6598230
Beschreibung
Karteikarten von Andrew Street, aktualisiert more than 1 year ago
|
|
Erstellt von Andrew Street
vor etwa 8 Jahre
|
|
| Frage | Antworten |
| 982 S & Sx of acute MI. | * Acute central CP lasting >20/60. P is non-responsive to GTN. May radiate to L arm, neck, or jaw. Often associated Sx: * Nausea * Sweatiness * Dyspnoea * Palpitations May present without CP eg in elderly or DM. Presentations may include: * Syncope * Pulmonary oedema * Epigastric P & vomiting * Post-op hypotension or oliguria * Acute confusion * Diabetic hyperglycaemic states. OHCM p112. |
| 983 The common mechanism to all ACS (STEMI, NSTEMI, unstable angina) is r..... or erosion of the fibrous c..... of a coronary artery p..... This leads to platelet aggregation and adhesion, localized t....., vasoconstriction and distal thrombus embolization. Thrombus formation and the v..... produced by platelet release of serotonin and thromboxane A2, results in myocardial i..... due to reduction of coronary b..... f..... | The common mechanism to all ACS is rupture or erosion of the fibrous cap of a coronary artery plaque. This leads to platelet aggregation and adhesion, localized thrombosis, vasoconstriction and distal thrombus embolization. Thrombus formation and the vasoconstriction produced by platelet release of serotonin and thromboxane A2, results in myocardial ischaemia due to reduction of coronary blood flow. |
| 984 Describe the emergency Ix that should be performed to confirm the Dx of MI. | * ECG * Bloods - FBC, U & E, glucose, lipids * Cardiac enzymes - CK and cTnT should be requested on ADx, and 3 hrs from ADx in all pt's with CP with the possible Dx of acute MI. If clinical suspicion persists, or the pt is at high risk, a further sample should be taken at 6-10 hrs from admission. In accordance with the new universal definition of MI, an ^in troponin by more than 7 ng/L to above 14 ng/L with appropriate clinical features is required for a definitive Dx of MI. An ^from < 14ng/L to more than 200 ng/L is highly suggestive of AMI. SGUL Greybook. |
| 985 Give criteria for Dx of MI. | Acute MI is defined by several criteria: * An↑ and then a ↓ in cardiac biomarkers (eg troponin - ^by >7 ng/L to >14 ng/L + appropriate clinical features is required for a definitive Dx of MI. An ^from < 14ng/L to >200 ng/L is highly suggestive of AMI) + either: * Sx of ischaemia or * ECG changes of new ischaemia or * Development of pathological Q waves or * Loss of myocardium on imaging. OHCM p112. |
| 986 What are two key questions in determining Rx/Mx of ACS? | 1) Is there ST elevation? 2) Is there a rise in troponin? - if not then unlikely that myocardial damage has occurred. OHCM p112. |
| 986 Describe the immediate Mx of a pt with STEMI. | ECG -> Bloods - FBC, U & E, glucose, lipids, cardiac enzymes -> Brief assessment - Hx (don't forget risk factors), examination, CI's to PCI or fibrinolysis? -> Aspirin 300mg -> Morphine 5-10mg IV + antiemetic eg metoclopramide 10mg IV -> STEMI on ECG & PCI available within 120/60? Yes -> PPCI. No -> Fibrinolysis -> Transfer to PPCI centre for either rescue PCI if fibrinolysis unsuccessful or for angiography. OHCM p809. |
