Page 1
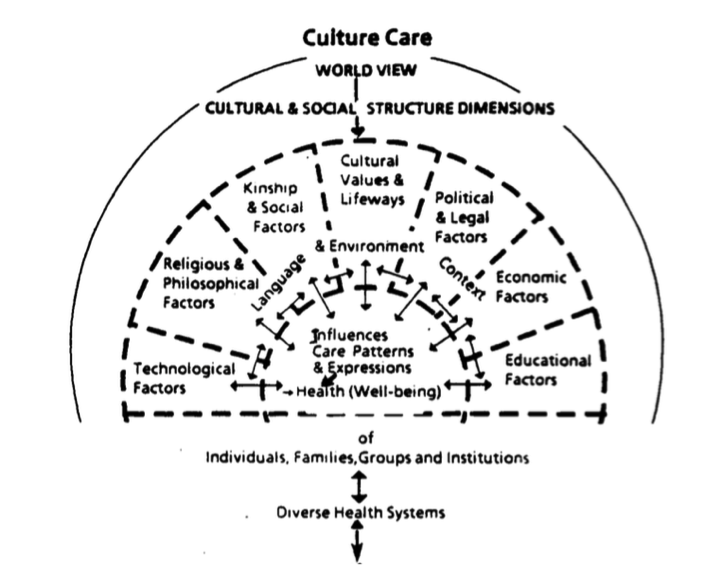
No More Tears for Henry Learning Aims: 1. Understand the complexities of fluid and electrolyte imbalances in children - Dawn 2. Explore health care values from a transcultural perspective - Michelle3. Identify the impact of a child's illness on individual family members and the family. Apply family theory in caring for children and caregivers - Mary Required Reading: Managing acute gastroenteritis among children: Oral rehydration, maintenance, and nutritional therapy. MMWR: Morbidity & Mortality Weekly Report, 52(RR-16), 1-16. Retrieved from http://www.cdc.gov/mmwr/index.html Canadian fundamentals of nursing (5th ed.). Toronto, ON: Elsevier (pg. 339-345) Learning Activities for Students Utilize the a family assessment tool to guide interviewing Henry’s mother in a role playing situation - CALGARY Assessment tool - Kate Have students contact a resource agency to learn more about the Mennonite culture and share findings with group - Gabriella No More Tears for Henry…Chart Data History of present problem: 2 day history of vomiting and diarrhea; not eating or drinking well Mother states Henry felt “warm” to touch Decreased appetite, refusing solids, Henry is drinking small amounts of chamomile tea Sleeping poorly Helen reports that Henry has been lethargic, irritable and clingy the last 2 days Health History: Mother states her pregnancy with Henry was normal He was born at 40 weeks gestation; uneventful labour and delivery His immunizations are up to date. Family History: Helen is 23 years old. Husband, Peter, is 28 years old. At age 2, Henry is the youngest of three children. He has a brother who is 3 and a sister who is 4 ½ years. Gordon’s Functional Health Patterns 1. Health Perception - Health Management: Folk remedies are frequently used in this culture. Helen believes the chamomile tea is helping with Henry’s symptoms. When Henry has had an ear infection in the past, he has taken Tylenol to help his symptoms. The family has a pattern of seeking medical care late in an illness 2. Nutrition/Metabolic: Henry was breastfed until 1 year of age. He now drinks milk, water or juice from a Sippy cup. He is able to hold his own spoon and feed himself finger foods Under usual circumstances, Henry is a “good eater”. His diet consists mainly of homemade soups, fruits, vegetables and stews. For the last 2 days, he has been vomiting and refusing to eat 3. Elimination Henry is not toilet trained; he wears cloth diapers He usually has 1 formed bowel movement per day and 5 heavy, wet diapers For the last 2 days, he has been having 5 liquid, loose stools per day 4. Activity & ExerciseHenry is meeting all developmental milestones appropriately. He started walking at 13 months and is very active. 5. Values & BeliefsHelen and Peter are Old Order Mennonite and believe in God. Their lives are very tied to their Mennonite culture. 6. Coping and StressHelen states that having 3 children under the age of 5 can be very busy and stressful. Henry’s current illness has impacted her ability to spend time with the other children. 7. Sleep & RestHenry usually sleeps 10 hours a night and takes a 1-hour afternoon nap. His usual bedtime is 8 pm. He sleeps in a room with his older siblings. 8. Roles & Relationships Peter works on the family farm. Helen is a stay at home mom with the 3 children. Helen does not drive, and needs to wait for Peter to drive her or the children to any appointments. 