6708257
Beschreibung
Karteikarten von Andrew Street, aktualisiert more than 1 year ago
|
|
Erstellt von Andrew Street
vor etwa 8 Jahre
|
|
| Frage | Antworten |
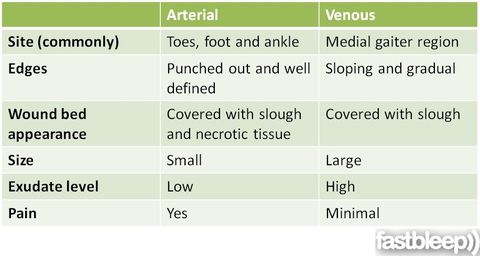
| 3601 Compare & contrast the presentation of venous & arterial leg ulcers | |
| Venous ulcer - note the pigment staining of the skin. | |
| Arterial ulcer | |
| 3602 Venous ulcers are the result of sustained venous h..... in the superficial ....., owing to incompetent v..... in the deep or perforating veins or to previous deep vein t...... The increased pressure causes extravasation of f..... through the capillary walls, giving rise to perivascular fibrin deposition, which leads to poor o..... of the surrounding skin. | Venous ulcers are the result of sustained venous *hypertension* in the superficial *veins*, owing to incompetent *valves* in the deep or perforating veins or to previous deep vein *thrombosis*. The increased pressure causes extravasation of *fibrinogen* through the capillary walls, giving rise to perivascular fibrin deposition, which leads to poor *oxygenation* of the surrounding skin. K & C p1226. |
| 3602 Arterial insufficiency refers to poor blood circulation to the lower leg and foot and is most often due to ..... In atherosclerosis the arteries become narrowed from deposits of fatty substances in the arterial vessel walls, often due to high levels of circulating c..... and aggravated by s..... and h..... The arteries fail to deliver oxygen and nutrients to the leg and foot resulting in tissue breakdown. | Arterial insufficiency refers to poor blood circulation to the lower leg and foot and is most often due to *atherosclerosis*. In atherosclerosis the arteries become narrowed from deposits of fatty substances in the arterial vessel walls, often due to high levels of circulating *cholesterol* and aggravated by *smoking* and *hypertension*. The arteries fail to deliver oxygen and nutrients to the leg and foot resulting in tissue breakdown. http://www.dermnetnz.org/topics/leg-ulcers/ |
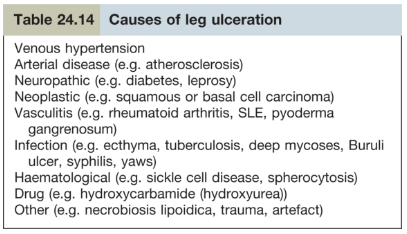
| 3603 List causes of leg ulceration. | |
| Outline how leg ulcers should be assessed. | * Site * Size * Shape * Number * Base/floor/edge * Surrounding skin * Examination of arterial, venous, lymphatic, & neurological systems * Nutritional status * Comorbidities * ABPI (AP/BP) * Duplex scan of vessels * FBC, ESR, renal, LFT's * Angiography * Biopsy From lecture: https://www.dropbox.com/home/P-Year%20Surgical%20Lectures?preview=Year+leg+ulcers+-+Miss+J.+Odili.pptx |
| 3604 Mx of leg ulcers. | * Debridement - medical or surgical * Dressings - reduce bacteria, moist environment, absorb effluent, protect granulation tissue, reduce P * Off-load pressure * 4 layer compression bandaging - improves healing rate * Optimise nutrition - protein, zinc, vitamin C * Relieve P * ABx only if infected * Avoid prolonged standing - exercise is good * Surgery: > Venous ulcers - strip varicose veins, reconstruct deep veins > Arterial ulcers - angioplasty, arterial bypass > Skin grafts From lecture: https://www.dropbox.com/home/P-Year%20Surgical%20Lectures?preview=Year+leg+ulcers+-+Miss+J.+Odili.pptx |
| 3605 Primary prevention of chronic venous insufficiency. | * Avoiding prolonged sitting or standing * Weight control * Smoking * Exercising * Intermittently elevating the leg may be helpful * Aggressive prophylaxis against DVT, particularly for pt's admitted to hospital, may reduce the incidence of CVI, as it occurs in as many as 50% of people within 5 to 10 years of an episode of DVT * Compression stockings for high risk pt's - eg strong FHx, standing occupations http://bestpractice.bmj.com/best-practice/monograph/507/prevention/primary.html |
| 3605 Secondary prevention of chronic venous insufficiency. | Prolonged standing should be avoided. If not possible, compression stockings should be worn. If obese, pt's should be advised to lose weight. Pt's with severe CVI or previous ulcers generally require lifelong graded compression stockings of at least 30 to 40 mmHg. Compliance with compression therapy markedly reduces, but does not eliminate, long-term sequelae. http://bestpractice.bmj.com/best-practice/monograph/507/prevention/secondary.html |
| 3606 Pathophysiology of pressure sores. | Ischaemia caused by capillary occlusion may be the dominant factor - other explanatory factors exist. Blockage of lymphatic flow may lead to ^toxic waste products. Reperfusion injury with the accompanying free radical development may damage cells. Prolonged pressure may directly damage cells, leading to cell death. Highest pressures are seen in deep tissues, especially along bony prominences. These deep tissues also appear to be most susceptible to pressure damage. Consequently, pressure often causes extensive deep tissue injury with little apparent damage initially in the more superficial tissues.These deep tissue injuries may then initially present as an area of dark purple discoloration with intact overlying skin. This lesion may then evolve over the course of several days or weeks to a large necrotic ulcer with extensive undermining of the wound edges. http://bestpractice.bmj.com/best-practice/monograph/378/basics/pathophysiology.html |
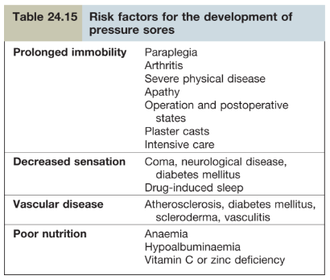
| Risk factors for developing pressure sores. | |
| 3608 & 3609 Prevention & Rx of pressure sores. | Prevention: * Good nursing practice - use of risk assessment tools, regular/prescribed turning, air mattresses, etc * MDT approach - eg Tissue Viability Nurse Rx: * Bed rest with pillows & fleeces to keep pressure off bony areas & prevent friction * Air-filled cushions for pt's in wheelchairs * Special pressure-relieving mattresses & beds * Regular turning but avoid pressure on hips * Ensure adequate nutrition * Non-irritant occlusive moist dressings (e.g. hydrocolloid) * Adequate analgesia (may need opiates) * Plastic surgery (debridement & grafting in selected cases) * Rx of underlying condition. K & C p1228. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Möchten Sie mit GoConqr kostenlos Ihre eigenen Karteikarten erstellen? Mehr erfahren.