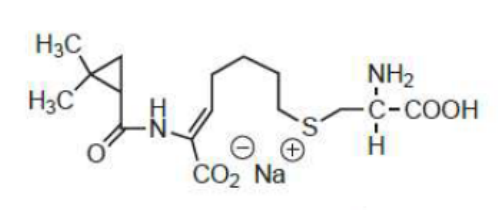
| Imipenem Carbapenem trans H: if reversed no B lactamase resistance highly active against aerobic/anaerobic gram+ and - active against pseudomonas B lactamase resistant N-formiminoyl-->no oligomerization--> more active broad spectrum bcz of hydroxyethyl metabolized by DHP-I-->toxic renal metabolite-->short t1/2=1h + Cilastatin (DHP-I inhibitor)--> less renal toxicity not orally active--> injection aminoglycosides+B lactams=synergism | |
| Cilastatin sodium | |
| Meropenem, Ertapenem, Doripenem | 2nd generation carbapenems have C4 CH3-->resistance to dehydropeptidase-->given as single agent parenterally highly active against aerobic/anaerobic gram+ and - active against pseudomonas except Ertapenem B lactamase resistant aminoglycosides+B lactams=synergism |
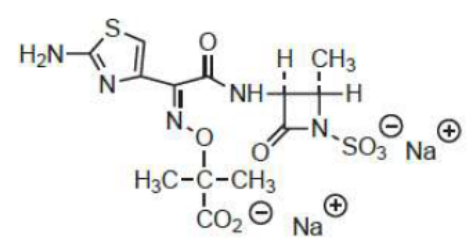
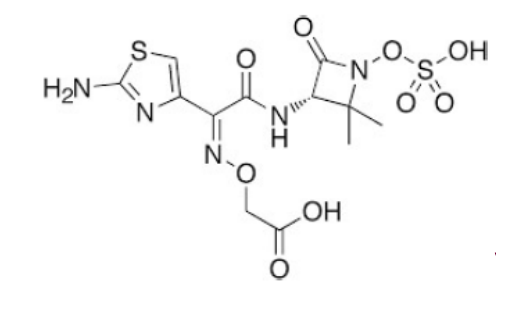
| Aztreonam disodium monobactam synthetic and chemically stable for 48h limited activity against gram+, mainly against gram - (including pseudomonas) strong e-withdrawing sulfamic acid makes it less stable B-lactamase resistant due to C2 a-methyl fused ring not needed for activity given by injection bcz not orally active mainly unchanged excretion in urine aminoglycosides+B lactams=synergism | |
| Tigemonam synthetic agent highly resistant to B-lactamase similar spectrum to aztreonam (gram- and pseudomonas) orally active with excellent bioavailability aminoglycosides+B lactams=synergism | |
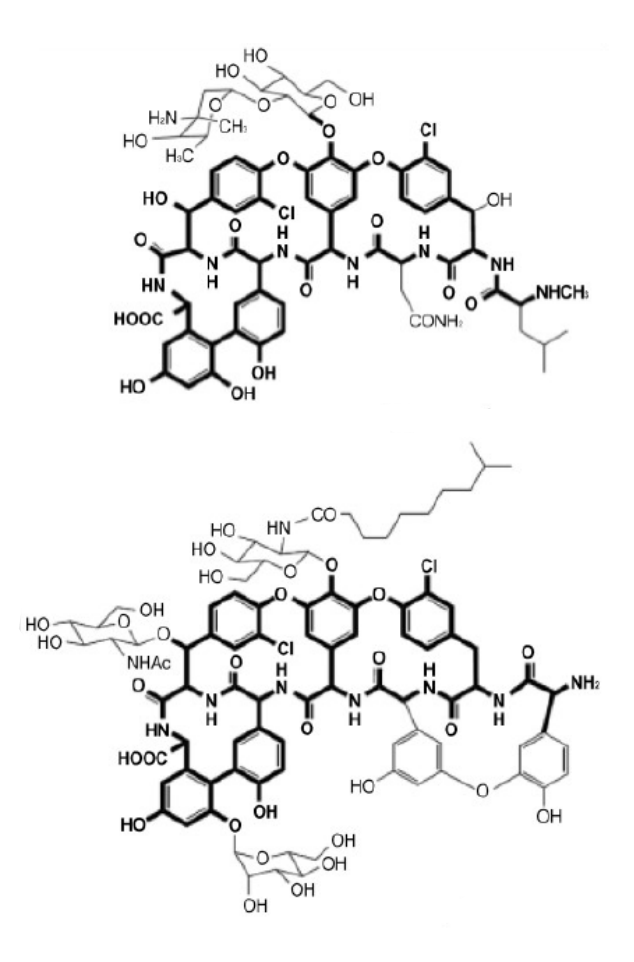
| Vancomycin and teicoplanin natural glycoproteins, cyclic peptides given parentarally active against MRSA SE: hypersensitivity, nephro and ototoxicity (only vancomycin) different MOA than B-lactams: bind to D-ala-D-ala end of peptide-->block cross linking inhibit cell wall synthesis through inhibition of transglycosylation step-->inhibition of elongation of peptidoglycan matrix (become susceptible to osmotic pressure) | |
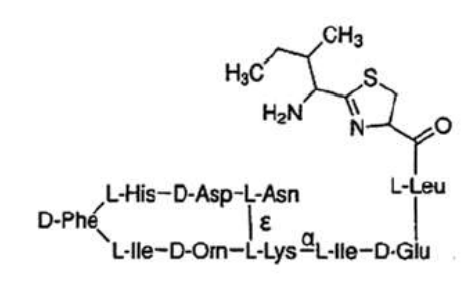
| Bacitracin natural cyclic peptide inhibits dephosphorylation of carrier molecules responsible for transporting PG monomers across plasma membranes SE: hypersensitivity, nephro+neurotoxicity limited use to topical and IM with caution | |
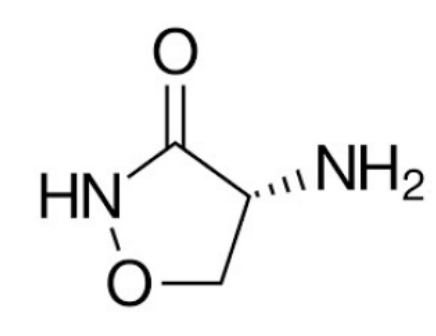
| Cycloserine natural structural analogue of D-ala competitive inhibitor of D-ala-D-ala synthetase and D-ala racemase orally active SE: CNS: tremor, seizure, confusion, hallucination and psychosis | |
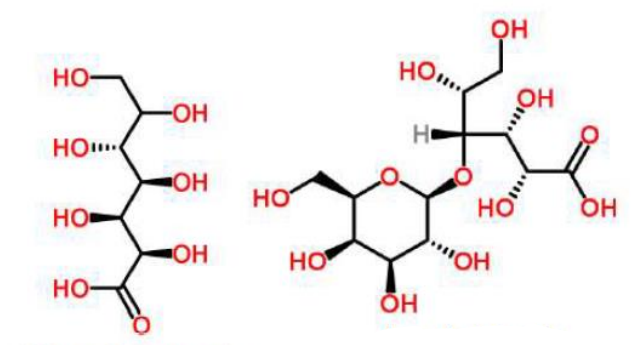
| Glucoheptonic (left) and Lactobionic (right) water soluble | |
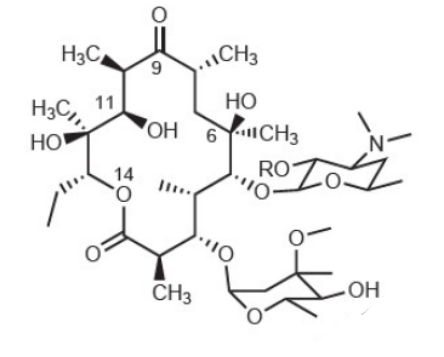
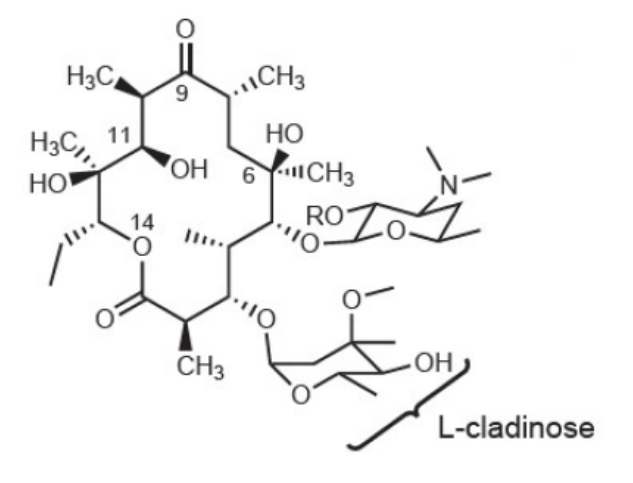
