20048059
Descripción
Test por Kaylee Garrick, actualizado hace más de 1 año
|
|
Creado por Kaylee Garrick
hace alrededor de 5 años
|
|
Pregunta 1
Pregunta
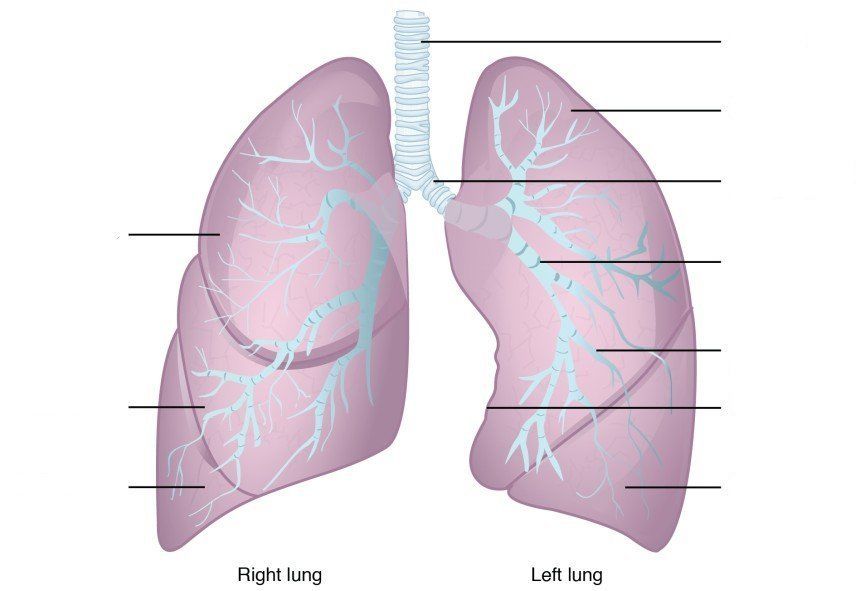
Label the areas of the respiratory CONDUCTING zones as appropriate:
Image:
Lung (binary/octet-stream)
{kind=link}
Respuesta
-
Trachea
-
Superior Lobe
-
Main (primary) bronchus
-
Lobar (secondary) bronchus
-
Segmental (tertiary) bronchus
-
Cardiac notch
-
Inferior lobe
-
Middle lobe
-
Trachea
-
Superior lobe
-
Main (primary) bronchus
-
Lobar (secondary) bronchus
-
Segmental (tertiary) bronchus
-
Cardiac notch
-
Inferior lobe
-
Middle lobe
-
Trachea
-
Superior lobe
-
Main (primary) bronchus
-
Lobar (secondary) bronchus
-
Segmental (tertiary) bronchus
-
Cardiac notch
-
Inferior lobe
-
Middle lobe
-
Trachea
-
Superior lobe
-
Main (primary) bronchus
-
Lobar (secondary) bronchus
-
Segmental (tertiary) bronchus
-
Cardiac notch
-
Inferior lobe
-
Middle lobe
-
Trachea
-
Superior lobe
-
Main (primary) bronchus
-
Lobar (secondary) bronchus
-
Segmental (tertiary) bronchus
-
Cardiac notch
-
Inferior lobe
-
Middle lobe
-
Trachea
-
Superior lobe
-
Main (primary) bronchus
-
Lobar (secondary) bronchus
-
Segmental (tertiary) bronchus
-
Cardiac notch
-
Inferior lobe
-
Middle lobe
-
Trachea
-
Superior lobe
-
Main (primary) bronchus
-
Lobar (secondary) bronchus
-
Segmental (tertiary) bronchus
-
Cardiac notch
-
Inferior lobe
-
Middle lobe
-
Trachea
-
Superior lobe
-
Main (primary) bronchus
-
Lobar (secondary) bronchus
-
Segmental (tertiary) bronchus
-
Cardiac notch
-
Inferior lobe
-
Middle lobe
-
Trachea
-
Superior lobe
-
Main (primary) bronchus
-
Lobar (secondary) bronchus
-
Segmental (tertiary) bronchus
-
Cardiac notch
-
Inferior lobe
-
Middle lobe
-
Trachea
-
Superior lobe
-
Main (primary) bronchus
-
Lobar (secondary) bronchus
-
Segmantal (tertiary) bronchus
-
Cardiac notch
-
Inferior lobe
-
Middle lobe
Pregunta 2
Pregunta
The passage of air into the lungs is governed by pressure differences caused by changes in [blank_start]lung volume[blank_end]. The [blank_start]thoracic diaphragm[blank_end] is the principle muscle of respiration which is innervated by the phrenic nerves derived from the ventral rami of cervical segments 3 – 5.
