8646368
Description
Mind Map by Fatma Shwaylia, updated more than 1 year ago
|
|
Created by Fatma Shwaylia
over 7 years ago
|
|
Mohammed's Spleen is Palpable
- Leukocytosis
- Causes of
Leukocytosis
- Nonneoplastic causes
- Neutrophilic leukocytosis
- Bacterial
infections
- Corticosteroids
- (inhibit
margination)
- (inhibit
margination)
- Myocardial
infarction
- Bacterial
infections
- Eosiniophilia
- Type I hypersensitivity reaction
- bronchial asthma
- reaction to penicillin
- bronchial asthma
- Helminthic infections
- Type I hypersensitivity reaction
- Monocytosis
- Chronic infections : Tuberculosis
- Autoimmune
- Inflammatory
Bowel disease
- Rheumatoid arthritis
- Systemic lupus
erythematosus
- Inflammatory
Bowel disease
- Chronic infections : Tuberculosis
- Lymphocytosis
- Viral infections (infectious
mononucleosis)
- Drugs (phynetoin)
- Viral infections (infectious
mononucleosis)
- Neutrophilic leukocytosis
- Neoplastic proliferations of the WBCs
- Leukemia Vs Lymphoma
- Leukemia
- Malignancy of the blood
- Can be in myeloid linage
- Tumor in the blood
- Most common
cancer in
childhood
- Types
- Acute myeloblastic leukemia(AML)
- Age : 15-60years of age
- 2.Thrombocytopenia – bleeding, bruising
- May present as discrete tissue masses (chloroma).
- Myeloblasts contain
intracytoplasmic
granules (Auer Rods ).
- 1.Neutropaenia – fever, chills, infections
- 3.Anemia – weakness, fatigue Might
have gingival involvement.
- Immunophenotype : CD13+,
Myeloperoxidase +
- Age : 15-60years of age
- Acute lymphocytic leukemia(ALL)
- 80% of childhood cases (age˂15 years
- composed of immature, precursor B (pre-B) or T
(pre-T) lymphocytes referred to as “Lymphoblasts”
- 85% of ALLs are precursor B-cell tumours(B-ALL)
- B-ALL: + CD10- CD19- CD20
- B-ALL: + CD10- CD19- CD20
- Less common, precursor T-cell
ALLs(T-ALL) often with thymic
involvement.
- T- ALL: + CD2- CD3- CD4-CD8
- T- ALL: + CD2- CD3- CD4-CD8
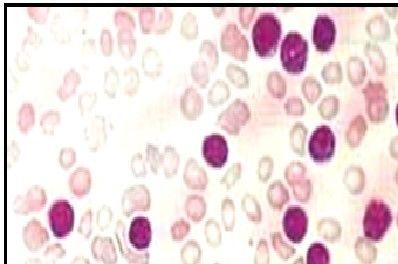
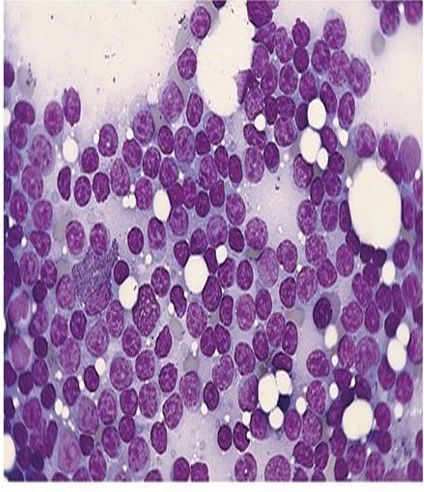
- Blood film showing blasts
- 85% of ALLs are precursor B-cell tumours(B-ALL)
- Abrupt onset –Bone marrow suppression – mass
–lymphadenopathy- splenomegaly.
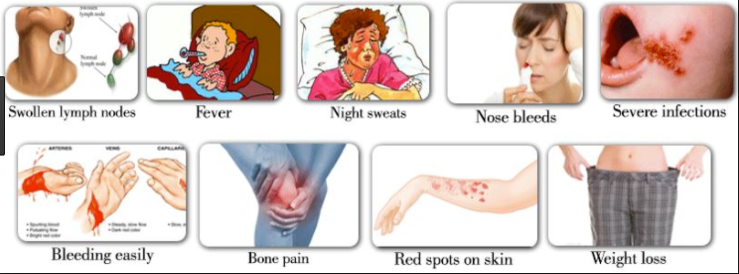
- Symptoms
- Fever-malaise-bleeding (petechial
bleeding)-mouth ulcers due to
infection.
