4090904
Description

Flashcards by Natashia Reyes, updated more than 1 year ago
|
|
Created by Natashia Reyes
about 10 years ago
|
|
| Question | Answer |
| Who does Spinal Cord Injuries Occur Most With | 16-30 y/o men |
| How soon do Hemorrhagic Areas of the Spinal Cord Appear | Within one hour and up to 4 hours after infarction they may be seen in gray matter |
| WHen is the Extent of Injury and Prognosis most Accurately Determined | At least 72 hours or more after injury |
| What is Spinal Shock | Decrease in reflexes, loss of sensation, flaccid paralysis below level of injury days to months and may mask post injury neurologic function |
| What is Neurogenic Shock What Level of Injury is it Usually Associated With | In contrast to spinal shock it is d/t loss of vasomotor tone caused by injury characterized by hypotension and bradycardia WARM DRY SKIN below injury. Loss of sympathetic innervation =vasodilation, venous pooling, &dcrsd cardiac output. T6 or above (cervical or high thoracic) |
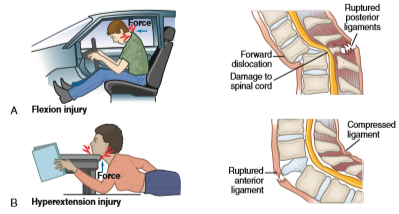
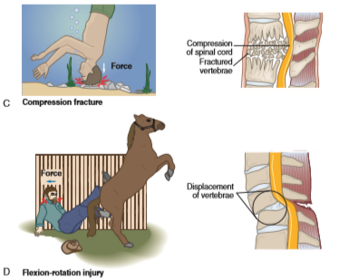
| How Are SCIs Classified | Mechanism, level, and degree of injury |
| What is the worst Mechanism of Injury in SCI | The flexion rotation injury because the ligamentous structures that stabilize the spine are torn |
| What Are the Mechanisms of SCI Injury | |
| What Are the Mechanisms of SCI Injury | |
| Levels: What Happens if the Cervical SC is Injured vs. Thoracic, Lumbar, or Sacral | The pt usually becomes a tetraplegic (formerly quadraplegia) though if low cervical then the arms are rarely fully paralyzed--- others are mostly paraplegics |
| Degree: What is Complete Vs. Incomplete (partial) Injury | Complete is total loss of sensory and motor function below level of injury partial is mixed loss of voluntary motor activity and sensations. |
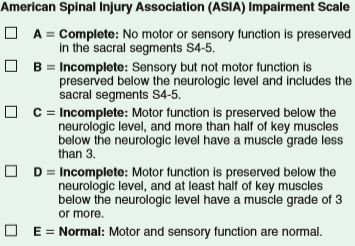
| What is a Good Scale for Classifying the SCI | The American Spinal Cord Injury Association Impairment Scale which combines assessments of motor and sensory function and is useful for recording changes and identifying appropriate goals for rehabilitation |
| What is the Physiological Response in a Patient with a C4 Injury | Total loss of respiratory function, mechanical ventilation required to keep the patient alive |
| What is the Physiological Response in SCI below C4 | Diaphragmatic breathing if phrenic nerve is functioning, in which hypoventilation almost always occurs because of decreased vital capacity and tidal volume |
| What is the Effect on Pt with Cervical and Thoracic SCI | Paralysis of abd muscles and often intercostals so pt cannot cough effectively enough to remove secretions, leading ot atelectasis and pneumonia |
| If the Pt has an Artificial Airway, is Older Adult, or Reduced Vital Capacity & Loss of Abd & Intercostal Muscle Function what are Extremely Important Measures | bronchial hygiene and Chest Physiotherapy are extremely important measures to reduce infection---Aggressive |
| What Happens to the Cardiovascular System with Injuries Above T6 What Kind of Monitoring is Necessary What Rate Requires Intervention & What Kind | decrease in effect of sympathetic NS, bradycardia, peripheral vasodilation resulting in hypotension, relative hypovolemia. Cardiac monitoring, heart rate below 40 drug Atropine to increase heart rate and prevent hypoxemia. Vasopressors for |
| What are the Effects of SCI @: C4 @C6 @T6 @L1 | |
| What is the ASAI Scale Classification of Injury | |
| What is the Response Acute Response of the Urinary and Post-Acute | Urinary retention and bladder atonic and overdistended typically in S2-4, indwelling cath may be inserted. Postacute hyperirritable, loss of inhibition, reflex emptying. Anticholinergic for supression of contractions oxybutynin (Ditropan), tolterodine (Detrol) or A Adrenergic terazosin (Hytrin), doxazosin (cardura) for relaxation decreasing spasticity |