Respuesta
-
lung volume
-
lung capacity
-
lung residue
-
lung resilience
-
thoracic diaphragm
-
lumbar diaphram
-
cervical diaphram
-
adregeneric diaphragm
Pregunta 3
Pregunta
When the diaphragm [blank_start]contracts[blank_end], the vertical diameter of the thoracic cavity increases and air moves into the lungs. This relationship between volume and pressure is represented in [blank_start]Boyle’s Law[blank_end]
Respuesta
-
contracts
-
relaxes
-
inverts
-
Boyle’s Law
-
Charles' Law
-
Henry's Law
-
Starling's Law
Pregunta 4
Pregunta
[blank_start]Muscles of inspiration[blank_end]: external intercostals, sternocleidomasoids, scalei, anterior serrate, trapezius, posterior neck muscles.
[blank_start]Muscles of expiration[blank_end]: internal intercostals, posterior inferior serrate, abdominal muscles.
[blank_start]Normal conditions[blank_end]: diaphragm and intercostals
Respuesta
-
Muscles of inspiration
-
Muscles of expiration
-
Normal conditions
-
Muscles of expiration
-
Muscles of inspiration
-
Normal conditions
-
Normal conditions
-
Muscles of inspiration
-
Muscles of expiration
Pregunta 5
Pregunta
In a patient with a pneumothorax, the lung collapses when the [blank_start]intraplural space[blank_end] is violated and the [blank_start]negative[blank_end] pressure between the lung and chest wall is no longer maintained
Respuesta
-
intraplural space
-
extraplural space
-
intercostal space
-
myocardial space
-
negative
-
positive
-
inerrant
-
backforce
Pregunta 6
Pregunta
Patients with Asthma have narrowed air passages due to smooth muscle contraction, mucus plugging and inflammation. This leads to an [blank_start]increase[blank_end] in residual volume, a [blank_start]decrease[blank_end] in vital capacity and a [blank_start]decrease[blank_end] in expiratory reserve volume
Respuesta
-
increase
-
decrease
-
decrease
-
increase
-
decrease
-
increase
Pregunta 7
Pregunta
In patients with emphysema, lung tissue is destroyed and weakened airway walls collapse during [blank_start]expiration[blank_end]. Because of chronic lung tissue inflammation and swelling, the airway walls have decreased recoil and elasticity. Thus, inspiritory capacity and expiratory reserve volume [blank_start]decease[blank_end] while reserve volume [blank_start]increases[blank_end]
Respuesta
-
expiration
-
inspiration
-
decease
-
increase
-
increases
-
decreases
-
remains the same
Pregunta 8
Pregunta
According to [blank_start]La Place’s[blank_end] Law, the surface tension of smaller alveoli is [blank_start]greater[blank_end] than that of larger alveoli. [blank_start]Surfactant[blank_end] is a substance produced by type II alveolar cells which decreases surface tension of the alveoli and is an important component to think about when dealing with [blank_start]pre-mature babies[blank_end]
Respuesta
-
La Place’s
-
Boyle's
-
Charles'
-
Henry's
-
Starling's
-
greater
-
lesser
-
the same
-
Surfactant
-
Lubriol
-
Protasine
-
Pluratol
-
pre-mature babies
-
obese patients
-
geriatrics
-
teenagers
Pregunta 9
Pregunta
Damage to the capillary membrane, heart failure and valvular disease can all lead to [blank_start]pulmonary odeama[blank_end]. This is due to an imbalance in the normal forces at the alveolar capillary membrane, causing fluid to accumulate in the pulmonary interstitial space and alveoli. This is best illustrated by [blank_start]Starling’s Law[blank_end]
Respuesta
-
pulmonary odeama
-
Emphysema
-
Asthma
-
Bronchitis
-
Starling’s Law
-
Henry's Law
-
Charles's Law
-
La Place's Law
Pregunta 10
Pregunta
Excess fluid accumulating within the pulmonary interstitial space is usually taken up by the [blank_start]lymphatic system[blank_end]
Respuesta
-
lymphatic system
-
artieral system
-
pulmonary system
-
endocrine system
Pregunta 11
Pregunta
Airway diameter and secretions are primarily controlled by the [blank_start]autonomic nervous system[blank_end]. [blank_start]Beta-2[blank_end] receptors function to dilate the bronchioles when activated by adrenergic agonists such as epinephrine and norepinephrine. Stimulation of these receptors also [blank_start]decreases[blank_end] the secretions of mucus and serous glands
Respuesta
-
autonomic nervous system
-
cardiac receptor system
-
somatic nervous system
-
enteric system
-
Beta-2
-
Beta-1
-
Alfa-1
-
Alfa-2
-
decreases
-
increases
Pregunta 12
Pregunta
[blank_start]Inspiration[blank_end] is controlled neurologically via the medullary respiratory centre which sends signals via the phrenic nerve. [blank_start]Expiration[blank_end] is controlled via the ventral respiratory group and is usually only activated during exercise or with certain diseases (COPD) where where [blank_start]expiration[blank_end] becomes an active process.