- Fever-malaise-bleeding (petechial
bleeding)-mouth ulcers due to
infection.
- Immunophenotyping : + TdT
- 80% of childhood cases (age˂15 years
- Chronic lymphocytic leukemia (CLL)
- 60 +-----indolent
course(slowly growing
tumor)
- Proliferation of neoplastic lymphoid cells (B –cells)
- Widespread involvement of
Bm,peripheral blood,LNs,spleen
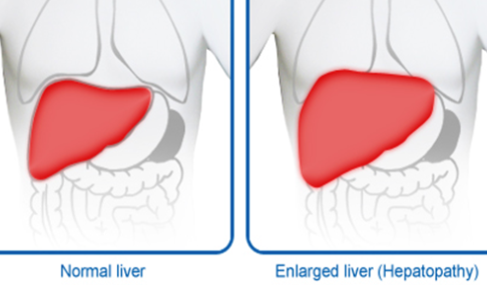
- hepatosplenomegaly- generalized
lymphadenopathy
- Increased WBC count….Absolute lymphocytosis
- Cells are susceptible to
destruction …smudge cells in
peripheral blood
- Immunedysregulation….Hypogammaglobulinemia
- Transformation to diffuse large B – cell lymphoma
- IHC: CD19+, CD20+,
CD23+, CD5+,
CD10.
- 60 +-----indolent
course(slowly growing
tumor)
- Acute myeloblastic leukemia(AML)
- Malignancy of the blood
- Lymphoma
- Malignancy of the
lymphoid tissue
- Only in lymphocytes
- Solid tumor
- Only 10% of
childhood cases
- Types
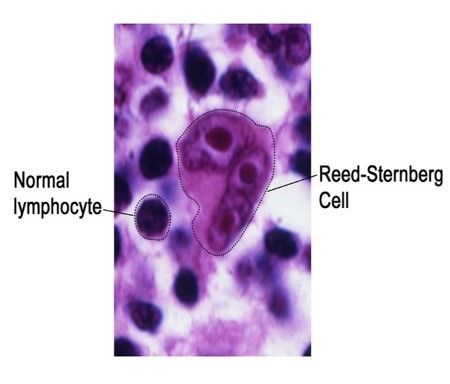
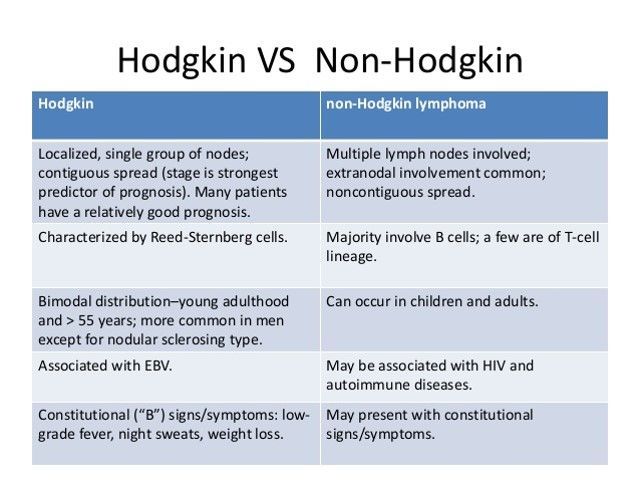
- Hodgkin’s
lymphoma
- presence of
reed-strenberg
cell.
- presence of
reed-strenberg
cell.