| Erythromycin natural macrolide-->bacteriostatic, reversible binding to 50S, gram+ ester or salt formation (prodrug) to increase water/lipid solubility to give parenterally: lactobionate (IV), ethylsuccinate (oral suspension for paediatrics to mask bitter taste) lipophilic (can add surfactant for slow release or glucoheptonic/lactobionic to make it water soluble) macrolides, clindamycin, lincomycin, chloramphenicol bind in same vicinity-->cross resistance form inactive ketal in acid-->given orally as coated tablet short t1/2 SE: GI dist, QT prolongation, cholestatic jaundice (erythromycin estolate), hypersensitivity (rare) not given IM bcz severe pain DDI bcz inhibit CYP3A4 main liver metabolite: N-demethylated analog safe during breastfeeding but not preg 3 MOA of resistance: lower binding to b ribosome, active efflux from cell, lack of penetration in some gram- | |
| Erythromycin prodrugs: - Erythromycin lactobionate (IV) - if R=CO(CH2)CO2C2H5=erythromycin ethylsuccinate: oral suspension for paediatric use to mask bitter taste | |
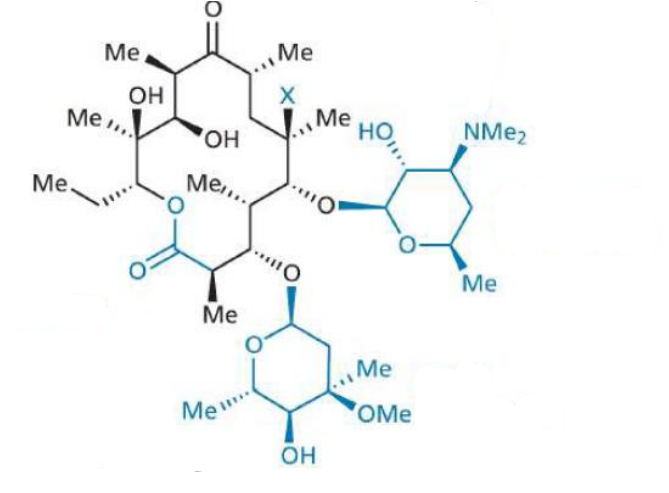
| Clarithromycin semi synthetic macrolide gram+,-, atypical bacteria improved acid stability and oral absorption by replacing OH by OMe less gastric upset than erythromycin 1st pass-->C-14 hydroxy analog-->greater antimicrobial potency enhanced lipophilicity-->lower and less frequent dosage for mild infections inhibitor of CYP3A4 SE: QT prolongation 3 MOA of resistance: lower binding to b ribosome, active efflux from cell, lack of penetration in some gram- | |
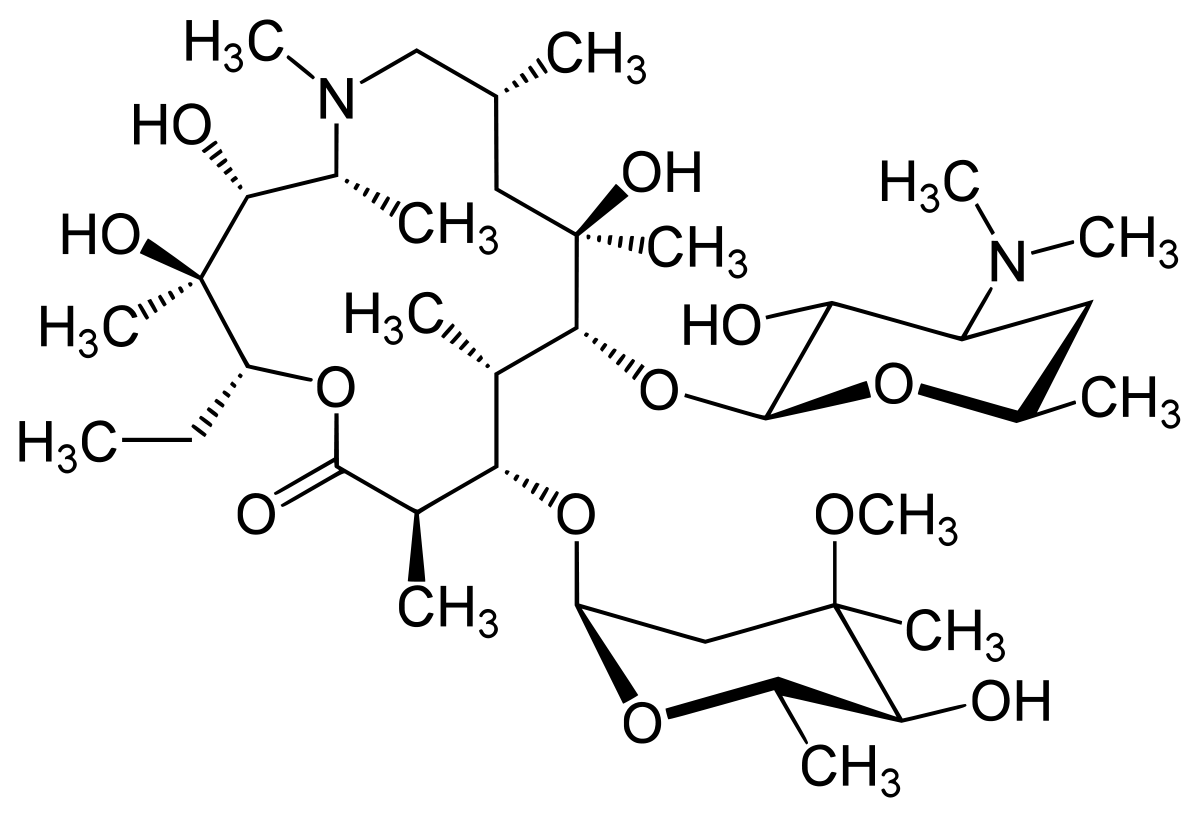
| Azithromycin semi synthetic macrolide gram+,-, atypical bacteria 15memb ring by adding N-CH3 on erythromycin -->improved acid stability longer t1/2 bcz of greater and longer tissue penetration (1x daily on empty stomach) broader spectrum than erythr ad clarithr significant postAB effect inactive hepatic metabolites 3 MOA of resistance: lower binding to b ribosome, active efflux from cell, lack of penetration in some gram- SE: QT prolongation | |
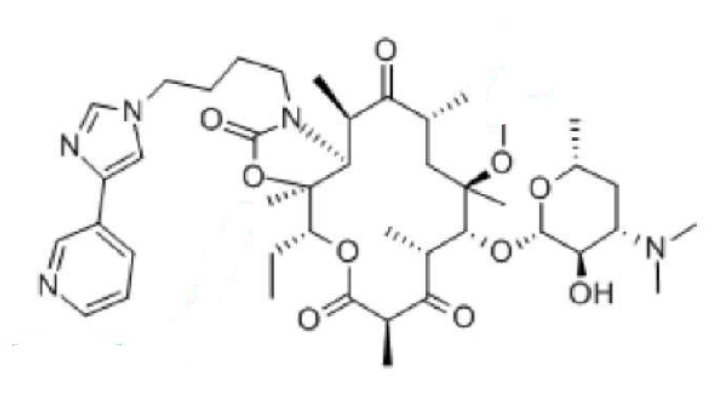
| Telithromycin ketolide (erythromycin derivative) active against erythromycin resistant improved acid stability oral to treat most community-acquired pneumonia CI with myasthenia gravis (pyridine ring)-->respiratory failure CYP3A4 competitive inhibitor inactive hepatic metabolites | |
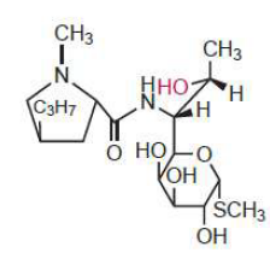
| Lincomycin Lincosamide natural erythromycin derivative 8C sugar (thiomethyl amino-octoside) weakly basic, form acid salts binding at a side partly overlapping with the macrolide site and are mutually cross-resistant with macrolides -->same MOA hepatic metabo: N-demethylated metabolite retains biologic activity gives Clindamycin reserved for penicillin-allergic patients bcz of increased risk of pseudomembraneous colitis (by Clostridium difficile) | |
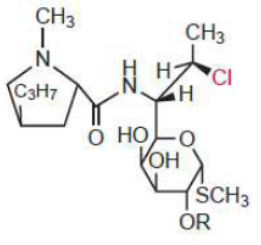
| Clindamycin from Lincomycin Cl at C7-->more bioactive and lipophilic than lincomycin-->better absorbed orally similar spectrum to macrolides N-demethylated metabolite is active (others are inactive) SE: GI, BBW for pseudomembranous colitis, SJS | |
