9532135
Descripción
Test por Narda Carrion-Hernandez, actualizado hace más de 1 año
|
|
Creado por Narda Carrion-Hernandez
hace más de 7 años
|
|
Pregunta 1
{kind=link}
Respuesta
-
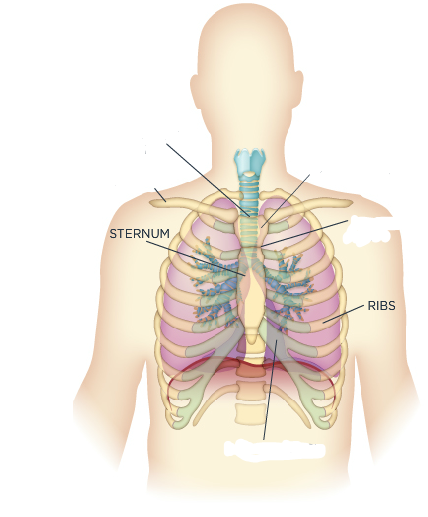
suprasternal notch
-
manubrium
-
clavicle
-
angle of louis
-
rib cartilage
Pregunta 2
Pregunta
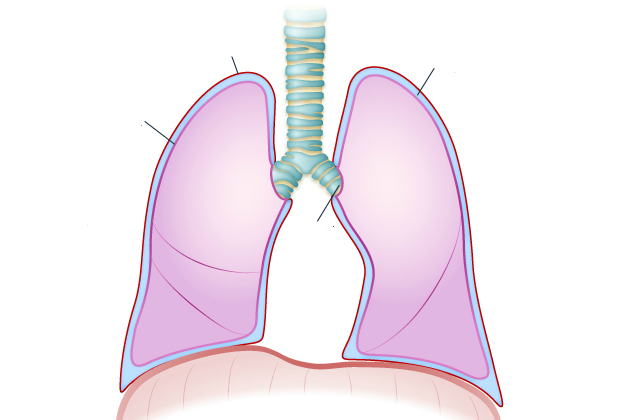
The lungs are attached to the thoracic cavity at the [blank_start]hilum[blank_end] and the [blank_start]pulmonary ligament[blank_end]. The parietal and visceral pleura meet at the [blank_start]hilum[blank_end] to create a sheath for the mainstream bronchi, the pulmonary vessels, and the nerves. The apex rises slightly above the level of the clavicle. The base rests on the diaphragm.
The space between the lungs is the [blank_start]mediastinum[blank_end]. It contains the heart, the great vessels, the esophagus, and the lymphatics.
Respuesta
-
hilum
-
pulmonary ligament
-
hilum
-
mediastinum
Pregunta 3
{kind=link}
Respuesta
-
parietal pleura
-
pleural space
-
visceral pleura
-
hilum
Pregunta 4
{kind=link}
Respuesta
-
sternocleidomastoid
-
external intercostals
-
scalene
-
internal intercostals
-
obliques
-
rectus abdominis
-
diaphragm
Pregunta 5
Pregunta
Inspiration is an active process. The [blank_start]medulla[blank_end] sends and impulse down the [blank_start]cervical plexus[blank_end] to the [blank_start]phrenic nerve[blank_end], stimulating the diaphragm to contract. Because the [blank_start]phrenic nerve[blank_end] receives impulses through the [blank_start]cervical plexus[blank_end] at the level of the fourth cervical nerve, spinal injury between the level of the 3rd and 5th cervical nerves will affect ventilatory function.
Respuesta
-
medulla
-
cervical plexus
-
phrenic nerve
-
cervical plexus
-
medulla
-
phrenic nerve
-
phrenic nerve
-
medulla
-
cervical plexus
-
phrenic nerve
-
medulla
-
cervical plexus
-
cervical plexus
-
medulla
-
phrenic nerve
Pregunta 6
Pregunta
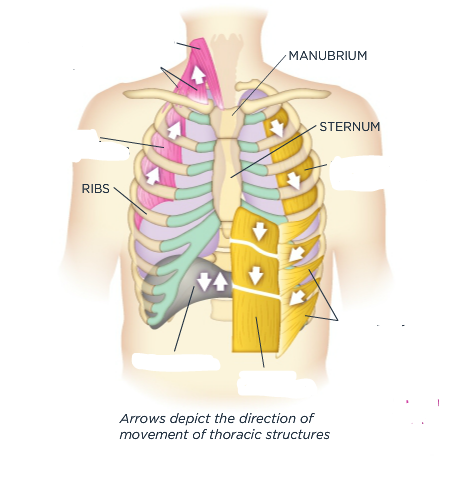
In expiration, the diaphragm relaxes and resumes its dome shape, pushing upward on the lungs. The lungs, chest wall, and abdomen recoil elastically, compressing the lungs and ejecting the air, similar to a balloon collapsing. The [blank_start]internal intercostal[blank_end] muscles help pull the ribs downward.