- Non-Hodgkin lymphoma:
- neoplastic
proliferation of B or T
cells
- neoplastic
proliferation of B or T
cells
- Hodgkin’s
lymphoma
- Malignancy of the
lymphoid tissue
- Leukemia
- Chronic Myeloproliferative disorders
- Hyperproliferation of neoplastic
myeloid progenitors while retaining
the capacity for terminal
differentiation
- 1-Chronic myelocytic leukemia (CML)
- clonal myeloproliferative neoplasm
- Dysregulated production and
uncontrolled proliferation of mature
and maturing granulocyte with fairly
normal differentiation
- Three stages:
Chronic Stage
Accelerated Stage
Blastic Stage
- Three stages:
Chronic Stage
Accelerated Stage
Blastic Stage
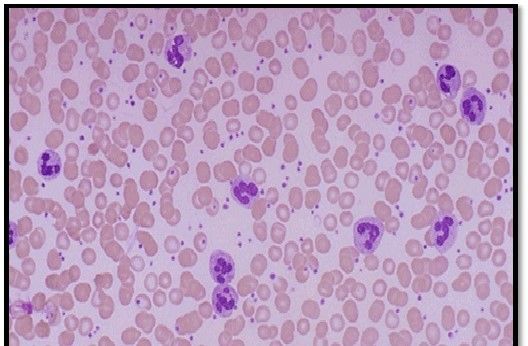
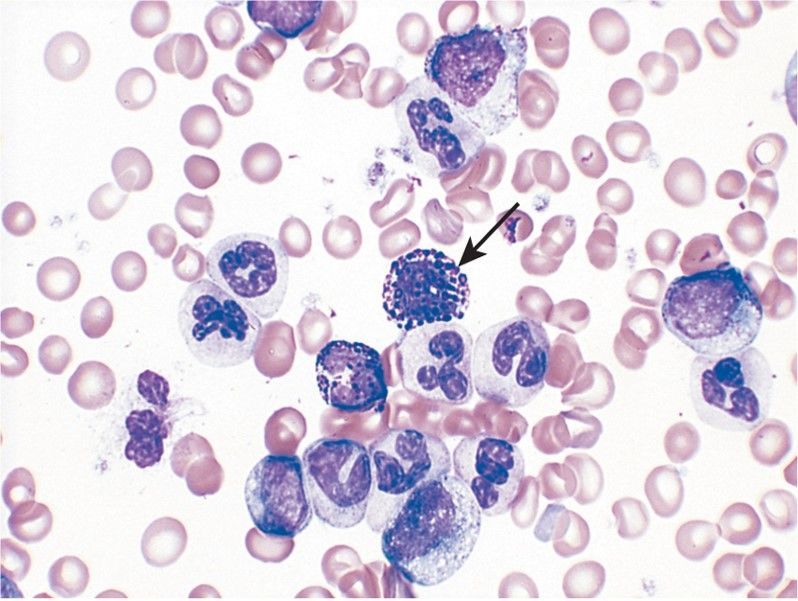
- CML: blood film showing marked leukocytosis ,
neutrophils at various stages of development
(segmented, band , metamyelocytes, myelocytes).
The cell in the centre is a basophil (basophilia is
prominent in CML) The bone marrow is
hypercellular owing to increased numbers of
granulocytic and megakaryocytic precursors.
- Dysregulated production and
uncontrolled proliferation of mature
and maturing granulocyte with fairly
normal differentiation
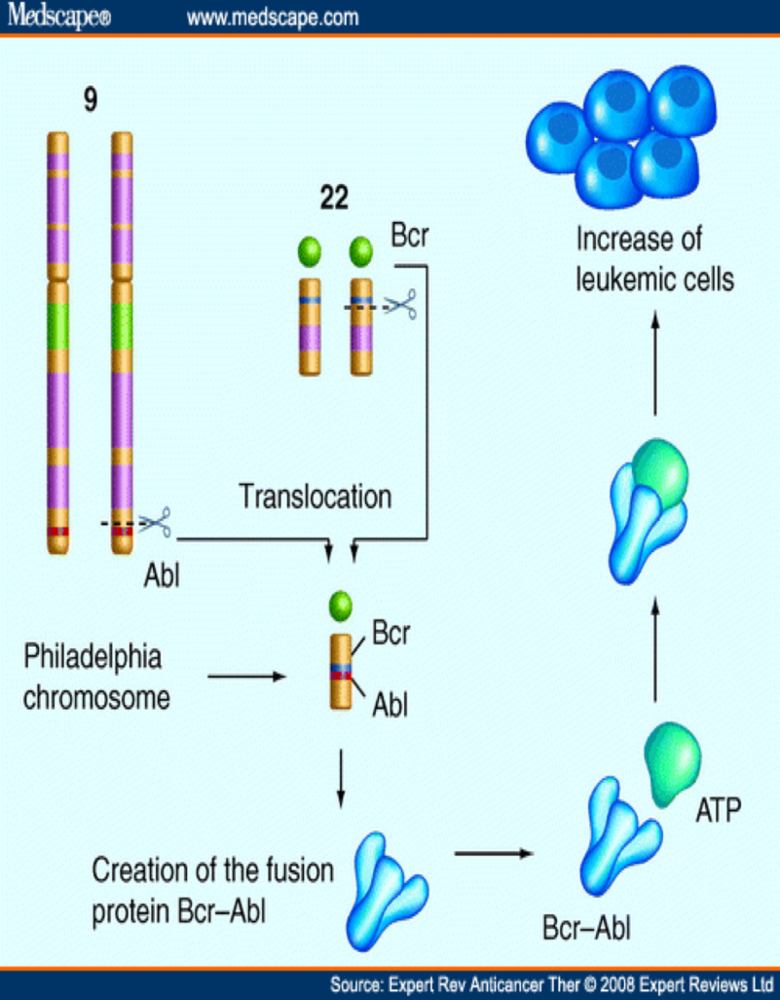
- Fusion of 2 genes
- BCR (or chromosome 22)
- ABL1 (on chromosome 9),
- resulting in BCR-ABL1 fusion gene
- Abnormal chromosome 22 called
Philadelphia (Ph) chromosome
- Final product: BCR-ABL1 fusion
protein, a dysregulated tyrosine
kinase
- Uncontrolled proliferation of
transformed cells/ Discordant
maturation/ Escape from
apoptosis/ Altered interaction
with the cellular Matrix
- Uncontrolled proliferation of
transformed cells/ Discordant
maturation/ Escape from
apoptosis/ Altered interaction
with the cellular Matrix
- A subset of patients with CML lack a detectable Ph
chromosome but have the fusion product for the
bcr/abl translocation detectable by reverse
transcriptase- polymerase chain reaction (RT-PCR)
- Final product: BCR-ABL1 fusion
protein, a dysregulated tyrosine
kinase
- Abnormal chromosome 22 called
Philadelphia (Ph) chromosome
- BCR (or chromosome 22)
- Management
- Pharmacological
- Tyrosine kinase inhibitors
- Imatinib
- dasatinib
- nilotinib
- bosutinib
- Ponatinib
- Imatinib
- Chemotherapy
- Interferon Therapy
- Tyrosine kinase inhibitors
- Non pharmacologcai
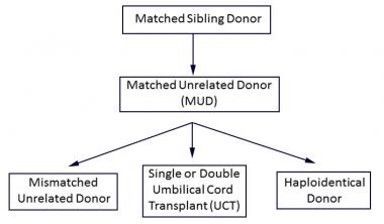
- Hematopoietic stem cell transplantation
- Radiation Therapy
- Hematopoietic stem cell transplantation