| GI: What is the Effect on Pt if Injury is @ T5 or Above & What are Interventions for This | Primary effect is hypomotility which may contribute to paralytic ileus and gastric distention. NG tube for intermittent suctioning may relieve gastric distention. Metoclopramide (reglan) may treat delayed emptying. Stress ulcers may also develop |
| GI: How can Intraabdominal Bleeding be Identified if patient has SCI and May Not Experience Pain or Tenderness | Continued Hypotension in spite of vigorous treatment and decreased Hemoglobin 14-18 men 12-16 women & hematocrit (42-52% men, 37-47% women) and expanding girth |
| GI: What Happens W/To the Bowels During SCI How are These Conditions Manageable | during spinal shock in early period & with injury T12 or below bowel is areflexic sphincter tone decreased later reflexic and sphincter tone enhances and reflex emptying occur both manageable with bowel program coordinated with gastrocolic reflex |
| What Happens to Thermoregulation with SCI | Poikilothermism-the adjustment of body temperature to room temp b/s interruption of sympathetic NS & w/ spinal cord disruption decreased ability to sweat or shiver below injury occurs so higher has greater loss to regulate temp |
| What May Occur w/ NG Suctioning What Needs to be Monitored What is Normal Loss with SCI and what Diet is Needed | Metabolic Alkalosis, electrolytes such as sodium 136-145 and potassium 3.5-5.0 must be monitored until discontinued and normal diet. Loss of weight greater than 10% common greater nutritional needs high protein diet prevents breakdown and atrophy |
| What may Decreased Tissue Perfusion Cause What is a Primary Problem with SCI MOst Highly Occurring in the First Three Months | Acidosis DVT |
| Cord Injury and Rehabilitation Potential: C1-C3 | C1-3: Often fatal move neck and up, loss of diaphragm innervation and respiratory function R-can drive electric wheelchair w/ portable ventilator by chin or mouth stick, headrest stabilizes head, computer use w/mouth stick, head wand, or noise control 24hr day attendant needed |
| Cord Injury and Rehabilitation Potential: C4 | Same as CS rehab, but injury may be able to breath without ventilator |
| Cord Injury and Rehabilitation Potential: C5 | Full neck, partial shoulder, back, biceps, gross elbow, inability to roll over or use hands & decreased respiratory reserve R--drive electric wheel chair with mobile hand supports, indoor mobility in manual wheelchair feeds self with adaptive equipment attendant 10hr/day |
| Cord Injury and Rehabilitation Potential: C6 | I-Shoulder & upper back abduction & rotation @ shoulder, full biceps to elbow flexion, wrist extnsn, weak thumb grasp, dcrsd respiratory reserve R--Cn assist w/transfer, perform sm self care, feed self w/hand devices, push w.c on smooth/flt surface, drive adapted van from w.c, indep comp use w adap equip 6hr/day attndt |
| Cord Injury and Rehabilitation Potential: C7- C8 | I-Triceps to elbow extnsn, finger extnsr and flxr, good grasp some dec strngth, decrsd resprtry rsrv R--transfers self to w/c, push self off most surfaces, perform most self care, independent use of w/c, drive car with powered hand controls (some) 06hr/day attendant |
| Cord Injury and Rehabilitation Potential: T1-T6 | I-Full innervation of upper extremities, finger extens/flexors, back, essential intrinsic hand muscl, full strength & dexterity of grasp. Decreased trunk stability, decreased repiratory reserve. REHAB-Full independence in self care and w/c drive car with hand control (most) independent standing in standing frame |
| Cord Injury and Rehabilitation Potential: T6-T12 | I--Full, stable thoracic muscles and upper back, functional intercostals, increased respiratory reserve REHAB-a-Full independent use of w/c ability to stand erect with full leg brace, ambulate on crutches w/ swing (gait difficult) inability to climb stairs |