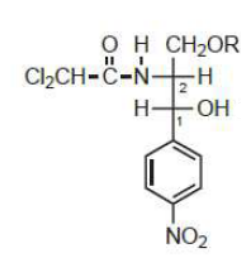
| Chloramphenicol only 1of 4 diastereomers is significantly active bacteriostatic active against gram+ and - binds to 50S near where macrolides and lincosamides bind resistance: enzymes that catalyze acetylation of hydroxyls-->inactive rapidly and completely absorbed orally inactive metabolites: +++C3 and C1 glucuronides diffuses in CSF-->treat meningitis ester prodrugs: C3-palmitate for pediatric oral suspension to mask bitter taste C3-hemisuccinoyl ester--> increase water solubility-->IV SE: inhibition of haematopoiesis, +++in older patients or in those with renal insufficiency "GRAY BABY" syndrome: when given to young infants when liver glucuronidation is underdeveloped-->rapid accumulation of the drug due to impaired excretion | |
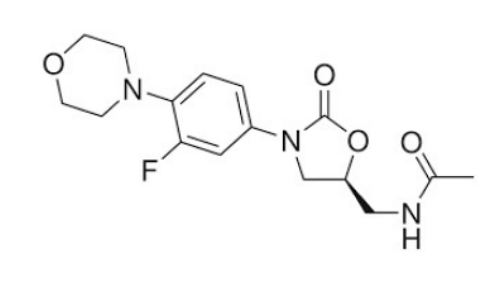
| Linezolid oxazolidinone treatment of infections caused by gram+ resistant to other ABs (including MRSA,VRE) not significant clinically against gram- Bacteriostatic effect in vitro but bactericidal in vivo bcz inhibits production of toxins by staph and strep orally active metabolites by liver | |
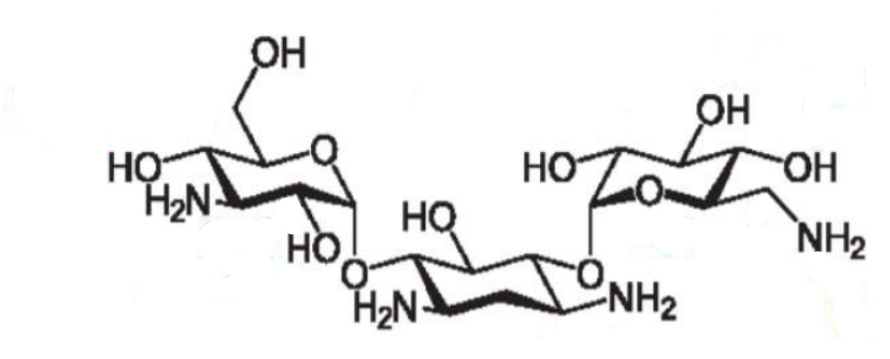
| Kanamycin A aminoglycoside (carb+amine) work best at alkaline pH-->positively charged-->active against aerobic gram- has deoxystreptamine binds irreversibly to 30S-->inhibit initiation of protein synthesis and inhibit fidelity translocation of genetic message-->nonsense protein bacteriostatic at low dose and bactericidal at high dose at high concentrations, eukaryotic protein synthesis can also be inhibited low PPB, poor oral absorption-->topical/IM/IV, cross placenta-->teratogenic, ACCUMULATE IN KIDNEY AND INNER EAR-->reduce dose if impaired kidney function, excreted in active form in urine nephro and oto toxicity: hearing loss and vertigo curare-like NM blockade (may be due to competitive inhibition of Ca ion-dependent ACh release at NM junction resistance: 1. bacterial amplification of enzymes that inactivate the AB (N-acetylate, O-phosphorylate, O-adenylate)-->prevent ribosomal binding, 2.point mutation of ribosomal A site-->decrease target affinity, 3.decrease uptake into bacterial cells aminoglycosides+B lactams=synergism EXCEPT PENICILLINS | |
| Neomycin, Paromomycin, Tobramycin | aminoglycosides (carb+amine) work best at alkaline pH-->positively charged-->active against aerobic gram- Neomycin, Tobramycin have deoxystreptamine Neomycin-->absorbed in ulcerated and denuded areas of GI, +++ototoxicity binds irreversibly to 30S-->inhibit initiation of protein synthesis and inhibit fidelity translocation of genetic message-->nonsense protein bacteriostatic at low dose and bactericidal at high dose at high [] , eukaryotic protein synthesis can also be inhibited low PPB, poor oral absorption-->topical/IM/IV, cross placenta-->teratogenic, ACCUMULATE IN KIDNEY AND INNER EAR-->reduce dose if impaired kidney function, excreted in active form in urine nephro and oto toxicity: hearing loss and vertigo curare-like NM blockade (may be due to competitive inhibition of Ca ion-dependent ACh release at NM junction tobramycin overcomes resistance by removal of OH in ring 1-->no phosphorylation aminoglycosides+B lactams=synergism EXCEPT PENICILLINS |