9. Cognitive/PerceptualHelen states that Henry recognizes and repeats a few words and can obey simple commands. His vision, hearing and speech are normal. Physical Assessment1. General Appearance: Sitting on mother's lap resting against her chest Skin pale in colour Feels warm to touch. Weight – 11 kg. (24 lbs); Height – 83 cm (33”) 2. Vital Signs: Temperature 37.5°C (axilla) Heart rate: 120 beats per minute Respiratory rate: 24 breaths per minute Blood pressure 92/56 Skin Warm to touch, pale in colour, pink nail beds, mucous membranes dry and pink, skin turgor poor, no bruises, red rash around anus4. Respiratory: Lungs clear to auscultation, no crackles, no wheezes 5. Cardiac Heart – normal, no murmurs heard Capillary refill 3 seconds, skin pale 6. Abdomen: No masses Not tender to touch Hyperactive bowel sounds 7. Musculoskeletal: Full range of movement in neck without complaints of pain No joint pain 8. Neurological:Irritable and lethargic 9. Genital/Urinary: Normally has 5 wet diapers per day. Has been having loose stools for the last 2 days. Helen is not sure if he has been voiding along with the loose stools. Patient’s Lab Data for Nurse to Review TestNORMAL Henry’s RESULTSNa136-145 mmol/ L 133 mmol/L K3.4-4 .7 mmol/ L 4.3 mmol/ L CL90-110mmol/L 112 mmol/ L C0220-28 mmol/L 24 mmol/L Blood Urea Nitrogen1.8-6.4 mmol/L6.8 mmol/L CREATININE18-62 mcmol/L 65 mmol/ L Stool for Culture and Sensitivity (C&S)Normal Intestinal FloraStool for Ova and Parasites (O&P)Normal Intestinal Flora 1. Understand the complexities of fluid and electrolyte imbalances in children http://ovidsp.tx.ovid.com.libaccess.lib.mcmaster.ca/sp-3.18.0b/ovidweb.cgi?WebLinkFrameset=1&S=BLCKF... - Changes in fluid and electrolyte balance may happen quickly in infants and children (I & Y C, increasing the nurses responsibility to anticipate often discreet signs of an imbalance - Children and infants present unique problems in managing fluids and electrolytes. Differences in the rate of metabolism and body surface area are two unique aspects - a Childs body composition and homeostatic controls differ from those of an adults the younger the child the greater the differences - Fluid and electrolyte imbalances occur more quickly in children - a newborn’s body is 70-80% water and an adults body is approx. 60% - By the time a child is almost 3 yrs old, the total body water is approx. 60% - Although infants have more fluid in their bodies, they are more susceptible to fluid loss problems because they intake and output more water volume daily than do adults - Insensible water loss (fluids lost through the skin and lungs) are higher for infants and children than for adults. - Any situation that causes an increase in loss of water and electrolytes through he skin threatens the body fluid balance of the infant and small child to a greater degree than it would an older adult - Basal metabolic rate (BMR) for children than it is for adults. An infants high BMR means the fluid intake per Kg body weight per day actually must exceed the per kilogram fluid requirements of an adult. - Infant kidneys are not mature enough to concentrate urine efficiently. The infant needs more water to excrete a given amount of solute. Assessment - As fluid volume decreases extremities become cool, even if the child is febrile - Assess fluid deficit in the mouth - If the pulse rate is greater than 160 beats per min for infants and 120 for children, hypervolemia should be suspected. - Children often hyperventilate to compensate for acidosis - BP is the last vital sign to show changes and not be relied on as an assessment indicator of dehydration - Fontanels of infants will be depressed with a moderate fluid deficit. Dehydration - In children, dehydration is usually attributable to vomiting or an acute viral