- Pharmacological
- clonal myeloproliferative neoplasm
- 1-Chronic myelocytic leukemia (CML)
- 2.Polycythemia vera
- 3.Myelofibrosis
- 4.Essential thrombocythemia
- JAK2 mutation, which normally promote growth and
division (JAK/STATA pathway) and it’s important
especially for controlling production of blood cells.
- JAK2 mutation, which normally promote growth and
division (JAK/STATA pathway) and it’s important
especially for controlling production of blood cells.
- Hyperproliferation of neoplastic
myeloid progenitors while retaining
the capacity for terminal
differentiation
- Leukemia Vs Lymphoma
- Nonneoplastic causes
- Leukocytosis refers to an increase in the total
number of WBCs due to any cause.
- if the leukocytosis is so severe,
it can mimic leukemia
"Leukaemoid Reaction"
- How to differentiate between leukemia
and a leukmoid reaction
- Leukaemoid Reaction
- WBC counts up to 15
- 100,000/mm3
- Shift to the left (immature WBCs)
- Shift to the left (immature WBCs)
- Signs of activation
- Doehle bodies
- toxic granulations
- NAP scores high (Differs the
condition from CML)
- MPO negative (Myeloperoxidase) to differ from CML
- Doehle bodies
- WBC counts up to 15
- 100,000/mm3
- Leukaemoid Reaction
- How to differentiate between leukemia
and a leukmoid reaction
- Causes of
Leukocytosis
- Hematological History Taking
- Anemia
symptoms
- Fatigue, weakness
- Blood in stools
- Easy bruising
- Heavy menstruation
- dyspnea
- Fatigue, weakness
- Lymphoid
symptoms
- Infections
- Infections
- Past medical, surgical history
- Frequent infections
- Bleeding disorders
- Radiotherapy
- Recent trauma
causing
bleeding
- Surgery to GI
- Transplant surgery
- Frequent infections
- Social history
- Smoking
- Alcohol
- origin
- Diet
- Sexual lifestyle
- Smoking
- Drug history
- Drug currently taking
- OTC’s especially NSAIDs
- Anticoagulant therapy
- Vitamins, supplements
especially Iron, B12
- Vitamins,
supplements
especially Iron, B12
- Allergies
- Drug allergies
- Drug currently taking
- Family history
- Same condition in
a family member
- Hemophilia, von willebrand’s
- Sickle cell anemia
- Thalassemia
- Leukemia (Philadelphia
chromosome)
- Same condition in
a family member
- Anemia
symptoms
- Hematological Physical Examination
- General Appearance
- Pale (anemia)
- Jaundice (hemolytic anemia).
- bruising
- Pale (anemia)
- Hands
- pallor of palm
- radial pluse
- Nails-koilonychia (iron deficiency).