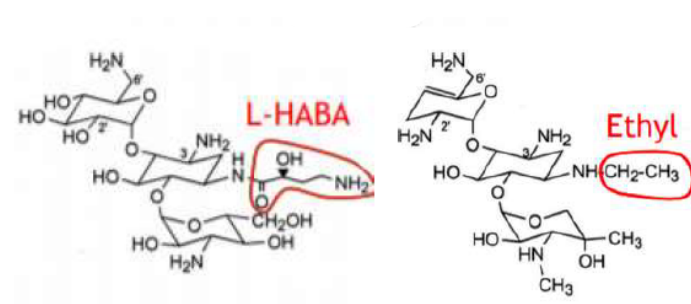
| Amikacin and Netilmicin aminoglycoside (carb+amine) work best at alkaline pH-->positively charged-->active against aerobic gram- binds irreversibly to 30S-->inhibit initiation of protein synthesis and inhibit fidelity translocation of genetic message-->nonsense protein bacteriostatic at low dose and bactericidal at high dose at high concentrations, eukaryotic protein synthesis can also be inhibited low PPB, poor oral absorption-->topical/IM/IV, cross placenta-->teratogenic, ACCUMULATE IN KIDNEY AND INNER EAR-->reduce dose if impaired kidney function, excreted in active form in urine nephro and oto toxicity: hearing loss and vertigo curare-like NM blockade (may be due to competitive inhibition of Ca ion-dependent ACh release at NM junction to overcome resistance: L-HABA on Amikacin and N-ethyl on Netilmicin aminoglycosides+B lactams=synergism EXCEPT PENICILLINS | |
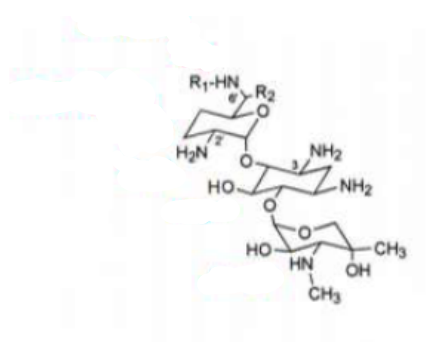
| Gentamicin has deoxystreptamine work best at alkaline pH-->positively charged-->active against aerobic gram- has deoxystreptamine binds irreversibly to 30S-->inhibit initiation of protein synthesis and inhibit fidelity translocation of genetic message-->nonsense protein bacteriostatic at low dose and bactericidal at high dose at high concentrations, eukaryotic protein synthesis can also be inhibited low PPB, poor oral absorption-->topical/IM/IV, cross placenta-->teratogenic, ACCUMULATE IN KIDNEY AND INNER EAR-->reduce dose if impaired kidney function, excreted in active form in urine nephro and oto toxicity: hearing loss and vertigo curare-like NM blockade (may be due to competitive inhibition of Ca ion-dependent ACh release at NM junction to overcome resistance: secondary amine in ring 1, removal of 3'OH and or 4'OH in ring 1 aminoglycosides+B lactams=synergism EXCEPT PENICILLINS | |
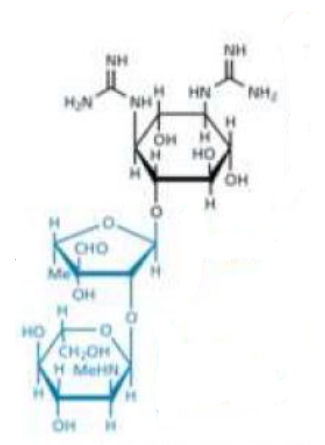
| Streptomycin aminoglycoside (carb+amine) work best at alkaline pH-->positively charged-->active against aerobic gram- exception bcz has streptidine (from streptamine) linked to 2 amino sugars (pentose and hexose) binds irreversibly to 30S-->inhibit initiation of protein synthesis and inhibit fidelity translocation of genetic message-->nonsense protein bacteriostatic at low dose and bactericidal at high dose at high concentrations, eukaryotic protein synthesis can also be inhibited low PPB, poor oral absorption-->topical/IM/IV, cross placenta-->teratogenic, ACCUMULATE IN KIDNEY AND INNER EAR-->reduce dose if impaired kidney function, excreted in active form in urine nephro and oto toxicity: hearing loss and vertigo curare-like NM blockade (may be due to competitive inhibition of Ca ion-dependent ACh release at NM junction resistance: 1. bacterial amplification of enzymes that inactivate the AB -->prevent ribosomal binding, 2.point mutation of ribosomal A site-->decrease target affinity, 3.decrease uptake into bacterial cells aminoglycosides+B lactams=synergism EXCEPT PENICILLINS | |