or bacterial diarrhea 2. Explore health care values from a transcultural perspective Sunrise Model: See the diagram at the bottom of the page. I wasn't able to paste it here.CNO Culturally Sensitive Care Practice guideline Culture- Refers to the learned values, beliefs, norms, and way of life that influence an individuals thinking, decisions and actions in certain ways. · Client centered care requires that nurses recognize the clients culture, the nurses culture and how both affect the nurse client relationship. · There is no single “RIGHT” way to do this for everyone, each client and situation is unique and therefore needs to be assessed and planned for individually · The focus must always be on the clients needs Assumptions · Everyone has a culture · Culture is individual · Individual culture is influenced by many factors (See Figure Sunrise Model) · Culture is always changing · Reactions to other cultures can be automatic, subconscious and have an impact on the nurse client relationship · A nurses own culture is influenced by personal beliefs in addition to our nursing values · We are responsible for assessing and responding appropriately to the clients cultural expectations and needs Acquiring cultural knowledge · It is impossible for nurses to know the details of every culture · It is however, possible for nurses to have a broad understanding of how culture can affect beliefs and behaviours · In health care culture may affect beliefs and values regarding o Perception of health illness and death o Meaning and role of suffering o View of hospitals, nurses, doctors and other healers o Rituals and customs (religious and other) o Boundaries related to privacy, age, gender, and relationships o Effectiveness and values of different types of therapies o Individual time keeping beliefs and practices that may direct activities o Family and social relationships o Decision making on consent to treatment o Independence/self care versus interdependence/being cared for o Communication norms (eye contact) Facilitating client choice · Nurse role is to help client meet their specific health goals. · We need to investigate into the clients view and try to understand the meaning behind a particular request, in addition to their overall treatment goals · If it becomes apparent that a clients cultural preference will negatively affect the client, the nurse works with the client to explain the harm/risks associated with that choice · Likewise, if the preference will affect the wellbeing of other clients, the nurse must look for some ways of achieving some parts of the clients preference, while safeguarding the other clients. Assessment Ask open-ended questions to find out relevant cultural information, nurse needs to listen with respect and remain nonjudgmental 1. What do you think has caused your problems? 2. Why do you think the problem started when it did? 3. What do you think the sickness does to you? 4. What are the major problems the sickness has caused? 5. What have you done for the illness until now? 6. What kind of treatment do you think you should receive? 7. Is there anything else that could be done either by you or by others (family priest) 8. What are the most important results you hope to achieve form these treatments? 9. What do you fear most about your sickness? 10. What do you fear most about the treatment? 11. Who should be consulted or involved in your care? http://www.cno.org/globalassets/docs/prac/41040_culturallysens.pdf Leininger, M. M. (1988). Leininger’s theory of nursing: cultural care diversity and universality. Nursing Science Quarterly, 1 (4), pp. 154-160.