Respuesta
-
Inspiration
-
Expiration
-
Respiratory syncope
-
Expiration
-
Inspiration
-
Respiratory syncope
-
expiration
-
inspiration
-
respiratory syncope
Pregunta 13
Pregunta
Chemoreceptors play an important role in the regulation of respiration. Central chemoreceptors in the [blank_start]medulla[blank_end] are sensitive to PH of cerebrospinal fluid. When the PH level drops, the ventilary rate [blank_start]increases[blank_end]. This would be due to an [blank_start]increase[blank_end] in C02 levels
Respuesta
-
medulla
-
aorta
-
cerebellum
-
cerebrum
-
increases
-
decreases
-
increase
-
decrease
Pregunta 14
Pregunta
Why would a hyperventilating patient lose consciousness?
Respuesta
-
PH levels will fall, causing central chemoreceptors to reduce the ventilary rate
-
PH levels will rise, causing central chemoreceptors to reduce the ventillary rate
-
PH levels will fall, causing central chemoreceptors to increase the ventillary rate
-
PH levels will rise, causing the central chemoreceptors to increase ventilary rate
Pregunta 15
Pregunta
Peripheral chemoreceptors exist in the [blank_start]carotid and aortic bodies[blank_end]. These are sensitive to [blank_start]oxygen[blank_end] and hence, if levels fall to a very low rate (below 60 mmHg), these are activated to increase ventillary rate. Those who have this system consistently activated are said to have a [blank_start]hypoxic drive[blank_end]
Respuesta
-
carotid and aortic bodies
-
medulla
-
recticular respiratory zone
-
pluralistic bodies
-
oxygen
-
carbon dioxide
-
hydrogen ions
-
bicarbonate
-
hypoxic drive
-
asthmatic tendancy
-
ventilation to perfusion mismatch
-
tachypnoeic altercation
Pregunta 16
Pregunta
Albuteral, bitolterol and salmeterol are all examples of [blank_start]Beta-2 Agonists[blank_end], used for treating Asthma and COPD. These work by inducing [blank_start]relaxation[blank_end] of the bronchial musculature. However, they can also have an effect on Beta-1 receptors causing [blank_start]increased heart rate[blank_end]
Respuesta
-
Beta-2 Agonists
-
anticholinergic agents
-
Glucocorticoids
-
Afla-1 Agonists
-
relaxation
-
constriction
-
spasm
-
exitation
-
increased heart rate
-
reduced heart rate
-
Atrial fibrillation
-
Atrial flutter
Pregunta 17
Pregunta
Ipratopium bromide works to reverse overstimulation of the autonomic nervous system by blocking the [blank_start]parasympathetic[blank_end] neurotransmitters. They are hence known as [blank_start]anticholinergic agents[blank_end]
Respuesta
-
parasympathetic
-
sympathetic
-
anticholinergic agents
-
Beta-2 agonists
-
glucocorticoids
-
Beta blockers
Pregunta 18
Pregunta
Glucocorticoids also reffered to as corticosteroids are compounds synthesized from the [blank_start]zona recticulars fasciculars[blank_end] of the adrenal cortex. [blank_start]Methylprednisolone[blank_end] is an example of this steroid
Respuesta
-
zona recticulars fasciculars
-
zona glomerulosa
-
zona medullla
-
Methylprednisolone
-
ibatropium
-
albuterol
-
salbutamol
Pregunta 19
Pregunta
Your unit is called to the scene of a 33-year old asthmatic complaining of severe shortness of breath. Lung sounds are decreased with diffuse wheezing and a prolonged expiratory component. All of the following are muscles of expiration, EXCEPT:
Respuesta
-
Internal instercostals
-
Prosterior inferior serrate
-
Rectus abdominous
-
Sternocleidomastoids
-
External Obliques
Pregunta 20
Pregunta
What would pulmonary function testing be likely to show in a patient experiencing a severe asthma attack?