| Cord Injury and Rehabilitation Potential: L1-L2 | Varying control of Pelvis, instability of lower back REHAB_Good sitting balance, full use of wheelchair, ambulation with long leg braces |
| Cord Injury and Rehabilitation Potential: L3-L4 | Quadriceps and hip flexors, absence of hamstring function, flail ankles REHAB-completely and independent ambulation with short leg braces and canes, inability to stand for long periods |
| What are Diagnostics Used With SCI Which is the Preferred Method What if Preferred is Unavail What if Changing Neurologic Stats What if Changing Mental Stats | CT is PREFERRED, Cervical X ray if CT unavail but no C7 or T1 viewable, MRI for soft tissue and neurological deficits when or Neuro status is changing. Altered Mental Status do a CT angoigram to rule out vertebral artery damage |
| What Diagnostics can be used for DVT | Duplex doppler ultrasound, impedance plethysmography, venous occlusion plethysmography, venography, clinical exam |
| What SCI is considered Blunt Trauma What is Considered Penetrating Trauma | Compression, flexion, extension, rotational, MVA, Pedestrian incidents, falls, diving--- Stretched, torn, crushed, or lacerated spinal cord, gunshot wounds, stab wounds |
| What is Characteristic of Neurogenic Shock | Hypotension, bradycardia, and dry flushed skin |
| What are Inital Interventions that Should Be Instituted | Ensure patent airway, immobilize and stabilize cervical spine, admin )2 via nasal cannula or nonrebreather mask, establish IV access w/two large bore catheters (18 gauge) to infuse NS or LR, assess for other injuries, control bleeding, obtain CT or cervical spine X-ray |
| What Ongoing Monitoring Should the Nurse Be Performing | Monitor vital signs, LOC, O2 sats, cardiac rhythm, urine output, keep warm, monitor for urinary retention, hypertension, ANTICIPATE NEED FOR INTUBATION IF GAG REFLEX IS ABSENT |
| What are Diagnostics that May Be Done During Cervical Cord Injury | hx, physical, complete neurologic exam, ABGs 7.35-7.45, Serial Bedside PFT, electrolyte, glucose, coagulation, Hemoglobin and Hematocrit, UA, CT, MRI, X-ray (anterior, odontoid, spinal) EMG to measure evoked potentials, duplex doppler, impedance plethysmography |
| What is the Focus of Acute Nursing Care with Cervical Cord Injury | Immobilization of the vertebral column, maintenance of heart rate (atropine) and b/p (dopamine (Intropin)), insertion of NG tube attached to suction, Intubation (if indicated by ABG or PFT, 02 by high humidity mask, indwelling cath, IV fluids, Stress ulcer prohpylaxis, bowel bladd training |
| What is the Recommended Immobilization with SCI Is it the Same if Pt has Penetrating SCI | Rigid cervical collar and supportive blocks with a backboard w/straps. Spinal immobilization with sand bags and tape is insufficient not recommended. In penetrating cases immobilization is NOT RECOMENDED. Biggest concern Neuro impairment frm vrtbr movement |
| How Should You as a Nurse Assess A Pt w/SCI: Muscles, Hands, Sensations | Assessment involves testing muscle groups(vs individual) w/& against gravity, alone and against resistance, on both sides, noting spontaneous movement. Ask pt to move legs then hands, spread fingers, extend wrists, shrug shoulders (all neuro asses) then sensory exam touch and pain by pinprick frm feet up |
| What is Relative to Musculoskeletal Injuries and Trauma | Internal trauma with hemorrhage sometimes only identifiable by rapidly increasing BP and pulse, urine, hgb & hct may be examined which are indicative of internal injuries |
| When is Early Surgery Typically Indicated | When cord compression is certain, neurologic disorder progresses-immediate surgery. Other criteria evidence of cord compression, progressive neuro deficit, compound fracture of vertebra, bony fragments (which may dislodge and penetrate cord), and penetrating wounds |