{kind=link}
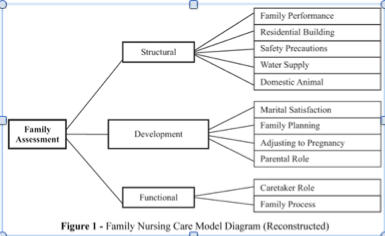
Mennonite Culture · In Ontario often difficult to distinguish Mennonites from others · Old Order – easier to recognize - Typically live without electricity, card and dress in simple, plain clothing - Men wear plain trousers and jackets with a plain straw hat - Women wear their hair long, covered by a prayer cap and have plain dresses - Sometimes use horse drawn buggies to get around - Often choose to educate the children in schools run by themselves ensuring their beliefs continue to get passed down each generation · Many don’t accept heath care and education by the government · Founding beliefs – Anabaptists · New order – live like non-Mennonites but religion is a major aspect - Also called Third Way - Try to connect faith to daily actions - Some believe that baptism and church involvement are voluntary - Use some forms of technology – depends on the community · Woolwich Community Health Centre - Non-profit organization - Provides health care, illness prevention and health promotion services - Funded by Ontario Ministry of Health but not through OHIP - Works with groups of people who face barriers to health and accessing health care http://www.thecanadianencyclopedia.ca/en/article/mennonites/ http://www.wchc.on.ca/about_chc.php 3. Identify the impact of a child's illness on individual family members and the family. Apply family theory in caring for children and caregivers Impact of Pediatric Critical Illness and Injury on Families: A Systematic Literature Review Marysia Shudy, Mary Lihinie de Almeida, Susan Ly, Christopher Landon, Stephen Groft, Tammara L. Jenkins, Carol E. Nicholson http://pediatrics.aappublications.org/content/118/Supplement_3/S203#T2 As shown in Table 1, studies using the PSS:PICU indicate that the most severe parental stress is role alteration. This is understood as the sense of helplessness in parents who are accustomed to control in providing safety and advocacy. Those we reviewed concluded that the main sources of stress in siblings were changes in parental behavior and care by a substitute caregiver Needs: Contact with child; nearby resting place, Know what is wrong with child; informed of changes, Feeling of hope; assurance of best care; maintaining caregiver role Parents felt guilty, excited, discouraged, and exhausted during hospitalization; siblings felt isolated, unimportant, and resentful Parents of children with LT illnesses were given more emotional support than those with NLT illnesses Family dynamics were negatively affected; siblings exhibited increased fears and withdrawal from injured child Family unit experienced increased stress, social distress, and adverse psychological effects In some instances, a major illness brings a family closer together; in others, even a minor illness causes significant strain. 4. Utilize the a family assessment tool to guide interviewing Henry’s mother in a role playing situation - CALGARY Assessment tool Calgary Assessment model (diagram pasted at the bottom of the page showing the flow chart) Wright, L. M., & Leahey, M. (2009). Nurses and families: A guide to family assessment and intervention (5th ed., p. 5). Philadelphia, PA: F. A. Davis Company. and Potter, Patricia, Anne Perry, Janet Ross-Kerr, Marilynn Wood, Barbara Astle, Wendy Duggleby. Canadian Fundamentals of Nursing, 5th Edition. Mosby Canada, 2014. VitalBook file. Be selective in which subcategories to use as it could be overwhelming to the family Structural Assessment • Internal structure is who is included in the family /how they are related to one another · ie. gender roles, sexual orientation, family composition, ranking (number of children, their ages, their expectations based on age) · Questions to ask: o Who is in your family? o Does anyone else live with you: for example, grandparents, boarders? o Has anyone recently moved out of your household, married, or died? o Can you think of anyone else who is like a family member but is not biologically related? o How have your parents' ideas about masculinity and femininity affected your own? Have your ideas about gender been challenged in any way since you became parents? o Do you have expectations of your children on the basis of their gender? o Is the division of labour at home based on gender roles? o How many children are in your family? o What are the children's ages? o Do you have distinct expectations for the oldest and younger children? • External structure is relationships the family shares with people and institutions outside of the family unit · ie. extended family · Context is the whole situation/background relevant to the family · ie. religion, socioeconomic class, ethinicity · Questions to ask: o Where do your parents live? How often do you have contact with them and your siblings? o Which family members do you see or speak with regularly? Who in your extended family are you the closest to? o Have members