11817811
Descripción
Fichas por Anna Hogarth, actualizado hace más de 1 año
|
|
Creado por Anna Hogarth
hace alrededor de 7 años
|
|
| Pregunta | Respuesta |
| 1. Outline the responses of bronchiolar and arteriolar smooth muscle which maintain a balance between ventilation of the alveoli and blood flow (perfusion) to the alveoli in normal conditions. 2. Define the term ventilation perfusion ratio (Va/Q) and give values for the whole lung, the base and the apex of the lung in a normal subject in the upright position, explaining why these differ. Illustrate, by means of diagrams, how the perfusion of the lung may be considered in terms of different zones. 3. Comment briefly on the effects, on blood passing through the lungs, of a high or a low Va/Q. 4. Briefly explain the changes in circulation at birth (this will be covered again in more detail in the human development course). | X |
| What are the two physical circulations in the body? | Bronchial and pulmonary - bronchial is part of the systemic circulation and supplies the trachea and the bronchi. |
| Describe the bronchial venous drainage | The bronchial venous drainage is goes partly into the bronchial veins and into the right atrium but mainly goes into the pulmonary veins going into the left atrium. Pulmonary circulation is the output from the right heart to the lungs. |
| Where does the bronchial circulation arise from? What is it part of? How much of the left ventricular circulation does it receive? | 1) Aorta 2) Systemic circulation 3) 1-2% |
| Where does the pulmonary circulation arise from? How much of the right cardiac output does it receive? | 1) The right ventricle 2) 100% |
| Why must right heart output always match left heart output? How long does it take for blood to pass through the lungs? What is the total area for gas exchange? | 1) Pulmonary circulation is in series with systemic 2) 5 seconds 3) 50-100m^2 |
| What are the special anatomical features of the pulmonary arteries? Why are these important? | 1) The arteries are thin walled (far less muscle), large diameter lumens and are highly distensible and compressible 2) Allows the pulmonary arteries to stretch during systole - maintain a low systolic pressure |
| What is pulmonary blood flow equal to? What is the mean pulmonary pressure? Given a constant cardiac output from the left and right side of the heart what does this mean? What happens if pulmonary arterial pressure increases? | 1) Pulmonary blood flow = pulmonary pressure/pulmonary resistance 2) 15 mmHg 3) The pulmonary resistance is much lower than that of systemic (in order to accommodate the same cardiac output) 4) Can cause pulmonary arterial hypertension which can cause right heart hypertrophy and eventually failure. |
| Describe the various pressures in the right heart, left heart and pulmonary/systemic arterial/venous systems. | Important to note that the drop in pressure between the pulmonary arteries and veins is much less than that of the systemic. |
| What type of innervation do the lungs receive? What augments bronchial muscle dilation? Is there neuronal innervation of the pulmonary arteries? | 1) Sympathetic (T2-T6 of the paravertebral chain) postganglionic mingle with the vagus fibres from the pulmonary plexus, form plexi around the pulmonary arteries. SNS innervates B2-R in bronchial smooth muscle. The smaller the diameter of the airway the greater the receptor density. 2) Circulating adrenaline 3) No (or very little) - no need, and sympathetic innervation inhibits mast cells which can reduce inflammation in the lungs. |
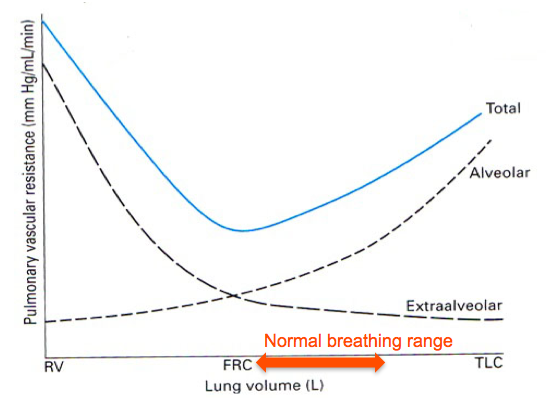
| What happens to alveolar and extra-alveolar capillary pressures during inspiration? | Alveolar capillaries are compressed as the alveolar expands resulting in negative pressure. Extra-alveolar capillaries are slightly pulled apart during inspiration due to the negative pressure, this decreases resistance. They are compressed during expiration. |
