5818188
Descripción
Test por Rachel Nall, actualizado hace más de 1 año
|
|
Creado por Rachel Nall
hace alrededor de 8 años
|
|
Pregunta 1
Pregunta
A [blank_start]Standard of Care[blank_end] is the highest mandate for clinical behavior.
Respuesta
-
Standard of Care
Pregunta 2
Pregunta
Select the standard of nursing practice that most applies to CRNAs.
Respuesta
-
Standard III
-
Standard IV
-
Standard V
-
Standard VI
Pregunta 3
Pregunta
Fill in the blanks for the AANA Standards for Nurse Anesthesia Practice:
Standard V
A. Monitor [blank_start]ventilation[blank_end] continuously.
B. Monitor [blank_start]oxygenation[blank_end] continuously.
C. Monitor [blank_start]cardiovascular[blank_end] status continuously.
D. Monitor [blank_start]body temperature[blank_end] continuously.
E. Monitor [blank_start]neuromuscular function[blank_end] and status.
F. Monitor and assess the [blank_start]patient positioning[blank_end].
Respuesta
-
ventilation
-
oxygenation
-
cardiovascular
-
body temperature
-
neuromuscular function
-
patient positioning
Pregunta 4
Pregunta
One of the key components to patient safety is to: [blank_start]Avoid turning your back on the patient[blank_end] and surgical procedure for long periods of time.
Respuesta
-
Avoid turning your back on the patient
Pregunta 5
Pregunta
[blank_start]Monitors[blank_end] are placed first and removed last.
Respuesta
-
Monitors
Pregunta 6
Pregunta
Name two ways (in alpha order) that CRNAs monitor the respiratory system:
1. [blank_start]Capnography[blank_end]
2. [blank_start]Pulse oximetry[blank_end]
Respuesta
-
Capnography
-
Pulse oximetry
Pregunta 7
Pregunta
What is the standard of care for monitoring of oxygenation?
Respuesta
-
Arterial blood gas
-
Capnography
-
Pulse oximetry
Pregunta 8
Pregunta
The Beer-Lambert Law is a method for measuring what?
Respuesta
-
Capnography
-
Arterial blood gas
-
Pulse oximetry
Pregunta 9
Pregunta
Drag and drop the spectrum of light to the appropriate type.
Red: [blank_start]660[blank_end] nm
Infrared: [blank_start]940[blank_end] nm
Respuesta
-
660
-
940
Pregunta 10
Pregunta
The Beer-Lambert Law and pulse oximetry measures the difference between absorbed light by [blank_start]oxyhemoglobin[blank_end] relative to [blank_start]deoxyhemoglobin[blank_end] in a pulsatile ([blank_start]arterial[blank_end]) bed.
Respuesta
-
oxyhemoglobin
-
deoxyhemoglobin
-
arterial
Pregunta 11
Pregunta
[blank_start]Oxyhemoglobin Dissociation Curve[blank_end]: The percentage of hemoglobin saturation with oxygen at different partial pressures of oxygen in blood is described by this S-shaped curve.
Respuesta
-
Oxyhemoglobin Dissociation Curve
Pregunta 12
Pregunta
Insert the appropriate corresponding numbers for the oxygen-hemoglobin dissociation curve.
At an 02 reading of 97 percent, the Pa02 is likely [blank_start]100[blank_end].
At an 02 reading of [blank_start]90[blank_end] percent, the Pa02 is usually 60.
At an 02 reading of 83 percent, the Pa02 is usually [blank_start]50[blank_end].
Respuesta
-
100
-
50
-
90
Pregunta 13
Pregunta
Your patient's pulse oximeter isn't reading well. What are some potential causes?
Low flow conditions
• [blank_start]Hypotension[blank_end]→vasoconstrictionoftheperiphery
– Motion artifact
– Nail polish
– Ambient light interference – [blank_start]Dysfunctional hemoglobin[blank_end]
• Fetal hemoglobin
• Hemoglobin S
– Carboxyhemoglobinemia
• 240timestheaffinityforhgbvs.O2. – Methemoglobinemia
– Methylene blue, indigo carmine
Respuesta
-
Hypotension
-
Dysfunctional hemoglobin
Pregunta 14
Pregunta
Name the three ways we verify intubation:
1. [blank_start]Auscultation[blank_end]
2. [blank_start]Chest excursion[blank_end]
3. Confirmation of [blank_start]CO2 in expired gases[blank_end].
Respuesta
-
Auscultation
-
Chest excursion
-
CO2 in expired gases
Pregunta 15
Pregunta
What is an early indicator of esophageal intubation and airway disconnect?