of your extended family been helpful to you during this time of illness? In what way? o What is your job? How many hours a week do you work? How does this affect family life? o Does anyone in the family work shifts? How does that influence your family functioning? o What level of education have you completed? o Does your family have economic challenges at this time? Developmental Assessment • Stages that families go through that requires adjustment or change • Interaction between individual’s development and the phase of the family developmental life cycle that are important to family functioning • Cycles: Leave home, become young adults, families join together through marriage, families have young children, then families have adolescents, move on to mid life, families in late middle age, and families at end of life Functional Assessment • Divided into instrumental and expressive • It's how family members interact with each other • Instrumental Functioning · Normal ADL's · ie. meals, sleep schedules, attending health needs o How these roles change when coping with relative’s illness or disability o Who is usually responsible for housekeeping and child care? o Do other family members help with these tasks? o Does anyone in the family require help with activities of daily living? o Who will be primarily responsible for flushing Mary's broviac line (an intravenous access device for the administration of medications and blood tests) when she is discharged home? • Expressive Functioning · How people communicate · Emotional: feelings expressed by the family · Verbal: focusing on using words · Nonverbal: body language, gestures, crying · Circular: how each family member influences the behaviour of others o How can you tell when each member of your family is happy, sad, or under stress? o How do you express happiness, sadness, or stress? o Johnny, when you are sad or worried, who in the family do you most like to spend time with or talk to about that? I've embeded the youtube video at the bottom of this document. 5. Mennonite Culture · In Ontario often difficult to distinguish Mennonites from others · Old Order – easier to recognize - Typically live without electricity, card and dress in simple, plain clothing - Men wear plain trousers and jackets with a plain straw hat - Women wear their hair long, covered by a prayer cap and have plain dresses - Sometimes use horse drawn buggies to get around - Often choose to educate the children in schools run by themselves ensuring their beliefs continue to get passed down each generation · Many don’t accept heath care and education by the government · Founding beliefs – Anabaptists · New order – live like non-Mennonites but religion is a major aspect - Also called Third Way - Try to connect faith to daily actions - Some believe that baptism and church involvement are voluntary - Use some forms of technology – depends on the community · Woolwich Community Health Centre - Non-profit organization - Provides health care, illness prevention and health promotion services - Funded by Ontario Ministry of Health but not through OHIP - Works with groups of people who face barriers to health and accessing health care http://www.thecanadianencyclopedia.ca/en/article/mennonites/ http://www.wchc.on.ca/about_chc.php
{kind=link}
Readings for scenario “No more tears for Henry” King, C.K., Glass, R., Bresee, J.S., & Duggan, C. (2003). Managing acute gastroenteritis among children: Oral rehydration, maintenance, and nutritional therapy. MMWR: Morbidity & Mortality Weekly Report, 52(RR-16), 1-16. Retrieved from http://www.cdc.gov/mmwr/index.html Summary Acute Gastroenteritis: - Common illness among infants and children in the world - accounting for >1.5 million outpatient visits, 200,000 hospitalizations, and approximately 300 deaths/year - Diarrhea is one of the common causes of mortality for children < 5 y o - Oral Rehydration Therapy (ORT) o Improved health outcomes among children in developing countries – decreased mortality o Use has lagged in US - Physicians recognize: o Supplementation of zinc can reduce incidence and severity of diarrheal disease o ORS of reduced osmolality (proportional reduced sodium nad glucose): recommended for global use - This article updates recommendations of managing gastroenteritis Introduction & Background - ORT encompasses two phases of treatment: 1) a rehydration phase, in which water and electrolytes are administered as oral rehydration solution (ORS) to replace existing losses, and 2) a maintenance phase, which includes both replacement of ongoing fluid and electrolyte losses and adequate dietary intake - The lag of ORT use in US is thought to be due to the ingrained use of IV therapy and reduced appeal of a technologically simple solution o Many children with mild dehydration and vomiting have ORT withheld - ORT use began in developing countries where IV availability is reduced - NOW, ORT accepted