1364294
Descripción
Fichas por Christine Su, actualizado hace más de 1 año
|
|
Creado por Christine Su
hace alrededor de 10 años
|
|
| Pregunta | Respuesta |
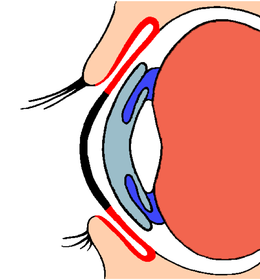
| Vitreous body | Clear gel-like substance filling the back portion of the eye (where floaters or cellular debris live) |
| Conjunctiva | Mucous membrane covering the sclera and inner lids |
| How do you assess the conjunctival membrane? | Pull down on lid to see while patient looks up |
| Sclera | Rigid, white outer shell of the eye |
| Chorioid | vascular layer between retina and sclera - where arteries and veins that perfuse the eye are located |
| Retina | Inner lining of the eye containing light sensitive rods and cones |
| Rods | super high light-sensitive cells how we see in low light light sensitivity and motion (peripheral vision due to rods) |
| How long does it take for rods to adjust in the darkness? | ~30 minutes |
| Cones | account for color and visual acuity (sharpness) |
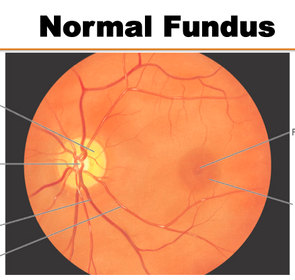
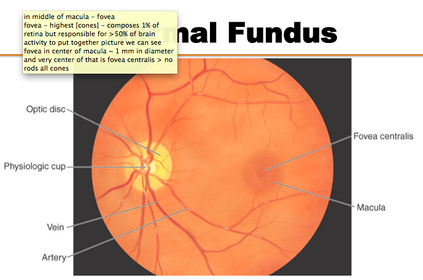
| Fovea | Located in middle of macula Highest concentration of cones Composes 1% retina but responsible for >50% brain activity 1 mm in diameter very center has all cones, no rods |
| Macular degeneration | Often occurs in older patients, but can also be accelerated in younger patients. Macula dysfunction so that there is blind spot in the middle of center focus. Must relearn to look at things peripherally. |
| Optic Nerve | Transmits visual stimuli from retina to brain via 2nd cranial nerve |
| Optic Disc | A circular area of retina, devoid of light receptors (blind spot) |
| Cornea | Clear, front part of eye Extension of sclera (white portion) Cornea is the clear part we see through |
| Lens | Clear, refracting media that focuses light. Responsible for high visual acuity. |
| Anterior Chamber | Clear fluid in front of the lens (in between cornea and lens) Important for diabetes patients because anterior chamber can change refractory of lens if there is a build up of glucose |
| Pupil | Round contractile orifice (hole) at the center of the iris that allows light in |
| Iris | Closed diaphragm that regulates amount of light entering. Controls pupil size. |
| Zonule | Suspensory ligament of the lens (suspends and holds lens in place in center of eye) |
| Ciliary Body | Produces aqueous fluid and controls thickness of the lens (focus) Can cause blurriness if no control over lens Manifests in myopia, astigmatism, progressive loss of vision |
| Cataracts | physical cause of focus control - loss of transparency of lens, which becomes opaque 50% of people who reach 70 have some sort of cataracts (William) Can replace lens |
| What are the consequences of cataracts? | Opaque lens Lose Contrast Add Blur Desaturation |
| What can cause gradual loss of vision? | Loss of focus control Cataracts Diabetic retinopathy Glaucoma |
| Glucose build up in anterior chamber can result in loss of visual acuity and can damage the retina | Diabetes Mellitus Diabetic Retinopathy |
| Protrusion of globe of eye Can see sclera all around the eye | Graves Disease Exophthalmos Proptosis |
| Drug side effects: Ethambutol | Optic neuritis Progressive loss of visual acuity Loss of color perception Usually reversible |
| Drug side effects: Thioridazine | pigmentary retinopathy pigment/color deposits in lens and retina Areas of pigments can't have same level of clarity |
| Drug side effects: Corticosteroids | Glaucoma Cataracts |
| Drug side effects: Rifampin | Ocular pain |
| Effects of allergies Medication allergies (mycins) | Ocular symptoms Higher incidence of allergies cause my medication allergies |