Respuesta
-
Arterial blood gas
-
Capnography
-
Pulse oximetry
Pregunta 16
Pregunta
[blank_start]Capnography[blank_end] continuously monitors all of the following:
– Alveolar ventilation
– Pulmonary perfusion
– Respiratory patterns
– Correct placement of endotracheal tube
Respuesta
-
Capnography
Pregunta 17
Pregunta
Match the type of capnography with its description:
[blank_start]Main-Stream Capnographs[blank_end] (non-diverting or flow-through):
CO2 sensor located between endotracheal tube and breathing circuit
[blank_start]Side-Stream Capnographs[blank_end]: (Diverting or aspiration):
Sensor is located in the main unit and CO2 is aspirated via a sampling tube connected to a T-piece adapter located between endotracheal tube and breathing circuit.
Respuesta
-
Main-Stream Capnographs
-
Side-Stream Capnographs
Pregunta 18
Pregunta
Name two potentially fatal conditions that may first be indicated by capnographic changes:
[blank_start]Pulmonary embolism[blank_end]
[blank_start]Malignant hyperthermia[blank_end]
Respuesta
-
Pulmonary embolism
-
Malignant hyperthermia
Pregunta 19
Pregunta
Use of [blank_start]capnography[blank_end] has markedly decreased incidence of unrecognized esophageal intubation and their associated brain injuries and deaths
Respuesta
-
capnography
Pregunta 20
Pregunta
Label the following image with the appropriate portions of the expiratory segment.
{kind=link}
Respuesta
-
Beginning of exhalation
-
Gas exhalation alveolar capillary bed
-
Alveolar plateau, C02-rich gas
-
Inspiration
Pregunta 21
Pregunta
Label the appropriate angle segments of the expiration of capnography.
{kind=link}
Respuesta
-
Alpha angle
-
Beta angle
Pregunta 22
Pregunta
Which of the following options describes Phase I of the expiratory segment?
Respuesta
-
Exhalation of gas from the alveolar capillary bed mixing with dead space gas
-
Positive slope due to continuous excretion of CO2 into alveoli
-
Gas exchange that is free of CO2
-
Used to assess extent of breathing
Pregunta 23
Pregunta
In capnography, what is part of the expiratory segment?
Respuesta
-
Phase 0
-
Phase I
-
Phase II
-
Phase III
Pregunta 24
Pregunta
In capnography, the [blank_start]alpha[blank_end] angle is between Phases II and III.
The [blank_start]alpha[blank_end] angle is an indirect indication of the V/Q status of the lung.
The [blank_start]beta[blank_end] angle is between Phase III and descending limb of inspiratory segment.
The [blank_start]beta[blank_end] angle is used to assess the extent of rebreathing.
Respuesta
-
alpha
-
beta
-
alpha
-
beta
-
alpha
-
beta
-
alpha
-
beta
Pregunta 25
Pregunta
Fill in the blanks for the five characteristics of capnogram that should be evaluated:
-Frequency
-Rhythm
-[blank_start]Height[blank_end]
-Baseline
-[blank_start]Shape[blank_end]
Respuesta
-
Height
-
Shape
Pregunta 26
Pregunta
Your patient has low or no ETCO2 -- what are two of the major causes?
[blank_start]Decreased CO2 production/delivery[blank_end].
Causes: Hypothermia
[blank_start]Decreased pulmonary perfusion[blank_end].
Causes: Hypovolemia
Hypotension
Pulmonary embolism
Decreased cardiac output (arrest)
Respuesta
-
Decreased CO2 production/delivery
-
Decreased pulmonary perfusion
Pregunta 27
Pregunta
Select some causes of low ETCO2.