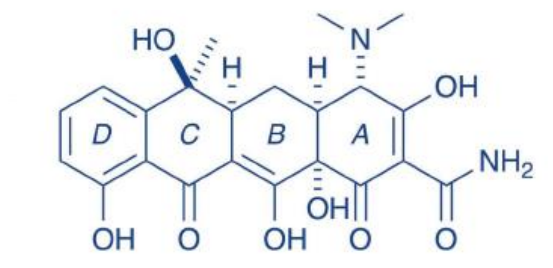
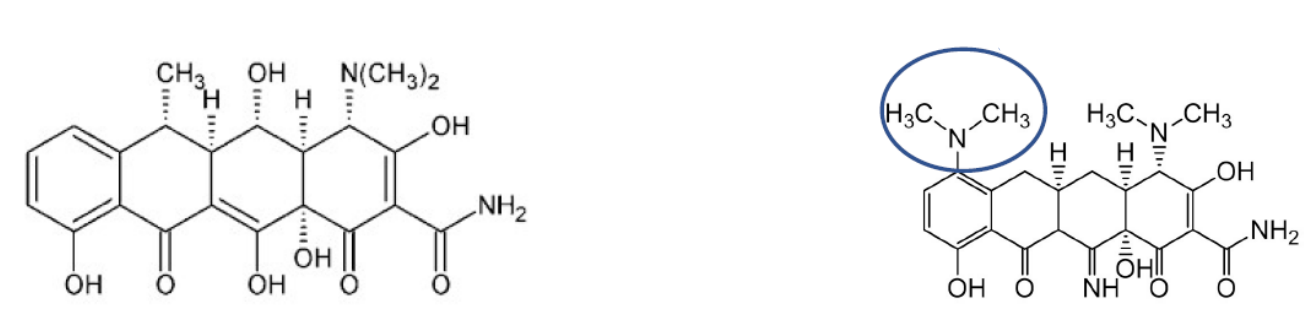
| Tetracycline natural tetracycline (1st gen) intermediate acting (t1/2=10-15h) bacteriostatic, active against gram+, - aerobic and anaerobic orally (food and milk decrease absorption) MOA: inhibit protein synthesis by binding to 30S and inhibiting binding of aminoacyltransfer-RNA to the ribosome-->termination of peptide chain growth derivative of octahydronaphthacene amphoteric: pka=3,7,9.5 reversible epimerization at C4 in acidic conditions: equal amounts of 2 diastereomers at equilibrium (only a is active (N to the back) not 4-epitetracycline) can also undergo dehydration in acidic conditions-->anhydrotetracycline (inactive) 4-epitetracycline can also undergo dehydration and give 4-epianhydrotetracycline (inactive and TOXIC-->Fanconi-like syndrome) in base: cleavage of ring by formation of lactonic product isotetracycline (inactive) acidic function chelates with metal ions-->insoluble at neutral pH-->incompatible with antacids and consumption of products rich in Ca ion should be avoided in children and pregnant women resistance by ribosomal protection | |
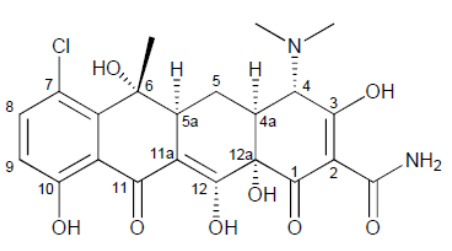
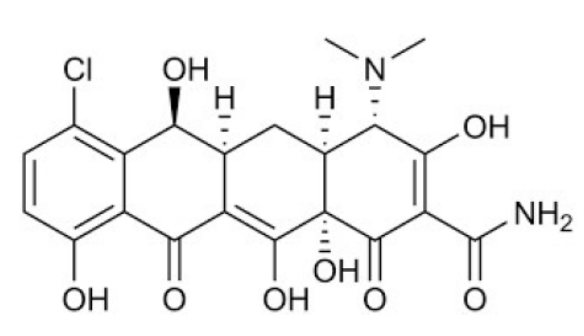
| Chlortetracycline natural tetracycline (1st gen) short acting (t1/2=7h) bacteriostatic, active against gram+, - aerobic and anaerobic orally (food and milk decrease absorption) MOA: inhibit protein synthesis by binding to 30S and inhibiting binding of aminoacyltransfer-RNA to the ribosome-->termination of peptide chain growth derivative of octahydronaphthacene amphoteric: pka=3,7,9.5 reversible epimerization at C4 in acidic conditions: equal amounts of 2 diastereomers at equilibrium (only a is active (N to the back) not 4-epitetracycline) can also undergo dehydration in acidic conditions-->anhydrotetracycline (inactive) 4-epitetracycline can also undergo dehydration and give 4-epianhydrotetracycline (inactive and TOXIC-->Fanconi-like syndrome) in base: cleavage of ring by formation of lactonic product isotetracycline (inactive) acidic function chelates with metal ions-->insoluble at neutral pH-->incompatible with antacids and concomitant consumption of daily products rich in Ca ion Cl-->phototoxicity should be avoided in children and pregnant women resistance by ribosomal protection | |