During forced expiration, coughing, physical exertion, or airway obstruction, expiration becomes and active process and requires recruitment of accessory muscles. Accessory muscles include the [blank_start]abdominal[blank_end] muscles and [blank_start]internal intercostals[blank_end].
Respuesta
-
internal intercostal
-
abdominal
-
internal intercostals
Pregunta 7
Pregunta
The upper airways consist of the trachea, nasal and oral cavities, pharynx, and larynx. No gas exchange occurs in the conducting (upper) airways.
Respuesta
- True
- False
Pregunta 8
Pregunta
The trachea is a hollow tube about [blank_start]4.5[blank_end] in long and one inch in diameter. It starts at the cricoid cartilage and extends to the carina, where it bifurcates into the mainstem bronchi.
Respuesta
-
4.5
Pregunta 9
Pregunta
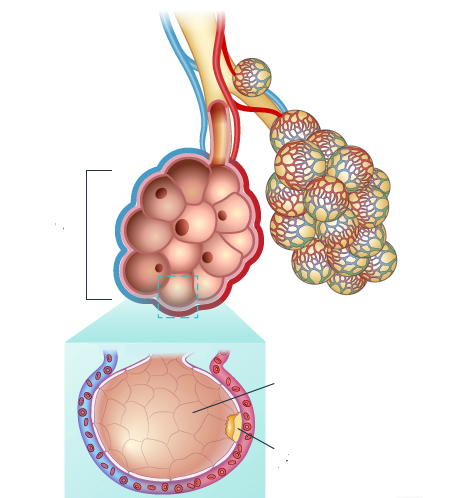
The alveoli comprises primarily type I and type II alveolar epithelial cells. Type I make up the majority of the alveolar surface which is where gas exchange takes places. Inhaled toxins easily injure Type I cells. Type II cells are small and numerous and move in when Type I are injured, eventually transforming into Type I cells. Type II cells produces, secrete and store pulmonary surfacant.
Label:
{kind=link}
Respuesta
-
alveolar sac
-
Type I cell
-
Type II cell
Pregunta 10
{kind=link}
Respuesta
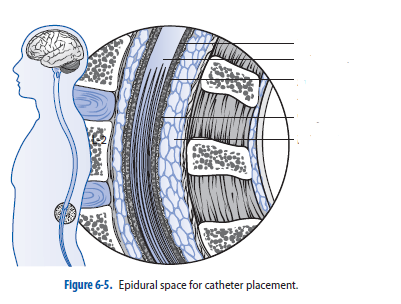
-
Pia matter
-
spinal cord
-
subarachnoid space
-
dura mater
-
epidural space
Pregunta 11
Pregunta
Bronchial circulation does not participate in gas exchange. Once blood circulates through and delivers its oxygen load, most of it is returned to the right side of the heart. A small amount travels via the pulmonary veins to the LA where it mixes with the fully oxygenated blood. This anatomical shunt results in an oxygen saturation of 96-99%. For this reason, a person breathing room air will never register an arterial oxygen saturation of 100%.
Respuesta
- True
- False
Pregunta 12
Pregunta
When the muscles of inspiration contract to create a larger space within the chest, the [blank_start]parietal pleura[blank_end] moves outward, increasing negative pressure in the [blank_start]intrapleural space[blank_end]. Intrapleural pressure drops from a resting pressure of -4 cm H2O to -10 cm H2O. This negative pressure creates pull on the [blank_start]visceral pleura[blank_end] and the lungs expand. At this point, pressure inside the lungs is less than atmospheric pressure, so air moves into the lung.
During expiration, the muscles of the thorax relax, compressing the lungs and increasing intrapulmonary pressure. When intrapulmonary pressure becomes greater than atmospheric pressure, air moves out of the lungs.
Respuesta
-
parietal pleura
-
visceral pleura
-
intrapleural space
-
intrapleural space
-
visceral pleura
-
parietal pleura
-
visceral pleura
-
parietal pleura
-
intrapleural space
Pregunta 13
{kind=link}
Respuesta
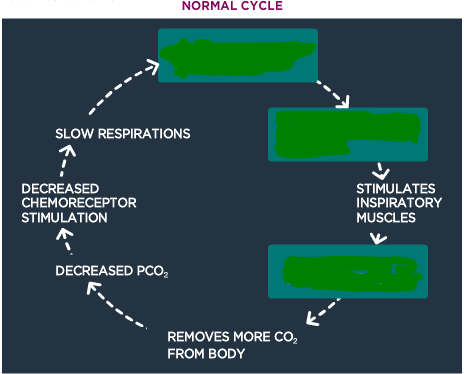
-
Increased PCO2 in blood and CSF
-
Stimulates chemorecep in medulla
-
Increases RR
Pregunta 14
{kind=link}
Respuesta
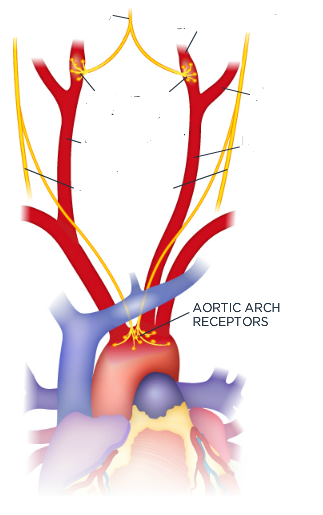
-
carotid sinus nerve
-
Left external carotid artery
-
carotid sinus receptors
-
Left internal carotid receptor
-
Left Common Carotid artery
-
Right Common Carotid artery
-
vagus nerve
Pregunta 15
Pregunta
During ventilation, central and peripheral chemoreceptors respond to changes in blood and other fluid chemistry. Additional sensors include juxtacapillary receptors (J-receptors), and receptors attuned to stretch and irritants.