Respuesta
-
Altered alveolar ventilation
-
Increase CO2 production/delivery
-
Increased pulmonary perfusion
-
Technical errors/machine faults
Pregunta 28
Pregunta
Match the causes of low ETCO2 to the examples (in alpha order)
Altered Alveolar Ventilation
[blank_start]Apnea (accidental extubation)[blank_end]
[blank_start]Hyperventilation[blank_end]
[blank_start]Increase in dead space ventilation[blank_end]
[blank_start]Partial/total airways obstruction[blank_end]
Technical Errors/Machine Faults
[blank_start]Esophageal intubation[blank_end][blank_start]Sampling line leak[blank_end]
[blank_start]Ventilator malfunction[blank_end]
Respuesta
-
Apnea (accidental extubation)
-
Hyperventilation
-
Increase in dead space ventilation
-
Partial/total airways obstruction
-
Esophageal intubation
-
Sampling line leak
-
Ventilator malfunction
Pregunta 29
Pregunta
Name the two chief causes of elevated CO2.
[blank_start]Increased CO2 production/delivery[blank_end].
[blank_start]Increased pulmonary perfusion[blank_end]
Respuesta
-
Increased CO2 production/delivery
-
Increased pulmonary perfusion
Pregunta 30
Pregunta
Drag and drop the cause of the elevated ETCO2 with its cause:
Increased CO2 production/delivery.
[blank_start]Fever[blank_end]
[blank_start]Hyperthyroid storm[blank_end]
[blank_start]Laparoscopic surgeries[blank_end]
[blank_start]Malignant hyperthermia[blank_end]
[blank_start]Right-to-Left Shunts[blank_end]
[blank_start]Sepsis[blank_end]
[blank_start]Shivering[blank_end]
[blank_start]Sodium bicarbonate[blank_end]
[blank_start]Tourniquet[blank_end]
Increased pulmonary perfusion
[blank_start]Increased blood pressure[blank_end]
[blank_start]Increased cardiac output[blank_end]
Respuesta
-
Fever
-
Hyperthyroid storm
-
Laparoscopic surgeries
-
Malignant hyperthermia
-
Right-to-Left Shunts
-
Sepsis
-
Shivering
-
Sodium bicarbonate
-
Tourniquet
-
Increased blood pressure
-
Increased cardiac output
Pregunta 31
Pregunta
Select some examples of elevated CO2 causes.
Respuesta
-
Hyperventilation
-
Hypoventilation
-
Bronchial intubation
-
Exhausted CO2 absorber
-
Apnea/circuit disconnect
-
Malignant hyperthermia
-
Sepsis
Pregunta 32
Pregunta
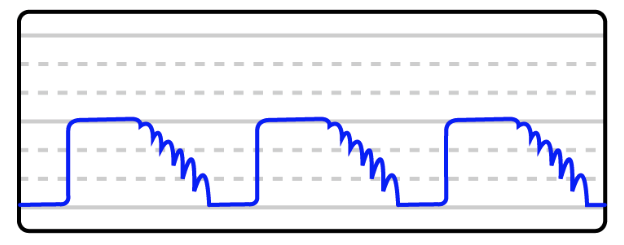
You notice your patient is experiencing small breaths at various points in the ETCO2 waveform. What is NOT a potential cause of this?
Respuesta
-
Inadequate muscle paralysis
-
Improper ventilator settings
-
Excessive oxygenation
-
Pressure on the patient's chest
Pregunta 33
Pregunta
Cardiac oscillations are most prominent in what patient population?
Respuesta
-
Adult
-
Elderly
-
Pediatric
-
Pregnant
Pregunta 34
Pregunta
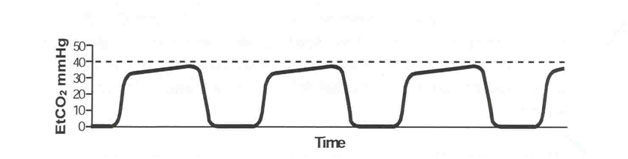
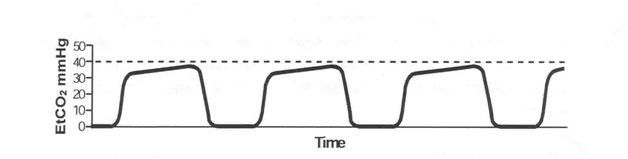
[blank_start]Cardiac oscillations[blank_end] are small gas movements produced by pulsations of the aorta and heart.
Respuesta
-
Cardiac oscillations
Pregunta 35
Pregunta
This image is an example of what on a capnograph?