Respuesta
-
Increased residual volume
-
Increased expiratory reserve volume
-
Increased vital capacity
-
Decreased inspiritory capacity
-
Little change in lung capacity
Pregunta 21
Pregunta
Patients with COPD are expected to have which of the following?
Respuesta
-
Difficulty with inspiring air due to bronchial narrowing
-
A decreased residual volume due to air trapped in dilated alveoli
-
Increased inspiratory capacity and decreased expiratory reserve volume
-
Increased elastic recoil of the lung segments
-
Difficulty with expiration due to chronic lung tissue inflammation and swelling
Pregunta 22
Pregunta
Neonatal respiratory distress syndrome occurs in certain infants as a result of:
Respuesta
-
Chronic airways inflammation
-
Hypertrophy of type II alveolar cells
-
Hyperactivity of type I alveolar cells
-
Collapse of the alveoli during expiration due to a lack of surfactant
-
Bronchoconstriction due to hyperresponsiveness to supplemental oxygen
Pregunta 23
Pregunta
The mechanism of beta-2 agonists in asthma is:
Respuesta
-
Activation of the parasympathetic neurons to provide bronchodilation
-
Stimulation to increase the secreations of the mucous glands to rid the lungs of irritants
-
Stimulation of beta-2 adrenergic receptors on cells in the terminal bronchioles
-
Stimulation of beta-2 adrenergic receptors on cells in the proximal bronchi
-
Disinhibation of the medullary respiratory centre located in the brainstem
Pregunta 24
Pregunta
A patient is hyperventilating and loses consciousness – what is the pathologic mechanism responsible for this?
Respuesta
-
Increased carbon dioxide levels in the CSF
-
Decreased carbon dioxide and hydrogen concentrations in the CSF
-
Increased oxygen levels in the CSF
-
Inhibition of the central chemoreceptors in the medulla
-
Activation of the carotid bodies in response to decreased inhaled carbon dioxide
Pregunta 25
Pregunta
A 69-year old with emphysema becomes less responsive with decreased respirations while on 4 lpm of oxygen during a prolonged inter-facility transport. What is the likely mechanism for these findings?
Respuesta
-
Lowering of the P02 to very low levels causing a hypoxic drive, stimulated by peripheral chemoreceptors in the carotid bodies – now being suppressed by the prolonged administration of oxygen
-
Lowing of the P02 to very low levels causing suppression of the hypoxic drive, stimulated by peripheral chemoreceptors in the carotid bodies
-
Build-up of C02 and hydrogen ions in the CSF, causing activation of the central chemoreceptors which will suppress ventilations
-
Lowering of the P02 to very low levels causing suppression of the hypoxic drive, stimulated by the central chemoreceptors of the medulla
-
Lowering of the PC02 to very low levels causing suppression of the hypoxic drive, stimulated by the central chemoreceptors of the medulla
Pregunta 26
Pregunta
The National Heart, Lung and Blood institute defines asthma as a [blank_start]chronic inflammatory disorder[blank_end] of the airways
Respuesta
-
chronic inflammatory disorder
-
acute respiratory implication
-
rare pathological damage
-
pulmonary odemic complication
Pregunta 27
Pregunta
[blank_start]Extrinsic[blank_end] asthma is believed to be caused by an antibody-dependant (IgE) activation of cells that release inflammatory mediators. For that reason, it is also known as allergic asthma and is usually picked up in [blank_start]childhood[blank_end]
Respuesta
-
Extrinsic
-
Intrinsic
-
Excretory
-
Excitory
-
childhood
-
adulthood
-
teenagers
-
geriatrics
-
newborns
Pregunta 28
Pregunta
[blank_start]Intrinsic[blank_end] asthma is more common in adults, is not related to antibody activation, tends to be more chronic, is severe and often controlled only with [blank_start]corticosteroids[blank_end]. Triggers include exercise or infections rather than exposure to allergens