Respuesta
- True
- False
Pregunta 16
{kind=link}
Respuesta
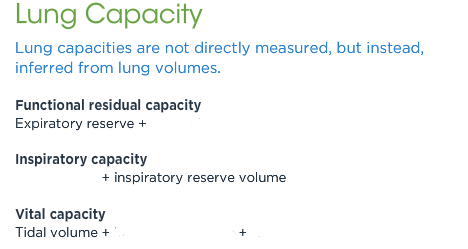
-
residual volume
-
tidal volume
-
inspiratory reserve
-
expiratory reserve
Pregunta 17
Pregunta
Any time alveoli are dysfunctional, gas exchange is impaired. When alveoli are not ventilated but blood is still perfusing the area, [blank_start]intrapulmonary shunting[blank_end] occurs.
Respuesta
-
intrapulmonary shunting
Pregunta 18
Pregunta
Alveoli may be ventilated, but have no corresponding blood flow to pick up oxygen, as in the case of pulmonary emboli. This is also known as alveolar dead space, or a [blank_start]high V/Q shunt[blank_end].
Occurs when adequate blood flow surrounds underventilated alveoli. The clinical effect of [blank_start]low V/Q[blank_end] is similar to shunting, and may result from similar pathology.
Respuesta
-
high V/Q shunt
-
low V/Q shunt
-
low V/Q
-
high V/Q shunt
Pregunta 19
Pregunta
2,3 diphosphoglycerate (2,3 DPG) is an organic substance in red blood cells that affects the affinity of hemoglobin for oxygen. A dramatic increase in tissue oxygen requirements spurs an acute increase in 2,3 DPG production.
Respuesta
- True
- False
Pregunta 20
Pregunta
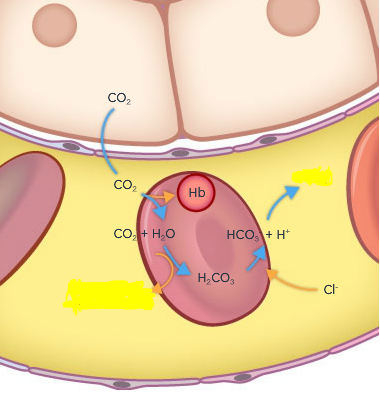
Carbon dioxide levels in the capillaries are lower than in the cells, allowing CO2 to move into the blood. Some carbon dioxide is carried dissolved in the plasma (indicated in the blood gas as PaCO2), some is bound to proteins including hemoglobin, but the majority is carried as HCO3 , the result of the formation and dissociation of carbonic acid.
As blood circulates back to the lungs, these compounds release the carbon dioxide, which then diffuses across the alveolar-capillary membrane into the alveoli in preparation for expiration.
Image:
Co2 (binary/octet-stream)
{kind=link}
Respuesta
-
HCO3-
-
carbonic anhydrase
Pregunta 21
Pregunta
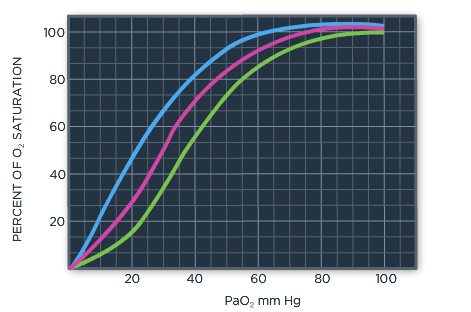
[blank_start]Right shift[blank_end] may be due to decreased blood pH, increased carbon dioxide (PaCO2), elevated temperature, and/or increased 2,3 DPG. When shifted right, oxygen is more easily detached from hemoglobin, enhancing delivery to tissues, even at lower oxygen saturation levels.
[blank_start]Left shift[blank_end] may be due to increased blood pH, decreased carbon dioxide, decreased temperature, and/or decreased 2,3 DPG. When the curve is shifted left, the bond between oxygen and hemoglobin is stronger and it is more difficult for hemoglobin to release oxygen to the tissue. Even if oxygen saturation is higher, tissue hypoxia may result.
{kind=link}
Respuesta
-
Right shift
-
Left shift
¿Quieres crear tus propios Tests gratis con GoConqr? Más información.