- Pale nails (anemia).
- pallor of palm
- Forearms
- scratch marks
- Found on legs as well
- Found on legs as well
- purpura
(dysglobulinema)
- scratch marks
- Face
- Eyes
- Conjunctiva: pale (anemia).
- Sclera: jaundice
(hemolytic anemia)
- hemorrhages (polycythemia)
- Conjunctiva: pale (anemia).
- Mouth
- Gum hypertrophy (leukemia).
- Gum bleeding-scurvy (Vit C).
- Gum hypertrophy (leukemia).
- Tongue:
- glossitis (iron
deficiency,
megaloblastic
anemia).
- glossitis (iron
deficiency,
megaloblastic
anemia).
- Eyes
- Trochlear & axillary nodes
- Cervical & supraclavicular nodes
- Rectal and pelvic
examination
- (blood
loss).
- (blood
loss).
- Fundi
- hemorrhage , infection
- hemorrhage , infection
- Chest & abdomen
- Enlarged liver
- Enlarged liver
- inguinal nodes
- General Appearance
- Investigations
- Blood film
- To differ the type of Blast: Myeloblast or Lymphobast (AML or ALL?)
- To study the RBC count and morphology
- size and shape of the cells in the samples
- Determine the Blast count
- To differ the type of Blast: Myeloblast or Lymphobast (AML or ALL?)
- Confirming tests
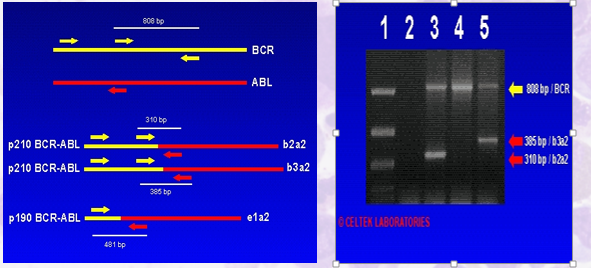
- PCR
- is more sensitive than
FISH
- can be used to monitor
the expression
quantitively
- Polymerase chain reaction is a DNA test that
can find the BCR-ABL fusion gene and other
molecular abnormalities. PCR tests may also
be used to monitor how well treatment is
working. This test is quite sensitive and,
depending on the technique used, can find 1
abnormal cell mixed in with approximately 1
million healthy cells. This test can be done
using a blood sample or bone marrow cells.
- is more sensitive than
FISH
- FISH
- Fluorescence in situ hybridization (FISH) is a test used to detect the BCR-ABL gene and to monitor the
disease during treatment. This test does not require dividing cells and can be done using a blood
sample or bone marrow cells. This test is a more sensitive way to find CML than the standard
cytogenetic tests that identify the Philadelphia chromosome.
- Fluorescence in situ hybridization (FISH) is a test used to detect the BCR-ABL gene and to monitor the
disease during treatment. This test does not require dividing cells and can be done using a blood
sample or bone marrow cells. This test is a more sensitive way to find CML than the standard
cytogenetic tests that identify the Philadelphia chromosome.
- Bone marrow aspiration and biopsy
- A bone marrow aspiration removes a sample of the fluid with a needle.
- A bone marrow biopsy is the removal of a small amount of solid tissue using a needle.
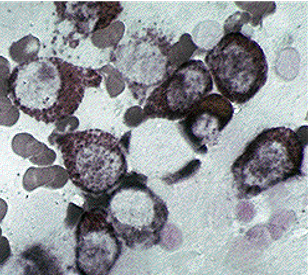
- Peripheral blood smear showing leukocytosis with increased number of blasts (MGG-Giemsa stain,
x400) (a). Bone marrow aspirate showing megakaryocyte and myeloid cells with excess of blasts
(MGG-Giemsa stain, x200, x1000) (b and c). Bone marrow biopsy is hypercellular with myeloid and
megakaryocytic hyperplasia (Hematoxylin and Eosin, x400) (d)
- A bone marrow aspiration removes a sample of the fluid with a needle.
- PCR
- CBC
- To make a total & differential WBC count
- Increase in granulocytes
- Decrease in Lymphocytes (due to dilution in the differential
count) A mild increase in basophils and eosinophils is present
- Number of blasts and Promyelocytes and metamyelocytes is ↑
- The platelet counts at diagnosis can be low, normal, or even increased in some patients
- Increase in granulocytes
- Determine the Blast count
- Too many immature white blood cells ( Total WBC ↑) above 20,000-60,000 cells/μL
- To make a total & differential WBC count
- Blood film
Media attachments
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Mind Maps for free with GoConqr? Learn more.