Respuesta
-
Intrinsic
-
Extrinsic
-
Intubatory
-
Allergic
-
corticosteroids
-
Beta-2 agonists
-
anticholinergic agents
-
Beta blockers
Pregunta 29
Pregunta
When mast cells are stimulated by IgE antibodies, numerous mediators (i.e. cytokines) are released, contributing to what is known as a generalised state of bronchial hyperresponsiveness. This causes:
Respuesta
-
Smooth muscle constriction in the bronchioles
-
edema
-
increased mucus secretion
-
decreased mucus secretion
-
smooth muscle construction in the trachea
-
smooth muscle dilation in the bronchioles
-
dehydration
Pregunta 30
Pregunta
The [blank_start]late response[blank_end] represents the secondary phase of an asthma episode, typically occurring [blank_start]4-12[blank_end] hours after the initial allergen introduction. This is significant as the cycle primes patients for future episodes by exposing sensitive irritant receptors that can later be more easily activated
Respuesta
-
late response
-
after response
-
by-response
-
recurrent response
-
4-12
-
24
-
1-2
-
6
Pregunta 31
Pregunta
People who have symptom free intervals between episodes are said to have:
Respuesta
-
episodic asthma
-
intrinsic asthma
-
extrinsic asthma
-
adolescent asthma
-
allergic asthma
Pregunta 32
Pregunta
Match these signs with their main symptoms:
Airways narrowing due to smooth muscle contraction / Inflammation of the airways – [blank_start]wheeze[blank_end]
Hyperinflation from trapped air in the distal airways – [blank_start]dyspnoea and tachyponea[blank_end]
Airway narrowing and hypersecretion – [blank_start]cough and chest tightness[blank_end]
A fall of more than 10 mmHg in systolic pressure during inspiration as a consequence of lung hyperinflation which compresses the left ventricle (right ventricular end systolic pressure increases, compressing the intraventricular septum) – [blank_start]pulsus paradoxus[blank_end]
Increased ventilation-perfusion mismatching due to airway obstruction – [blank_start]hypoxaemia[blank_end]
Respuesta
-
wheeze
-
pulsus paradoxus
-
hypoxaemia
-
dyspnoea and tachyponea
-
cough and chest tightness
Pregunta 33
Pregunta
Match the clinical features with the asthma classification:
[blank_start]Mild Intermittent[blank_end] (Step 1) – symptoms <2x/wk, brief exacerbations, PEF >80%
[blank_start]Mild Persistent[blank_end] (Step 2) - symptoms >2x/wk, night symptoms >2x/mo, exacerbations effect activity, PEF >80%
[blank_start]Moderate Persistent[blank_end] (Step 3) – symptoms daily, daily use of albuterol, excaserbations greater than 2x/week, night symptoms >1x/wk, PEF >60 - <80%
[blank_start]Severe Persistant[blank_end] (Step 4) – symptoms continuous, liminted physical activity, frequent night symptoms, PEF ,60%
Respuesta
-
Mild Intermittent
-
Mild Persistent
-
Moderate Persistent
-
Severe Persistant
Pregunta 34
Pregunta
Fill in the blanks:
Step 1 (mild intermittent) : QUICK RELIEF [blank_start]Short acting bronchodilator[blank_end]; LONG TERM CONTROL [blank_start]No daily medication required[blank_end]
Step 2 (mild persistent): QUICK RELIEF [blank_start]Short acting bronchodilator[blank_end] ; LONG TERM CONTROL [blank_start]Low dose inhaled corticosteroid[blank_end] OR [blank_start]Mast Cell Stabiliser[blank_end] OR [blank_start]Leukotrine inhibitor[blank_end]
Step 3 (moderate persistent) : QUICK RELIEF [blank_start]short acting bronchodilator[blank_end]; LONG TERM CONTROL [blank_start]Medium dose inhaled corticosteroid[blank_end] AND [blank_start]long acting bronchodilator[blank_end]
Step 4 (severe persistent): QUICK RELIEF [blank_start]short acting bronchodilator[blank_end] ; LONG TERM CONTROL [blank_start]high dose inhaled corticosteroid[blank_end] AND [blank_start]long acting bronchodilator[blank_end] AND [blank_start]corticosteroid tablets[blank_end]