{kind=link}
Respuesta
-
Cardiac oscillations
Pregunta 36
Pregunta
Other considerations/things that may mimic [blank_start]cardiac oscillations[blank_end]
– negative intrathoracic pressure
– low respiratory rate
– low I:E ratio
– Waning muscle relaxation
Respuesta
-
cardiac oscillations
Pregunta 37
Pregunta
Phase II and III are prolonged or slanted when a patient experiences a [blank_start]prolonged expiratory upstroke[blank_end].
Respuesta
-
prolonged expiratory upstroke
Pregunta 38
Pregunta
You are administering anesthesia when you suddenly notice your patient's baseline is elevated. You immediately:
Respuesta
-
Check for disconnections
-
Look at your CO2 absorbent
-
Change the I:E ratio
-
Increase your patient's sedative
Pregunta 39
Pregunta
You see the capnograph below during your case. You know this is a sign of:
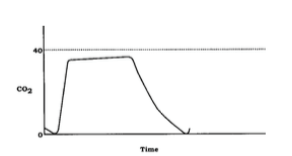{kind=link}
Respuesta
-
Exhausted CO2 absorbent
-
Airway obstruction
-
Cardiac oscillations
-
Inspiratory valve malfunction
Pregunta 40
Pregunta
An [blank_start]expiratory valve[blank_end] defect allows exhaled CO2-rich gases to be rebreathed with each inspiration.
Respuesta
-
expiratory valve
Pregunta 41
Pregunta
ETC02 is indicative of [blank_start]alveolar[blank_end] CO2.
Respuesta
-
alveolar
-
arterial
Pregunta 42
Pregunta
You have two CO2 readings: 38 and 43. Which one is the arterial concentration or PACO2?
Respuesta
-
38
-
43
Pregunta 43
Pregunta
The [blank_start]facial[blank_end] nerve is the better site to monitor for onset of block because the larynx also mimics the response of the diaphragm.
Respuesta
-
facial
-
ulnar
Pregunta 44
Pregunta
The [blank_start]ulnar[blank_end] nerve is the best nerve to monitor for recovery.
Respuesta
-
facial
-
ulnar
Pregunta 45
Pregunta
Match the pattern of stimulation to its stimulus.
[blank_start]Single stimulus:[blank_end] The simplest mode of stimulation; consists of a single supramaximal electrical stimulus that is delivered from every 1 to 10 seconds (1‐0.1 Hz)
[blank_start]Train of Four:[blank_end] Four successive 200 μs stimuli at 2Hz delivered every 0.5 seconds for 2 seconds
[blank_start]Double Burst Stimulation:[blank_end] delivers two bursts (at 50Hz) of three electrical stimulations separated by 750 sec followed later by two such impulses
[blank_start]Tetanus:[blank_end] Repetitive, high-frequency stimulation at frequencies of 50 Hz or greater for five seconds
Respuesta
-
Single stimulus:
-
Train of Four:
-
Double Burst Stimulation:
-
Tetanus:
Pregunta 46
Pregunta
Which form of peripheral nerve monitoring is based on the concept that acetylcholine is depleted by successive stimulation?
Respuesta
-
Single stimulus
-
Train of four
-
Double-burst stimulation
-
Tetanus
Pregunta 47
Pregunta
In Train of Four stimulation, no twitches equals what kind of blockage?
Respuesta
-
75
-
80
-
90
-
100
Pregunta 48
Pregunta
Clinical relaxation usually require what percentage of neuromuscular blockage?
Respuesta
-
50 to 60 percent
-
60 to 70 percent
-
75 to 95 percent
-
100 percent
Pregunta 49
Pregunta
What PNM improves accuracy over the T4/T1 ratio by delivering a stronger stimulation and eliminating the second and third twitches?
Respuesta
-
Double burst stimulation
-
Single burst stimulation
-
Tetanus
Pregunta 50
Pregunta
Which PNM option may provide an indication of the time until return of the first response in the TOF and subsequent readiness for reversal of neuromuscular blockage?
Respuesta
-
Tetanus
-
Post-Tetanic Potentiation
-
Train of Four
-
Double-Burst Stimulation
Pregunta 51
Pregunta
Which of the following muscle groups are most sensitive to neuromuscular blocking agents?
Respuesta
-
Diaphragm and Masseter
-
Extra ocular and adductor pollicis
-
Diaphragm and Orbicularis oculi
-
Adductor pollicis and Orbicularis oculi
¿Quieres crear tus propios Tests gratis con GoConqr? Más información.