as standard of care for the clinically efficacious and cost-effective management of acute gastroenteritis Physiologic Basis for using ORS - The adult intestinal epithelium must handle 6,500 mL of fluids/day, consisting of a combination of oral intake, salivary, gastric, pancreatic, biliary, and upper intestinal secretions. This volume is typically reduced to 1,500 mL by the distal ileum and is further reduced in the colon to a stool output of <250 mL/day in adults --- during diarrhea the volume of intestinal fluid output is substantially increased overwhelming the reabsorptive capacity of the GI tract - Solutions with a high concentration of co-transporters increase the risk from hypertonic solutions that decrease rather than improve sodium and water transport into the bloodstream. However, solutions of lower osmolarity, but that maintain the 1:1 glucose to sodium ratio, perform optimally as oral solutions for diarrhea management (see Choice of ORS). Home Management of Acute Diarrhea Initiation of Therapy: - All families should be encouraged to have a supply of ORS in the home at all times and to start therapy with a commercially available ORS product as soon as diarrhea begin Need to recognize severity: - Infants are more at risk for becoming dehydrated because of higher body-surface-to-volume ratio, higher metabolic rate, smaller fluid reserves and depend on others for fluid - When fever is present: infants and children should be evaluated to rule out other serious illnesses (sepsis and meningitis) - Box 1 provides a guide for when to seek medical evaluation: Referral for Evaluation: - This is the responsibility of the physician - Focus on factors putting a child at risk of dehydration o Number of days the child has been ill o # of episodes of diarrhea or vomiting o Volume of fluid output o Mental status o Past medical history Clinical Assessment - Diarrhea is 3 or more loose/ watery stools/day o Volume of fluid lost through stools can vary from 5mL/kg body weight/day (normal) à >200 mL/ kg body weight/ day - Dehydration and electrolyte losses associated with untreated diarrhea cause the primary morbidity of acute gastroenteritis. - Diarrhea can be among the initial signs of non-gastrointestinal tract illnesses, including meningitis, bacterial sepsis, pneumonia, otitis media, and urinary tract infection. - Vomiting alone can be the first symptom of metabolic disorders, congestive heart failure, toxic agent ingestion, or trauma. - To rule out other serious illnesses, a detailed history and physical examination should be performed as part of the evaluation of all children with acute gastroenteritis. History: - onset, frequency, quantity, and character (i.e., the presence of bile, blood, or mucus) of vomiting and diarrhea - Recent oral intake, including breast milk and other fluids and food; urine output; weight before illness; and associated symptoms, including fever or changes in mental status, should be noted. - The past medical history should identify underlying medical problems, history of other recent infections, medications, and human immunodeficiency virus (HIV) status. A relevant social history can include the number and nature of caregivers, which can affect instructions regarding follow-up care. Physical Examination Things to gather: - Body weight - Vitals: T, HR, RR, BP - special concern given to infants and children who appear listless, apathetic, or less reactive - sunken eyes? Tearing? - lips, mouth, and tongue will yield critical clues regarding the degree of dehydration - Deep respiration can be indicative of metabolic acidosis - Faint or absent bowel sounds can indicate hypokalemia - general perfusion and capillary refill - check skin turgor Dehydration Assessment This table provides a guideline for a starting point for treatment and who can be sent home for therapy Lab Evaluation - stool cultures should be gathered in there is dysentery but not for acute, watery diarrhes for immunocompetent pt - CBC and urine and blood cultures might be indicated when sepsis or UTIs are a concern Acute Gastroenteritis Therapy based on degree of dehydration - 7 principles guide optimal treatment in Box 2 - Treatment should include two phases: rehydration and maintenance. - Rehydration phase: the fluid deficit is replaced quickly (i.e., during 3--4 hours) and clinical hydration is attained. - Maintenance phase: maintenance calories and fluids are administered. Rapid realimentation should follow rapid rehydration, with a goal of quickly returning the patient to an age-appropriate unrestricted diet, including solids - Breastfeeding should be continued at all times - Diet: increased as soon as tolerated to compensate for lost caloric intake during the acute illness. o Lactose restriction is usually not necessary (although it might be helpful in cases of diarrhea among malnourished children or among children with a severe enteropathy), and changes in