Respuesta
-
Short acting bronchodilator
-
No daily medication required
-
Low dose inhaled corticosteroid
-
Mast Cell Stabliser
-
Leukotrine inhibitor
-
Long acting bronchodilator
-
No daily medication required
-
Long acting bronchodilator
-
Short acting bronchodilator
-
High dose inhaled corticosteroid
-
Short acting bronchodilator
-
No daily medication required
-
Low dose inhaled corticosteroid
-
mast cell stabilizer
-
long acting bronchodilator
-
Low dose inhaled corticosteroid
-
No daily medications
-
high dose inhaled corticosteroid
-
long acting bronchodilator
-
Mast Cell Stabiliser
-
corticosteroid tablets
-
Leukotrine inhibitor
-
Mast cell activator
-
long acting brocnhodilator
-
short acting bronchodilator
-
no daily tablets
-
mast cell stablisers
-
luekotrine inhibitors
-
Medium dose inhaled corticosteroid
-
Low dose inhaled corticosteroid
-
High dose corticosteroid
-
Mast cell activator
-
long acting bronchodilator
-
short acting bronchodilator
-
corticosteroid tablets
-
Leukotrine inhibitor
-
short acting bronchodilator
-
long acting bronchodilator
-
Mast cell stabilizer
-
No quick relief
-
high dose inhaled corticosteroid
-
medium dose inhaled corticosteroid
-
low dose inhaled corticosteroid
-
Leukotrine inhibitor
-
long acting bronchodilator
-
short acting bronchodilator
-
corticosteroid tablets
-
corticosteroid injections
-
corticosteroid inhibitors
Pregunta 35
Pregunta
Match the drug to the action:
Relaxes smooth muscle while also decreasing the release of mediators from mast cells and basophils –
DRUG TYPE [blank_start]Beta-adrenergic agonist[blank_end] – EXAMPLE [blank_start]albuterol, epinephrine[blank_end]
Inhibitory effect on bronchoconstricting leutrienes and prostaglandins by stopping phospholipid A2 –
DRUG TYPE [blank_start]anti-inflamitory agent (corticosteroids)[blank_end], EXAMPLE [blank_start]prednisolone[blank_end]
Inhibition of the parasympathetic nervous system by selectively binding and blocking the neurotransmitter acetylcholine to its receptor in nerve cells –
DRUG TYPE [blank_start]anticholinergic[blank_end], EXAMPLE [blank_start]Ipatropium[blank_end]
Respuesta
-
Beta-adrenergic agonist
-
albuterol, epinephrine
-
anti-inflamitory agent (corticosteroids)
-
prednisolone
-
anticholinergic
-
Ipatropium
Pregunta 36
Pregunta
Several risk factors for COPD have been identified, but by far the primary cause is related to [blank_start]tobacco smoke exposure[blank_end]
Respuesta
-
tobacco smoke exposure
-
obesity
-
cardiac failure
-
excessive exercise
Pregunta 37
Pregunta
The four main actions of tobacco smoke are:
Respuesta
-
impairs ciliary movement
-
inhibits the function of macrophages
-
overstimulates the mucus glands
-
Stimulates irritant receptors
-
Induces smooth muscle contraction
-
Causes bronchoconstriction
-
inhibits the mucus glands
-
causes vasodilation of the alveoli
-
Reduces irritant receptor sensitivity
Pregunta 38
Pregunta
Someone who is known to be a “pink puffer” will be likely to have what characteristics?
Age: [blank_start]>50[blank_end]
Disease process: [blank_start]Emphysema[blank_end]
Cough: [blank_start]Mild[blank_end]
Weight Changes: [blank_start]weight loss[blank_end]
Sputum: [blank_start]Scant[blank_end]
Degree of hypoxia: [blank_start]Mild[blank_end]
Response to bronchodilators: [blank_start]Mild improvement[blank_end]
Cough type: [blank_start]Dyspneic[blank_end]
Accessory Muscle Use: [blank_start]Yes[blank_end]
Hyperventillation: [blank_start]Yes[blank_end]
Respuesta
-
>50
-
Young (50s)
-
Emphysema
-
Bronchitis
-
Mild
-
Chronic
-
weight loss
-
weight gain
-
Scant
-
Copious
-
Mild
-
Severe
-
Mild improvement
-
Great improvement
-
Dyspneic
-
Tussive
-
Yes
-
No
-
Yes
-
No
Pregunta 39
Pregunta
Someone who is known to be a “blue bloater” will be likely to have what characteristics?