| Demeclocycline natural tetracycline (1st gen), intermediate acting (t1/2=10-15h), lacks C6 methyl of tetracycline-->2°alcohol-->more chemically stable than tetracycline against dehydration orally (food and milk decrease absorption) C7-Cl: phototoxicity: erythema in sensitive patients on exposure to strong sunlight bacteriostatic, active against gram+, - aerobic and anaerobic MOA: inhibit protein synthesis by binding to 30S... derivative of octahydronaphthacene amphoteric: pka=3,7,9.5, reversible epimerization..., can also undergo dehydration in acidic conditions-->anhydrotetracycline (inactive) 4-epitetracycline can also undergo dehydration and give 4-epianhydrotetracycline (inactive and TOXIC-->Fanconi-like syndrome) in base: cleavage of ring by formation of lactonic product isotetracycline (inactive) acidic function chelates with metal ions-->insoluble at neutral pH-->incompatible with antacids and products rich in Ca ion avoided in children/preg resistance by ribosomal protection | |
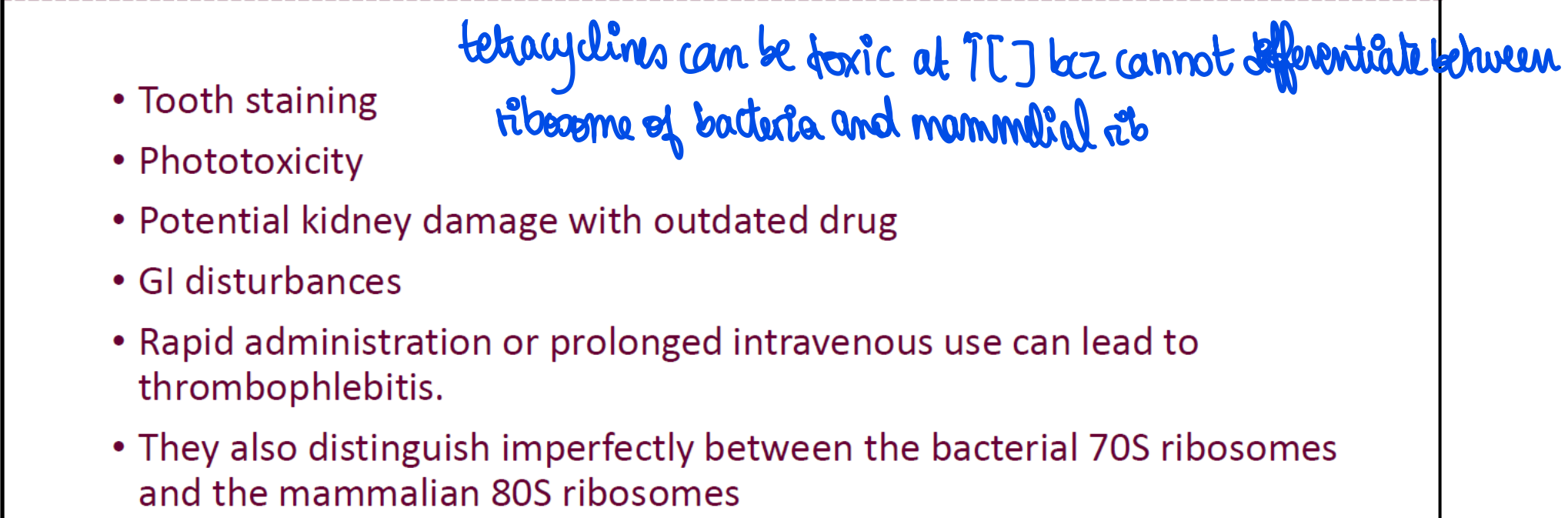
| Doxycycline and Minocycline Deoxytetracyclines semi synthetic (2nd gen) long acting (t1/2>=16h) orally (food and milk decrease absorption) reversible epimerization at C4 in acidic conditions no C6 hydroxyl grp-->cannot undergo dehydration under acidic conditions-->completely free of kidney toxicity,Stable in basic conditions bacteriostatic, active against gram+, - aerobic and anaerobic MOA: inhibit protein synthesis by binding to 30S... derivative of octahydronaphthacene amphoteric: pka=3,7,9.5 acidic function chelates with metal ions-->insoluble at neutral pH-->incompatible with antacids and products rich in Ca2+ avoid in child/preg resistance by ribosomal protection | |
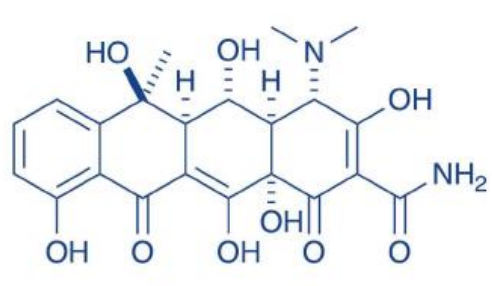
| Tigecycline Glycylcycline: additional glyclamido substitution at 9 position 3rd gen (next gen) long acting (t1/2>=16h) more active than old tetracyclines against resistant strains IV bacteriostatic, active against gram+, - aerobic and anaerobic MOA: inhibit protein synthesis by binding to 30S and inhibiting binding of aminoacyltransfer-RNA to the ribosome-->termination of peptide chain growth derivative of octahydronaphthacene amphoteric: pka=3,7,9.5 reversible epimerization at C4 in acidic conditions no C6 hydroxyl grp-->cannot undergo dehydration under acidic conditions-->completely free of kidney toxicity,Stable in basic conditions acidic function chelates with metal ions... with antacids and products rich in Ca2+ avoid in child/preg resistance by ribosomal protection | |
| Oxytetracycline natural tetracycline (1st gen) bacteriostatic, active against gram+, - aerobic and anaerobic MOA: inhibit protein synthesis by binding to 30S... orally (food and milk decrease absorption) derivative of octahydronaphthacene amphoteric: pka=3,7,9.5 reversible epimerization at C4 in acidic conditions: equal amounts of 2 diastereomers... can also undergo dehydration in acidic conditions-->anhydrotetracycline (inactive) 4-epitetracycline can also undergo dehydration and give 4-epianhydrotetracycline (inactive and TOXIC-->Fanconi-like syndrome) in base: cleavage of ring by formation of lactonic product isotetracycline (inactive) acidic function chelates with metal ions... avoid in child/preg resistance by ribosomal protection | |