formula usually are unnecessary - During both phases, fluid losses from vomiting and diarrhea are replaced in an ongoing manner - Antidiarrheal medications are not recommended for infants and children Minimal Dehydration - treatment is aimed at providing adequate fluids and continuing an age-appropriate diet - use of ORS should be encouraged: 1 mL of fluid should be administered for each gram of output - In hospital: weigh soiled diapers (without urine) - If unable to measure: children weighing <10 kg should be administered 60--120 mL (2--4 ounces) ORS for each episode of vomiting or diarrheal stool, and those weighing >10 kg should be administered 120--240 mL (4--8 ounces) Mild – Moderate Dehydration - should have their estimated fluid deficit rapidly replaced - administering 50--100 mL of ORS/kg body weight during 2--4 hours using additional ORS to replace continued losses - Using a teaspoon, syringe, or medicine dropper, limited volumes of fluid (e.g., 5 mL or 1 teaspoon) should be offered at first, with the amount gradually increased as tolerated - Nasogastric (NG) feeding allows continuous administration of ORS at a slow, steady rate for patients with persistent vomiting or oral ulcers o More cost-effective and well-tolerated than IV rehydration - If ORT doesn’t improve child’s dehydration keep them until signs of dehydration subside - After dehydration is corrected, further management can be implemented at home, provided that the child's caregivers demonstrate comprehension of home rehydration techniques (including continued feeding) Severe Dehydration - constitutes a medical emergency requiring immediate IV rehydration - LR, NS/ similar solution administered until pulse, perfusion and mental status return to normal - Serum electrolytes, bicarbonate, blood urea nitrogen, creatinine, and serum glucose levels should be obtained - Hypotonic solutions should not be used for acute parenteral rehydration - Watch for overhydration - Hydration status should be reassessed frequently to determine the adequacy of replacement therapy - As soon as the severely dehydrated patient's level of consciousness returns to normal, therapy usually can be changed to the oral route, with the patient taking by mouth the remaining estimated deficit. An NG tube can be helpful for patients with normal mental status but who are too weak to drink adequately. Clinical management in the hospital Inpatient care is indicated for children if caregivers cannot provide adequate care at home; substantial difficulties exist in administrating ORT, including intractable vomiting, ORS refusal, or inadequate ORS intake; concern exists for other possible illnesses complicating the clinical course; ORS treatment fails, including worsening diarrhea or dehydration despite adequate volumes; severe dehydration (>9% of body weight) exists; social or logistical concerns exist that might prevent return evaluation, if necessary, or such factors as young age, unusual irritability or drowsiness, progressive course of symptoms, or uncertainty of diagnosis exist that might indicate a need for close observation. Limitations of ORT: - children in hemodynamic shock – their airway protective reflexes might be impaired - Ab ileus: don’t give fluids until BS are audible - Bowel obstruction - A limited percentage of infants (<1%) with acute diarrhea experience carbohydrate malabsorption. This is characterized by a dramatic increase in stool output after intake of fluids containing simple sugars (e.g., glucose), including ORS Hypernatremic Dehydration - serum sodium concentration >145 mEq/L - Respond well to ORT Dietary Therapy - Breastfed infants: feed on demand - Formula-fed infants should continue their usual formula immediately upon rehydration in amounts sufficient to satisfy energy and nutrient requirements - Not necessary to use lactose free formulas (unless lactose intolerant) - Children receiving semisolid or solid foods should continue to receive their usual diet during episodes of diarrhea. Foods high in simple sugars should be avoided because the osmotic load might worsen diarrhea; therefore, substantial amounts of carbonated soft drinks, juice, gelatin desserts, and other highly sugared liquids should be avoided. - Early feeding decreases changes in intestinal permeability caused by infection, reduces illness duration, and improves nutritional outcomes - Recommended foods include age-appropriate unrestricted diets, including complex carbohydrates, meats, yogurt, fruits, and vegetables. Pharmacological Therapy Antimicrobial - antimicrobial therapy is not usually indicated among children because the majority of cases of acute diarrhea are self-limited and not shortened by antimicrobial agents. Exceptions to these rules involve special needs of individual children Nonantimicrobial Drug Therapies - Nonspecific antidiarrheal agents (e.g., adsorbents such as kaolin-pectin), antimotility agents (e.g., loperamide), antisecretory drugs, and toxin binders (e.g., cholestyramine), are commonly used among older children and adults, but data are limited regarding their efficacy. Supplemental Zinc Therapy - severe zinc deficiency (e.g., acrodermatitis enteropathica) is associated with diarrhea, milder deficiencies of zinc might play a role in childhood diarrhea, and zinc supplementation might be of benefit either for improved outcomes in acute or chronic diarrhea or as prophylaxis against diarrheal disease - # of trials have been shown that zinc supplements help in treating diarrheal disease but this needs further evaluation Probiotics - Further human trials are needed before making specific recommendations Acute Bloody Diarrhea (Dysentery) - Oral rehydration therapy is critical in managing specific types of diarrheal diseases. - Dysentery: acute bloody diarrhea caused by invasive microbial infection. o Doesn’t include occult blood (detected by guaiac card only) or streaks of blood on the surface of formed stool - Tx of dehydration in dysentery follows the same principles as treatment of acute watery diarrhea. - Child with bloody diarrhea is at higher risk for complications, including sepsis and other systemic diseases - threshold for admission of such children to the hospital for close observation is lower. - Stool cultures are needed for guiding therapy. Food should not be withheld for children with dysentery any more than in other cases of diarrhea. More frequent, smaller meals might be better tolerated, and higher protein intakes - In the majority of cases, empiric antimicrobial agents should not be administered while awaiting culture results, because antimicrobial therapy might not be indicated even when culture results are positive. Amoebiasis is an unusual cause of bloody diarrhea in young children, even in less-developed countries. Treatment for amoebiasis should be reserved for those cases in which trophozoites are detected on microscopic examination of the stools Choice of ORS: - In 1975, WHO and the United Nations Children's Fund (UNICEF) agreed to promote a single ORS (WHO-ORS) containing (in mmol/L) sodium 90, potassium 20, chloride 80, base 30, and glucose 111 (2%) for use among diverse populations – single solution to be used for diarrhea treatment with a variety of electrolytes losses - Further studies have shown ORS of lower osmolality is better than ORT Barriers - Cultural practices - Lack of parental knowledge - Lack of training for HCP - Cost - Among physicians, preference for IV hydration, even where evidence indicates improved results from oral rehydration = major barrier Conclusion: Treatment of acute diarrhea has relied upon simple and effective therapy of oral rehydration. The critical co-principle in case management of early resumption of feeding of children immediately upon rehydration has also gained wide acceptance. More recent advances in the science of diarrhea treatment include recognition for the role of zinc supplementation in reducing disease severity and occurrence, and development of an oral rehydration solution of lower osmolarity for global use. The combination of oral rehydration and early nutritional support promises to safely and effectively assist a patient through an episode of diarrhea. If the principles of therapy outlined in this report are accepted by all levels of the medical community and if education of parents includes teaching them to begin ORT at home, numerous deaths and unnecessary clinic visits and hospitalizations can be avoided. ORT is suitable for use among children throughout the world Toddlers (18months – 3 yrs old) Important stages of growth, development and maturation: Physical - Growth is slower - Growth in spurts - Wide gait and walk hesitantly - Fine and gross motor skills progress quickly - Fine Motor skills: reaching, grasping, manipulating small objects - Gross Motor skills: balance and coordination continuously improve, most are walking alone by 18months, tend to experiment with skills Cognitive - Relationships between objects and actions - Imitate adults - Develop a number sense, match colours and shapes - Engage in symbolic play (object-use and make-believe) Social/ Emotional - Egocentric - Autonomous and independent - No conscience - Demonstrate negativism - Enjoy ritualism - Experience separation anxieties - Tantrums as coping mechanism - Early toddlers: solitary play - Early preschoolers: associative play Common Concerns/Hazards - Illnesses: chickenpox, viruses - Hazards: most deaths are a result of accidents (from their curiosity): falls, chemicals, burns, drowning, choking, and MVA Communication Techniques: - Demonstrate and use play to teach a procedure - Provide visuals - Simplify vocabulary: clear and firm instructions - Offer limited options: don’t offer a choice when there is none - Praise a child for a job well done
Want to create your own Notes for free with GoConqr? Learn more.