| When is a Fusion Procedure Typically Done | when two or more vertebra have been injured and involves attaching metal screws, plates, or others to bone of spine to help keep them aligned, sometimes small pieces of bone from hip used |
| When is Methylprednisolone (MP) used in SCI | Its NOT!!! Not any longer b/c high doses assoc with immunosuppression, increased upper GI bleeds, increased risk infection, sepsis, longer ICU stays, death. |
| When is Low-Molecular Heparin Utilized | enoxaparin (Lovenox) to prevent VTE unless internal bleeding or recent surgery, oral anticoagulation alone is not recommended as prophylactic tx |
| What Should Mean Arterial Pressure be Maintained @ & What Happens if it Falls Below | 90 mm Hg so that perfusion to spinal cord is improved, if it is lower or low vasopressors such as dopamine (Intropin) is used in the acute phase. |
| Neurologic Alterations Above C8 vs Below C8 Complete S&S | Flaccid paralysis and anesthesia below level of injury result tetraplegia above C8, paraplegia below, Hyperactive Deep Tendon reflexes, Bilateral Positive Babinski (fanning out, abn) Test (after resolution of spinal shock) |
| What Kind of Traction is Utilized in Cervical Injuries How Would You As a Nurse Describe This When Should You as a Nurse Remove This What if Your Pins are Dislodged | Crutchfield, Vinke, or Gardner-Wells tongs using a rope that extends form center of tongs over pulley with weights at end. Traction must be maintained AT ALL TIMES. May be removed 1-4 weeks after.--Hold head in neutral position, call for help, stabilize head while physician reinserts tongs NO SKELETAL TRACT |
| How Should You as a Nurse Care for the Tong Sites | Cleansing sites twice a day with normal saline and applying an antibiotic ointment that acts as a mechanical barrier to the entrance of bacteria |
| What is Kinetic Therapy What is Typical after Cervical Fusion or other Stabilization Surgery What is Typical for Stable Injury with No Surgery | Continuous side to side rotation to 40 degree or more to prevent pulmonary complications and prevent pressure ulcers.---Hard Cervical Collar, or sternal-occipital-mandibular immobilizer---Halo apparatus by means of life jacket |
| How are Patients with Thoracic or Lumbar Spine Injuries Immobilized and What Purpose Does it Serve | Custom thoracolumbar orthosis (Body Jacket) which inhibits spinal flexion, extension, and rotation, or with a Jewett brace which restricts forward flexion |
| In First 48 Hours Spinal Cord Edema May Increase What Situations Require Nursing Intervention and What Kind of Intervention | Injury @ or above C3, patient is exhausted from labored breathing or ABG indicates deterioration (as alkalosis indicates respiratory insufficiency and acidosis indicates inadequate tissue perfusion) init endotracheal intubation or tracheostomy and mechanical ventillation |
| What is an Acceptable PaO2 (Identify) & what is an Acceptable PaCO2 (Identify) Value for a Patient with Uncomplicated Tetraplegia What if your Pt Cannot Count to 10 Aloud W/O taking a Breath | Partial pressure of oxygen in arterial blood greater than 60 mm Hg & partial pressure of carbon dioxide in arterial blood Less than 45 mm Hg are acceptable values---IMMEDIATE Attention is needed |
| How can You as a Nurse Perform Assisted (Augmented) Cough Tecnique What Should you do if Crackles or Rhonchi | Place heels of both hands just below xiphoid process and exert firm upward pressure to area timed with patients efforts to cough which stimulation action of ineffective abdominal muscles during expiratory phase---Tracheal suctioning |
| How Should a Nurse Apply and Care for SCDs | Remove stockings every 8 hours for skin care, venous duplex studies may be performed before applying SCD, regular ROM exercises and stretching should be done and assess thighs and calves every shift for signs of DVT deep reddish color or edema, if in wheelchair lift self up & shift Q15-30min |