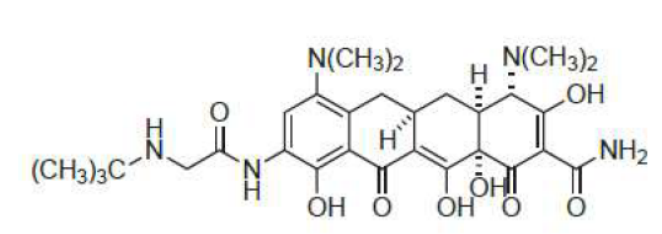
| SE of tetracyclines |
Image:
Se (binary/octet-stream)
|
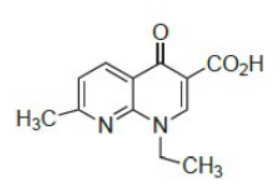
| Nalidixic acid precursor of synthetic quinolones 1st gen (against few gram- to treat UTI and lack activity against gram+, pseudomonas, and anaerobes) 1,8-naphthyridine derivative able to chelate polyvalent metal ions-->decreased solubility and reduced drug absorption agents containing polyvalent metals should be administered separately from quinolones orally with excellent bioav renal excretion moderate PPB-->long t1/2 resistance: 1. mutation in gyrase/topoisomerase: cross resistance. 2. increase in drug efflux/decrease in outer membrane permeability affecting drug influx (more common in gram-) | |
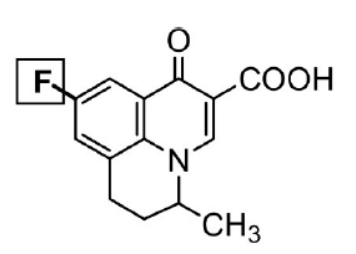
| Flumequine fluoroquinolone from nalidixic acid 1st gen (against gram- to treat UTI and lack activity against gram+, pseudomonas, and anaerobes) bactericidal MOA: inhibition of DNA synthesis by inhibiting DNA gyrase (+++in gram -) so cell's DNA becomes inaccessible-->cell death human topoisomerase 2 has low affinity at normal doses able to chelate polyvalent metal ions-->decreased solubility and reduced drug absorption agents containing polyvalent metals should be administered separately from quinolones orally with excellent bioav renal excretion moderate PPB-->long t1/2 resistance: 1. mutation in gyrase/topoisomerase: cross resistance. 2. increase in drug efflux/decrease in outer membrane permeability affecting drug influx (more common in gram-) | |
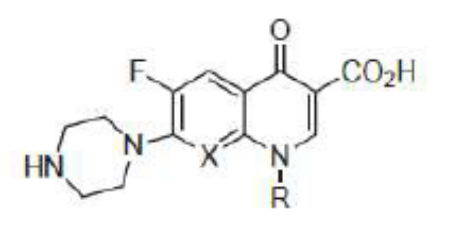
| Norfloxacin and Ciprofloxacin ciprofloxacin-->against pseudomonas quinolone from nalidixic acid 2nd gen (active against gram - and weak activity against some gram + like streptococcus-->for systemic infections) CNS SE ciprofloxacin also given IV able to chelate polyvalent metal ions-->decreased solubility and reduced drug absorption agents containing polyvalent metals should be administered separately from quinolones orally with excellent bioav renal excretion moderate PPB-->long t1/2 resistance: 1. mutation in gyrase/topoisomerase: cross resistance. 2. increase in drug efflux/decrease in outer membrane permeability affecting drug influx (more common in gram-) Norfloxacin SE: crystalluria | |
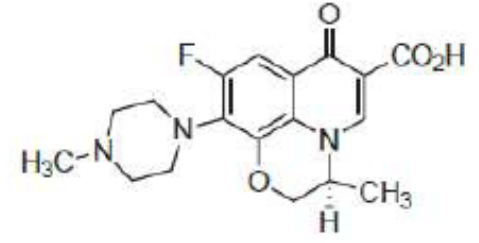