Age: [blank_start]Young (50s)[blank_end]
Disease process: [blank_start]Bronchitis[blank_end]
Cough: [blank_start]Chronic[blank_end]
Weight Changes: [blank_start]weight gain[blank_end]
Sputum: [blank_start]copious[blank_end]
Degree of hypoxia: [blank_start]Can be severe[blank_end]
Response to bronchodilators: [blank_start]great improvement[blank_end]
Cough: [blank_start]Tussive[blank_end]
Accessory muscle use: [blank_start]No[blank_end]
Hyperventilation: [blank_start]No[blank_end]
Respuesta
-
Young (50s)
-
>50
-
Bronchitis
-
Emphysema
-
Chronic
-
Mild
-
weight gain
-
weight loss
-
copious
-
scant
-
Can be severe
-
Mild
-
great improvement
-
mild improvement
-
Tussive
-
Dyspneic
-
No
-
Yes
-
No
-
Yes
Pregunta 40
Pregunta
You are called to a 60 y/o patient who is sat in the tripod position on arrival. Respiratory inspection reveals use of excessory muscles to breathe, mild hypoxia and a mild cough producing little sputum. Pt is found to have a prolonged expiratory component with a wheeze on exhalation. Without any further history taking, what disease process could this patient have?
Respuesta
-
Emphysema
-
Bronchitis
-
Asthma
Pregunta 41
Pregunta
Permanent destruction of elastic segments of the alveoli by mechanical, chemical, or other factors is the pathogenetic hallmark of:
Respuesta
-
Emphysema
-
Bronchitis
-
Asthma
Pregunta 42
Pregunta
You are called to a 49 y/o patient with a chronic cough producing copious amounts of sputum. You notice the patient is overweight and on examination find them to be hypoxic but with only a small, insignificant rise in RR. The patient tells you that his breathing symptoms are part of a chronic condition and this is not acute.
Respuesta
-
Emphysema
-
Bronchitis
-
Asthma
Pregunta 43
Pregunta
Irritation of the mucosa by smoke, chemicals and other irritants leading to the hyperplasia of mucus glands and disruption of the normal function of cilia in the respiratory tissue lining the airways describes:
Respuesta
-
Bronchitis
-
Emphysema
Pregunta 44
Pregunta
What pathologic changes are thought o be responsible for the development of the barrel chest of emphysema?
Respuesta
-
Permanent dilation of the pulmonary air spaces with the destruction of the airway walls
-
Stretching of bronchi with air trapping in the plural space
-
Formation of small air spaces in segments of lung with air leakage into the plura
-
Alveolar expansion during expiration due to increased surfactant formation
-
Increased vital capacity
Pregunta 45
Pregunta
All of the following classes of medications can be used in the acute COPD exacerbations, EXCEPT:
Respuesta
-
Beta-2 adrenergic receptor agonists
-
Systemic corticosteroids
-
Methylated Xanthines
-
Cholinergic agonists
Pregunta 46
Pregunta
While all of these are a risk factor for COPD, which is the most likely to cause it?