| X | |
| What is the mean pulmonary pressure in the pulmonary artery, lung apex and lung base? | 1) 15 mmHg 2) 2 mmHg 3) 25 mmHg |
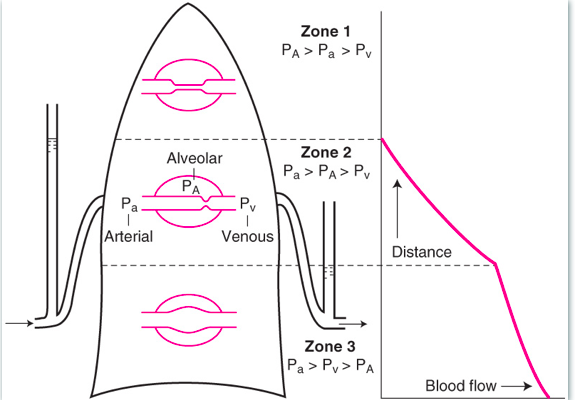
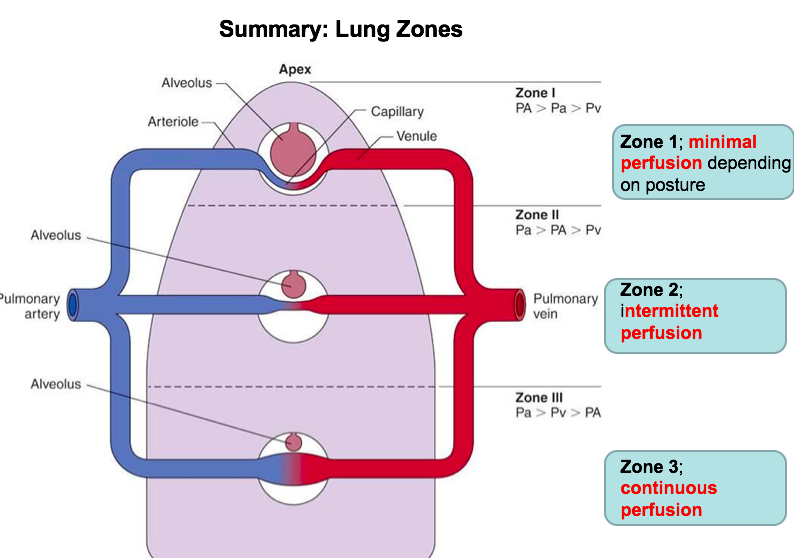
| What affect does gravity have on the perfusion of the lung? What model has this led to? | 1) Gravity causes pressure to be much greater at the base of the lung and much less at the apices. 2) Three zone model (when standing) Apices - very little blood flow Centres - pulsatile flow Bases - continual blood flow |
| In the original three zone model why was there thought to be no blood flow in the lung apices? Pulsatile flow in the middle? | 1) PA (alveoli) is greater the the Pa (arterioles - capillaries) - consequently the capillaries are completely compressed (lack of muscle) 2) Pulsatile because during inspiration PA (Alv) drops below atmospheric. Flow decreases suing expiration when Pa increases and partially blocks the capillaries. |
| X | |
| When does zone one actually become alveolar dead space? | In a normal healthy person pulmonary arterial pressure exceeds alveolar in all regions of the lung - only when a person is unwell (e.g. haemorrhage) or ventilated with possible pressure do the vessels in zone become completely collapsed by alveolar pressure, cutting of blood flow. Not much point in trying to ventilate the top zone of the lung if someone already has a lung condition. |
| Why is blood flow in the base of the lungs continuous? | Pulmonary arterial pressure (greatest) and pulmonary venous pressure always exceed alveolar pressure. Best zone for gas exchange. |
| How is the distribution of blood flow through an upright human lung measured? Why is a small zone 4 sometimes present at how does the blood flow here compare to zone 3? | 1) Radioactive xenon is injected into the venous supply - this ends up in the alveolar gas from pulmonary capillaries. Radiation counters can be used to assess the amount of radiation passing through each zone. 2) Zone 4 can be present at lung bases due to the pulmonary interstitial pressure compressing the capillaries at the base of the lungs - decreases blood flow. |
| X | |
| What does lung compliance measure? What is the equation? Where does is region in which the breathing is most efficient? | 1) Stretchability/distensibility 2) C = dV/dP Compliance = change in volume per unit pressure change 3) In the region of most compliance - i.e. least work for greatest change in volume. This is the most steep part of the 'S' shaped curve of the lung. This is both the normal and optimal zone for lung compliance. |
| How does compliance compare between the base and the apex of the lungs? What does this mean in terms of which region is better ventilated? | 1) Compliance is much higher at the base of the lungs than at the apex. 2) For a given pressure there is a greater change in volume of the base - hence the base of the lungs are better ventilated. |
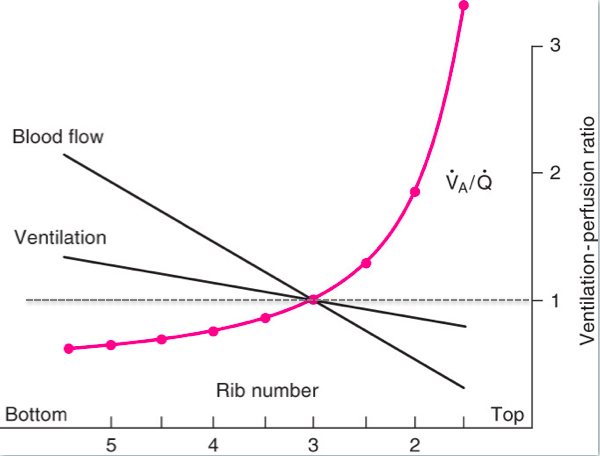
| How do blood flow and ventilation compare through the lungs? | Both blood flow and ventilation are higher at the base of the lungs. Blood flow is greater than ventilation at the base. Blood flow, however, decreases more steeply so that at the apices of the lungs, ventilation is greater than blood flow. |
| What is the VQ ratio? How does it change through the lungs (what are the absolute values)? | 1) VA/Q = perfusion ratio (alveolar ventilation/blood flow) 2) Greatly increases from base of lungs to apex (as apex has VA>Q). At the apex VQ is ~ 3.3, at the base VQ is ~ 0.6 |
| X | |
| What are the PaO2 and PaCO2 of the apex? Base? What does this say about the characteristics of both? What is the blood like in the venous return from the lungs? | 1) PaO2 - 130; PaCO2 - 28 2) PaO2 - 88; PaCO2 - 42 3) Apex is very good as gas diffusion but has poor blood flow, base is relatively poor at gas diffusion but has an excellent blood flow 4) Pulmonary veins contain a mix between the two. |