| Ofloxacin (2nd gen: active against gram - including pseudomonas and weak activity against some gram + like streptococcus-->for systemic infections) and Levofloxacin (3rd gen: once daily, active against gram + and strep pneumonia and atypical bacteria, less active against pseudomonas) quinolone from nalidixic acid levo is 2x as active and more potent bcz of increased binding to DNA gyrase also available IV newer drugs have better distribution-->used for systemic infections able to chelate polyvalent metal ions-->decreased solubility and reduced drug absorption agents containing polyvalent metals should be administered separately from quinolones orally with excellent bioav renal excretion moderate PPB-->long t1/2 resistance: 1. mutation in gyrase/topoisomerase: cross resistance. 2. increase in drug efflux/decrease in outer membrane permeability affecting drug influx (more common in gram-) | |
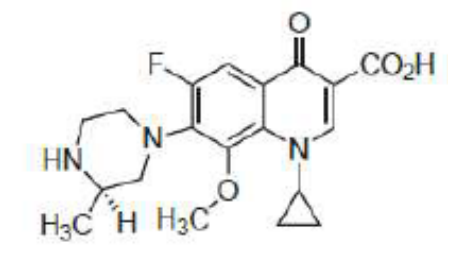
| Gatilfloxacin 3rd gen (3rd gen: once daily, active against gram + and strep pneumonia and atypical bacteria, less active against pseudomonas) quinolone from nalidixic acid low phototoxicity newer drugs have better distribution-->used for systemic infections able to chelate polyvalent metal ions-->decreased solubility and reduced drug absorption agents containing polyvalent metals should be administered separately from quinolones orally with excellent bioav renal excretion moderate PPB-->long t1/2 resistance: 1. mutation in gyrase/topoisomerase: cross resistance. 2. increase in drug efflux/decrease in outer membrane permeability affecting drug influx (more common in gram-) | |
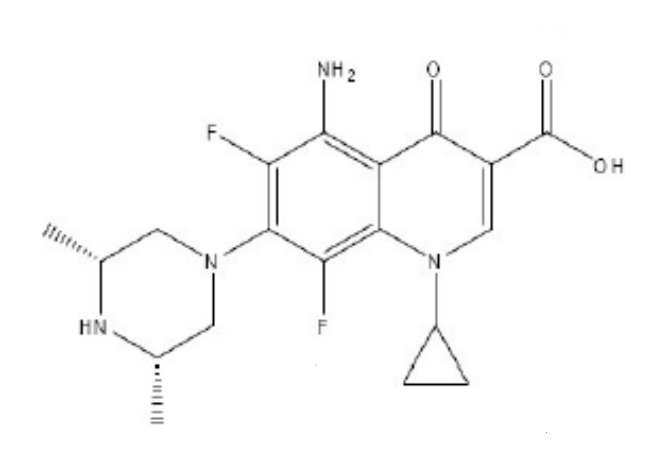
| Sparfloxacin 3rd gen (3rd gen: once daily, active against gram + and strep pneumonia and atypical bacteria, less active against pseudomonas) quinolone from nalidixic acid increased activity against gram+ QT prolongation newer drugs have better distribution-->used for systemic infections able to chelate polyvalent metal ions-->decreased solubility and reduced drug absorption agents containing polyvalent metals should be administered separately from quinolones orally with excellent bioav renal excretion moderate PPB-->long t1/2 phototoxicity resistance: 1. mutation in gyrase/topoisomerase: cross resistance. 2. increase in drug efflux/decrease in outer membrane permeability affecting drug influx (more common in gram-) | |
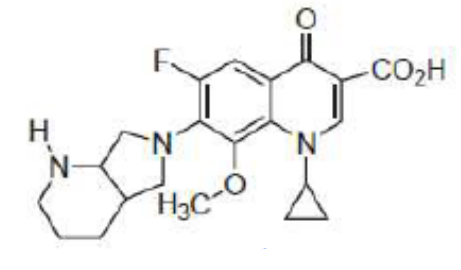
| Moxifloxacin 4th gen (active against anaerobes and aerobic gram+ but not much against gram -) quinolinone from nalidixic acid low phototoxicity NO RENAL EXCRETION newer drugs have better distribution-->used for systemic infections able to chelate polyvalent metal ions-->decreased solubility and reduced drug absorption agents containing polyvalent metals should be administered separately from quinolones orally with excellent bioav moderate PPB-->long t1/2 resistance: 1. mutation in gyrase/topoisomerase: cross resistance. 2. increase in drug efflux/decrease in outer membrane permeability affecting drug influx (more common in gram-) | |
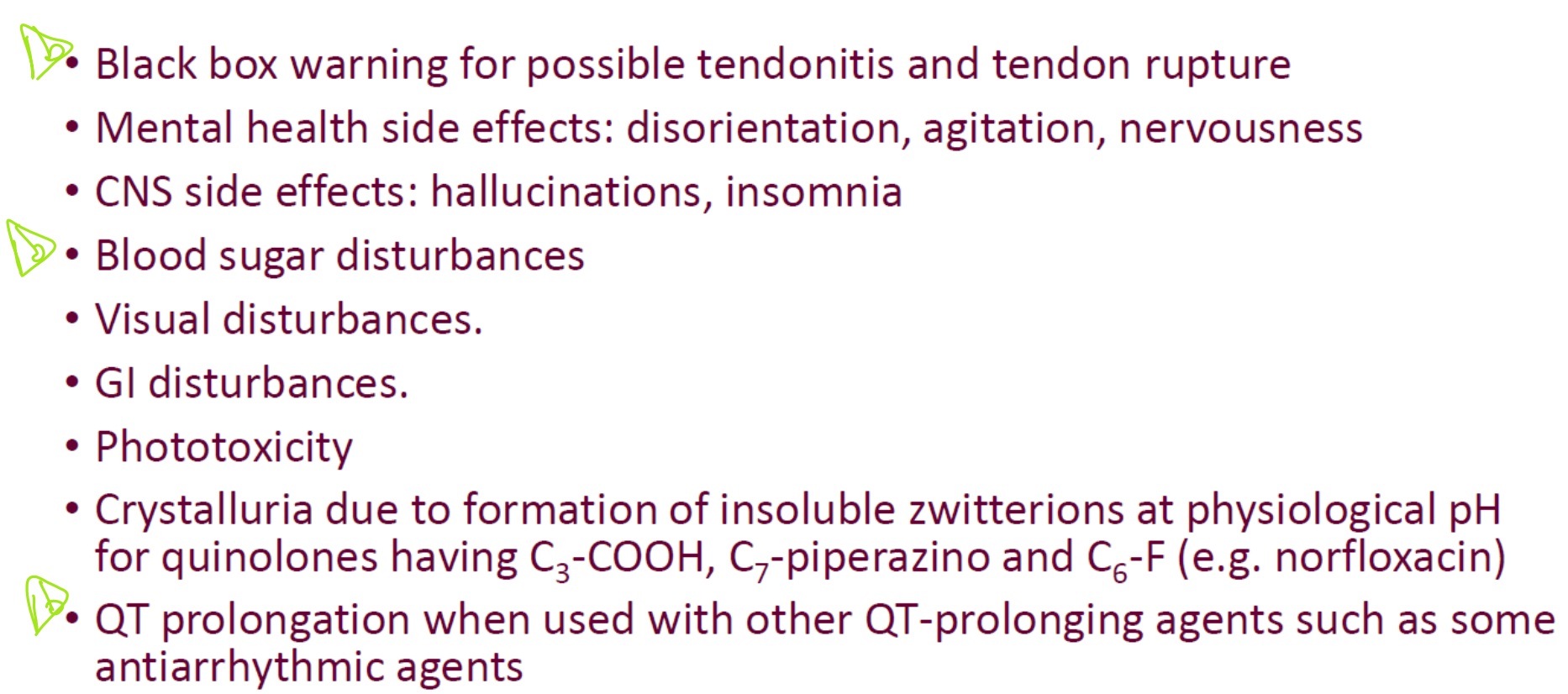
| SE of quinolones |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Möchten Sie mit GoConqr kostenlos Ihre eigenen Karteikarten erstellen? Mehr erfahren.