Respuesta
-
Previous exposure to sulphur dioxide and nitrogen dioxide
-
History of alfa1-antitrypsin deficiency
-
Exposure to significant air pollution
-
A history of severe viral pneumonia during infancy
-
Tobacco smoke exposure
Pregunta 47
Pregunta
Match the following clinical characteristics to the most appropriate type of COPD patient:
- A 66 y/o woman with dyspnoea, mild hypoxia and a history of weight loss – [blank_start]EMPHYSEMA (pink puffer)[blank_end]
- A 55 y/o morbidly obese smoker with dyspnoea who improves significantly after two treatments of nebulised albuterol – [blank_start]BRONCHITIS (blue bloater)[blank_end]
- A 72 y/o male smoker with accessory muscle use, hyperventilation and a barrel chest – [blank_start]EMPHYSEMA (pink puffer)[blank_end]
- A 50 y/o female with a history of chronic occupational smoke exposure who presents with copious sputum, chronic cough and severe hypoxia – [blank_start]BRONCHITIS (blue bloater)[blank_end]
- An 8 y/o female with a history of wheezing after exposure to a new pet – [blank_start]NEITHER[blank_end]
Respuesta
-
EMPHYSEMA (pink puffer)
-
BRONCHITIS (blue bloater)
-
NEITHER
-
BRONCHITIS (blue bloater)
-
EMPHYSEMA (pink puffer)
-
NEITHER
-
EMPHYSEMA (pink puffer)
-
BRONCHITIS (blue bloater)
-
NEITHER
-
BRONCHITIS (blue bloater)
-
EMPHYSEMA (pink puffer)
-
NEITHER
-
NEITHER
-
BRONCHITIS (blue bloater)
-
EMPHYSEMA (pink puffer)
Pregunta 48
Pregunta
Venostsis; vessel wall inflammation and/or endothelial injury; hypercoagulability all relate to [blank_start]Virchow’s triad[blank_end] for pulmonary embolism.
Respuesta
-
Virchow’s triad
-
Cushing's triad
-
Beck's triad
-
Dieulafoy's triad
Pregunta 49
Pregunta
While all of these are a risk factor for PE, which is the most likely to cause it?
Respuesta
-
Recent surgery
-
Pregnancy
-
Prolonged immobilisation
-
Presence of an underlying malignancy
-
Previous history of a DVT or PE
Pregunta 50
Pregunta
With few exceptions, almost all emboli arise within the large deep veins of the [blank_start]pelvis[blank_end] and [blank_start]lower extremities[blank_end].
Respuesta
-
pelvis
-
humerus
-
sternum
-
ulna
-
ribcage
-
spine
-
lower extremities
-
upper extremities
-
mid auxiliary components
Pregunta 51
Pregunta
Thrombus almost always starts in the veins of the calf (saphenous vein) and propagates to veins above the knee. Over 90% of emboli arise from the following viens (TICK THREE):
Respuesta
-
Femoral
-
Popliteal
-
Illiac
-
Renal
-
Pulmonary
-
Basilic
-
Auxiliary
Pregunta 52
Pregunta
Signs and symptoms of a PE include:
Respuesta
-
Haemoptysis
-
Dyspnoea
-
Pleuritic chest pain
-
Apprehension
-
Tachypnoea
-
Tachycardia
-
Fever
-
Sweating
-
Syncope
-
Cyanosis
Pregunta 53
Pregunta
All of the following are risk factors for developing a PE, EXCEPT:
Respuesta
-
Venostasis, vessel wall inflammation
-
Known hypercoaguable state
-
Pregnancy
-
Prolonged strenuous exercise
-
Recent surgery
Pregunta 54
Pregunta
While all of these are signs and symptoms of a PE, which are the most sensitive indications?
Respuesta
-
Tachypnoea and dyspnoea
-
Diaphoresis and tachycardia
-
Fever and syncope
-
Pleuritic chest pain and apprehension
-
Crackles on lung exam and cyanosis
Pregunta 55
Pregunta
All of the following are acceptable actions during pre-hospital transport of a patient with suspected pulmonary embolism, EXCEPT:
Respuesta
-
Supplemental oxygen to maintain SP02 above 95%
-
Pre-hospital 12-lead ECG
-
Heparin or low molecular weight heparin if approved by medical control during a prolonged transport
-
Intravenous thrombolytics if approved by medical control during a prolonged transport
-
Application of compression stockings and intravenous fluids titrated to keep the cannulated vein open
Pregunta 56
Pregunta
Match the situation with the type of emboli risk:
Fracture of a long bone (tibula/fibula) – [blank_start]FAT EMBOLI[blank_end]
At the end of the first stage of labour – [blank_start]AMNIOTIC FLUID EMBOLI[blank_end]
During placement of central cannulated lines – [blank_start]AIR EMBOLI[blank_end]
Prolonged immobilisation – [blank_start]BLOOD CLOT EMBOLI[blank_end]
Respuesta
-
FAT EMBOLI
-
AMNIOTIC FLUID EMBOLI
-
AIR EMBOLI
-
BLOOD CLOT EMBOLI
¿Quieres crear tus propios Tests gratis con GoConqr? Más información.