| 986 Describe the immediate Mx of a pt with NSTEMI. | *Adx* to CCU -> *SaO2* <90% or breathless, low flow O2 -> *analgesia* eg morphine 5-10mg IV + metoclopramide 10mg IV -> *Nitrates* GTN spray or tablets -> *Aspirin* 300mg PO & *2nd antiplatelet* (eg clopidogrel, ticagrelor) unless contraindicated -> *Beta-blocker* PO eg metoprolol 50mg/12 hrs if HT/tachycardic/LV function <40% if contraindicated (asthma, COPD, LVF, bradycardia, coronary spasm) give rate-limiting calcium aantaagonist (eg verapamil 80-120mg/8 hrs PO or diltiazem 60-120mg/8 hrs PO -> *Fondaparinux* 2.5mg OD subcut or *LMWH* 1mg/kg/12 hrs subcut -> IV nitrate if P continues, (GTN 50mg in 50mL 0.9% saline + maintain systolic >100mmHg -> Record ECG whilst in P. If low risk pt -> may be Dx if a repeat trroponin is -ve. Rx medically & arrange further Ix eg stress test, angiogram. If high risk pt (^troponin, ST/T wave changes, DM, CKD, LVEF <40%, early angina post MI, recent PCI, BABG, intemediate-high GRACE score) -> infusion of GPIIb/IIIa antagonist & refer for angiography as an in-pt (speed dependent on risk but within 72/24). OHCM p811. |
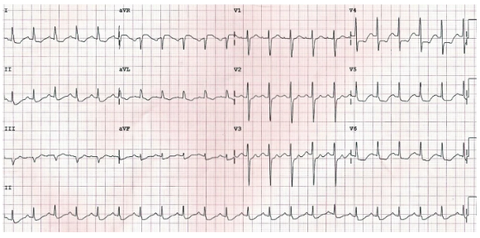
| ST depression due to subendocardial ischaemia is usually widespread — typically present in leads I, II, V4-6 and a variable number of additional leads. A pattern of widespread ST depression plus ST elevation in aVR > 1 mm is suggestive of left main coronary artery occlusion. ST depression localised to a particular territory (esp. inferior or high lateral leads only) is more likely to represent reciprocal change due to STEMI. The corresponding ST elevation may be subtle and difficult to see, but should be sought. In this eg - widespread subendocardial ischaemia due to LMCA occlusion http://lifeinthefastlane.com/ecg-library/myocardial-ischaemia/ | |
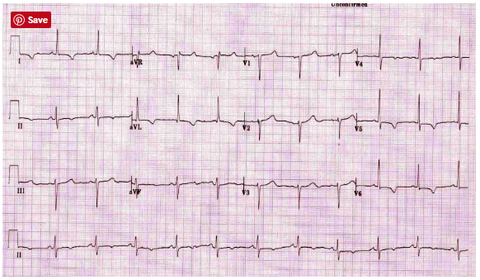
| T wave inversion may be considered to be evidence of ischaemia if: At least 1 mm deep Present in ≥ 2 continuous leads that have dominant R waves (R/S ratio > 1) Dynamic — not present on old ECG or changing over time. In this eg - widespread T wave inversion due to myocardial ischaemia (most prominent in the lateral leads. http://lifeinthefastlane.com/ecg-library/myocardial-ischaemia/ | |
| 992 Unstable angina refers to angina of recent onset (<..... h) or a deterioration in previous s..... a..... with Sx frequently occurring at ....., i.e. acute coronary syndrome | Unstable angina refers to angina of recent onset (<24 h) or a deterioration in previous stable angina with symptoms frequently occurring at rest, i.e. acute coronary syndrome K & C p729. |
| 992 What is the difference between unstable angina & NSTEMI? | The difference between UA & NSTEMI is that in the latter there is occluding thrombus, which leads to myocardial necrosis & ^serum troponins or CK-MB. MI occurs when cardiac myocytes die due to myocardial ischaemia, and can be diagnosed on the basis of appropriate clinical Hx, 12-lead ECG & ^biochemical markers – troponin I and T, CK-MB. K & C p733. |
| 993 Describe S & Sx of unstable angina. | * ^Frequency of CP (common) * P occurs daily or several times/day, instead of occasionally. * ^Severity of CP (common) * Decreasing levels of activity needed to trigger CP & may occur at rest. * Retrosternal CP radiating to jaw, arm, or neck (common) * Retrosternal pressure or heaviness radiating to the jaw, arm, or neck that is relieved or improved by nitrates. * Dyspnoea (common) * 4th HT sound (S4) (common). http://bestpractice.bmj.com/best-practice/monograph/149/diagnosis/history-and-examination.html |
| 994 List Ix that should be performed in a pt with unstable angina. | * ECG * Bloods - FBC, U & E, glucose, lipids * Cardiac enzymes - troponin, CK. OHCM p112. |
| 995 Immediate Mx of unstable angina. | Non-ST-elevation acute coronary syndrome * 1st - antiplatelet therapy (aspirin & ticagrelor) plus * Beta-blocker or calcium-channel blocker plus * Statin adjunct * Intravenous nitrate therapy adjunct * ACE inhibitor If early invasive approach planned plus * Anticoagulation plus * Early coronary catheterisation and intervention plus * Glycoprotein IIb/IIIa inhibitor If invasive approach not planned (ischaemia-guided therapy) plus * Anticoagulation plus * Glycoprotein IIb/IIIa inhibitor. http://bestpractice.bmj.com/best-practice/monograph/149/treatment/details.html |