| During First 48-72 hours after SCI How does GI Tract React what are Interventions | may stop functioning, NG tube Must be inserted, b/c pt cannot have oral intake careful monitor of F&E needed. Once bowel sounds gradually reintroduce foods, if high cervical injury evaluate swallowing first. If inadeq intake make contract with pt encourage foods liked etc |
| How often is Intermittent Catheterization Done What if pt Urine Odor or Appearance Suspicious When Should a Bowel Program be Started and How | Best way to prevent UTI regular and complete bladder drainage, once stable start IC and do every 3-4 hours, send a specimen for culture. Bowel in cacute care, chose rectal stimulant to follow with manual evacuation, inital side lying posit, as soon as sitting then upright or bedside comode |
| Automic Dysreflexia S/S | Hypertension (up to 300 mm Hg systolic), Throbbing Headache, Marked Diaphoresis (above injury), Bradycardia (30-40 beats per minute), piloerection (goose pimples), flushing above injury, blurred vision or spots, nasal congestion, anxiety, nausea, MEASURE BP w/headache complnts |
| What are Nursing Interventions for Autonomic Dysreflexia | Elevate HOB to 45 degrees or sit patient upright, DETERMINE CAUSE most common bladder irritation, Immediate Cath Instill LIDOCAINE FIRST in urethra if cath already in place check for kinks or folds, if plugged do irrigation slowly and gently or insert new |
| What if Stool Impaction is Causing the Autonomic Dysreflexia What are your Nursing Interventions Now | Perform Digital Rectal exam ONLY AFTER application of anesthetic ointment to decrease rectal stimulation and avoid increasing symptoms. |
| What Other Nursing Interventions are Indicated for Autonomic Dysreflexia | Remove all skin stimuli like constrictive clothing or tight shoes, monitor BP frequently, if symptoms persist after source is relieved admin a-adrenergic blocker (nifedipine (Procardia)) continue to monitor until stable |
| What Would You Tache as S/S to Family & Pt | Sudden onset of acute headache, elevation in BP or reduction in pulse rate, flushed face & chest above injury and pale extremities, sweating above injury level, nasal congestion, feeling apprehension--raise to sitting, remove stimuli, call if unrelieved |
| How Much Should a Pt with Neurogenic Bladder Take In How Much if Indwelling Cath When May Cath Drainage Time Be Extended vs Shortened | 1800-2000 ml, 3-4 L per day, done every 4 hours if less than 200mL of urine time of interval may be extended, if more than 500mL time shortened usually 5-6 intermittent caths done per day |
| What Should You Teach a Pt and Family About Bowel Management After Spinal Cord Injury | Three well balanced meals, TWO servings milk group, Two or more meat group including poultry, eggs & fish, four + vegetables and fruit, four + breakfast cereal & bread. Fiber 20-30g/day, gradually increased over 1-2wk, 2-3 Quarts fluid per day |
| What Should You Teach a Pt and Family About Bowel Management After Spinal Cord Injury Part Two | Avoid Beans &Spicy Foods, evacuate bowels regular like 30 mins after first meal, if possible upright & feet flat or on stool, DON'T keep on toilet or bedpan longer than 20-30 min b/c breakdown. Stretching, ROM, position changing, & functional movement needed, manual stimulation may help Only Oral Lax if Necessary 1-2d, small vol enema 20-30 min after suppos, valsalva if t12 or lower |
| How to Care for Halo Vest | Clean around pin sites with hydrogen peroxide, water, or alcohol, for skin care pt should lie down with head on pillow loosen ONE side gently wash under then dry simutaneously check skin, if wet blow dry, mark vest strap for correct fit, keep sheepskin pad under vest, if perspiration or itching cotton t shirt |
| Psychogenic Erections/Vaginal Lubricants vs Reflexive Responses What Happens With Menstruation | Psychogenic Usually Occuring thorough T10-12 @ Reflexic S2-4. Menses may be interrupted 6 months after SCI |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.