| What can the VQ ratio tell you about hypoxemia? What will the PO2/PCO2 begin to reach in both scenarios? | 1) If the airway is obstructed the V=O. VQ will also equal 0. The PO2 and PCO2 of that lung will start to reach that of mixed venous blood 2) If blood flow is obstructed then VQ will increase as Q decreases. Alveolar PO2 and PCO2 of a lung which is ventilated but not perfused will begin to reach that of inspired air. |
| What is the physiological response to pulmonary hypoxia? How does this arise? Why does this happen? | 1) Causes local vasoconstriction (Euler-Liljestrand response) 2) Release of local factors (not neuronal innervation) 3) Diverts blood away from areas of the lung which aren't being ventilated to better ventilated regions (opposite response to systemic hypoxia where you would try to increase blood flow through vasodilation). |
| What happens if hypoxia occurs in alveoli? When might this occur? | 1) Vasoconstriction in all pulmonary capillaries results in pulmonary arterial hypertension. This can lead to right atrial hypertrophy and eventually failure. 2) If you suddenly go to a high altitude, produces general hypoxia as the partial pressure of oxygen is much lower (although same concentration) as you go higher. |
| How does pulmonary circulation adapt to match increased cardiac output which occurs during exercise? | Cardiac output can increase by 4X during exercise. Pulmonary blood flow = pulmonary pressure/resistance. Pulmonary pressure does not change, instead the pulmonary arteries dilate during exercise to decrease resistance. |
| What are the three mechanisms which contribute to pulmonary arterial vasodilation? | 1) The thin walled arteries stretch with increased blood flow at the start of exercise. This generates a reflex relaxation of the arterial smooth muscle, widening the lumen and reducing resistance. 2) Increased ventilation at the start of exercise - the increase in PO2 and oxygen levels increases the production of NO from the pulmonary endothelium, maximising smooth muscle vasodilation. 3) Arteriovenous shunts can open in the lungs so that blood goes directly into the pulmonary veins from right heart - last resort for if the pulmonary blood flow is being overloaded as this blood won't be oxygenated. |
| Why is the foetal pulmonary vascular resistance so high? What is the adaption in place for this? What happens when the baby is born? | 1) Foetal pulmonary resistance is so high due to generalised hypoxic vasoconstriction in the fetal lungs (blood is oxygenated by mother, oxygenated blood enters through inferior vena cava) 2) The foramen ovale allows blood to be shunted from the right to the left atria 3) When the baby takes its first breath the pulmonary vascular resistance drops and the alveoli of the neonate become better oxygenated. Pulmonary blood flow becomes equal to systemic. |
| Why is a lack of closure of the foramen ovale potentially not a problem? | Pressure in the two atria is more or less the same. |
| What is the ductus arteriosus? What causes it and the foramen ovale to close/what happens if they don't close? How can these babies be treated? | 1) A shunt which goes directly from the pulmonary trunk to the aorta so that the oxygenated blood in the foetal right ventricle can bypass the lungs. 2) Both usually close when baby takes its first breath, drop in pulmonary pressure causes the structures to close. Lethal if they don't as lungs don't get perfused. 3) Treat with NO - in normal babies their first inspiration of O2 triggers the production of NO, in babies whose shunts don't close they lack NOS. Give them NO and they start producing NOS after a few days and it solves the immediate problem. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
¿Quieres crear tus propias Fichas gratiscon GoConqr? Más información.