| 995 Ongoing Rx for a pt with confirmed unstable angina. | * 1st antiplatelet therapy plus * Statin ± ezetimibe adjunct * Beta-blocker adjunct * ACEi plus * Cardiac rehabilitation. http://bestpractice.bmj.com/best-practice/monograph/149/treatment/details.html |
| 997 List indications for urgent cardiological intervention. | * Primary PCI should be offered to all STEMI pt's who are at or can get to a primary PCI centre within 120/60 of 1st medical contact. If this isn't possible they should receive fibrinolysis and then be transferred to a primary PCI centre. * Pt's with acute NSTEMI coronary syndromes are classed as high risk if there's a ^ in troponin, dynamic ST/T wave changes, or secondary criteria (DM, CKD, LVEF <40%, early angina post MI, recent PCI, BABG, intemediate-high GRACE score) and should be referred for angiography as an in-pt. OHCM p809-811. |
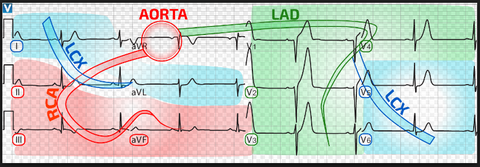
| 998 Describe which vessels supply which myocardiaal regions. | The *RCA* arises from the right coronary sinus & courses through the R side of the AV groove, giving off vessels that supply the *R atrium & the RV*. The vessel usually continues as the posterior descending coronary artery, which runs in the posterior interventricular groove and supplies the *posterior part of the interventricular septum and the posterior LV wall.* Within 2.5 cm of its origin from the L coronary sinus, the L main coronary divides into the *LAD* artery and the *circumflex* artery. The LAD artery runs in the anterior interventricular groove & supplies the *anterior septum & the anterior LV wall*. The *L circumflex* artery travels along the L AV groove & gives off branches to the *L atrium & the LV* (marginal branches). The *SA node & the AV node* are supplied by the *RCA* in about 60% and 90% of people, respectively. The majority of the *LV* is supplied by the *LCA* & DS in this vessel can cause significant myocardial dysfunction. K & C p672. |
| 999 Explain how an ECG can be used to determine the site of MI & indicate which vessel is occluded. | |
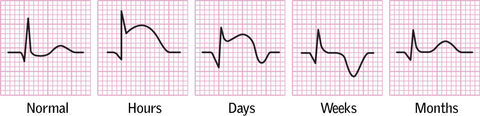
| 1000 Describe the evolution of ECG changes following an MI. | |
| 1002 List complications of MI. | * Cardiac arrest * Unstable angina: * Bradycardias or HT block * Tachyarrhythmias * RV failure * Pericarditis * DVT & PE * Systemic embolism * Tamponade * Mitral reguritation * Ventricular septal defect * Late malignant ventricular arrhythmias * Dressler's syndrome - recurrent pericarditis, pleural effusions, fever, anaemia, & ^ESR 1-3/52 post MI * LV aneurysm. OHCM p1116. |
| 1007 List drugs proven to improve prognosis following MI and give evidence supporting their use. | • Aspirin (eg 75mg) ↓vascular events (MI, stroke, or vascular death) by 29%. • Long-term β-blockade ↓mortality from all causes by ∼25% in pt's who have had a previous MI (eg bisoprolol 2.5–5mg/d enough to decrease the pulse to ≤60; continue for at least 1yr). If CI, consider verapamil or diltiazem. • Continue ACEi in all pt's. ACEi in those with evidence of HF reduces 2yr mortality by 25–30%. • Start a statin, eg simvastatin 40mg.35 Cholesterol reduction post-MI has been shown to be of benefit in pt's with both ^ & normal cholesterol levels. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Möchten Sie mit GoConqr kostenlos Ihre eigenen Karteikarten erstellen? Mehr erfahren.