| Risk factors | Allergies Family History |
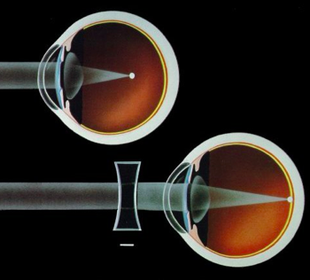
| Myopia | Nearsightedness Can see things closely Globe stretched longer Focus point occurs too early Negative diopter Concave lens correction |
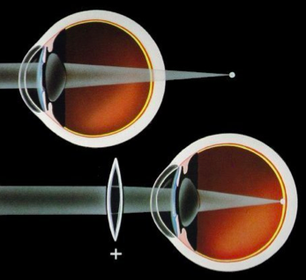
| Hyperopia | Farsightedness See things far Globe stretched up and down Focus point too far behind retina Positive Diopter Convex lens correction |
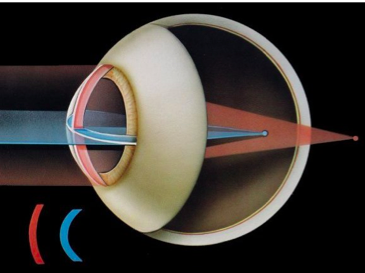
| Astigmatism | Corneal curvature is not regular Entering rays are not refracted the same Problems with both near/far vision Benefit from lasik surgery to shave cornea |
| Presbyopia | Due to aging Lessening of flexibility of lens Weakened ciliary muscle Can't accommodate quickly to change from near to far Progressive over time, must treat Why older people move things farther away when you try to show them things |
| Describe eye chart exam procedure | Patient reads chart from 20 ft away Cover one eye at a time Determine smallest line read without messing up Test w/o corrective lens first, then with E chart for kids/non-English speakers |
| Explain Snellen numbers Explain Diopter numbers | Snellen: 20/200 This person can see from 20 ft what a normal person can see from 200 ft (legally blind) Diopter: Amount of fix you put in lens to correct vision (-) is for myopia (+) is for hyperopia |
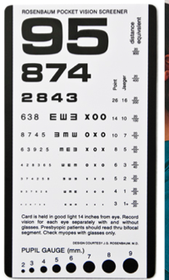
| Rosenbaum chart | Tests near vision Patient holds card about 14 in from eye Cover one eye at a time Test w/o corrective, then with Smallest line read without error |
| Confrontation Test | Peripheral vision test Stand opp pt at eye level ~ 1 meter away Each cover eye directly opp of each other Extend arm and move centrally until patient can see Test nasal, temporal, superior, interior Examiner as control Wiggle fingers |
| Inner/Outer Canthus | Inner/outer (temporal) corners of eye |
| Limbus | border between iris and sclera (the circle around iris) |
| Upper palpebral Fold | Fold of the eye (Palpebral = eyelid) |
| Caruncle | Inner canthus - the place where all the boogers come out of |
| Lacrimal gland | outer part where tears are stored and released (under the distal part of eyebrow) |
| Lacrimal Sac | Tear flow collected here (inner portion of eye) |
| Conjunctival Nevus | Eye mole Discoloration of sclera of eye |
| Xanthelasma | Irregular, yellowish plaque of cholesterol Deposited most commonly in nasal portion of upper or lower lid |
| Ptosis | Drooping of upper lid Causes: Neurologic Myogenic (muscle weakening) |
| Lice infestation | Looks like dandruff of eyelashes Nits will attach to hair shafts, close to body heat |
| Stye (Acute hordeolum) | Acute inflammation of an eyelash follicle Usually caused by Staphylococcus Small, painful Resolves quickly Acute onset |
| Chalazion | Caused by inflammation of a blocked meibomian gland (produces lubricating oils, have hundreds) Usually on upper lid, usually painless Can be mistaken for stye Bigger, can take months to go away Can cause visual abnormalities (astigmatism) |
| Blepharitis | Chronic inflammation of lid margin Redness and flaking Dryness, scales Causes: lice infestations, allergies, bacterial dermatitis (local irritation to skin) Characterized by excess oil production of glands near eyelid - bacteria can grow |
| Symptoms, Signs, and Causes of Conjunctivitis | Symptoms: red eyes (bilateral), gritty feeling, stickiness Signs: Swollen eyelids, mucoid discharge, dilated vessels Causes: bacterial/viral infections, trauma, sicca (dry eyes) |
| Pinguecula | A common, benign yellowish elevation, usually nasal Thickening of connective tissue |
| Keratitis | Corneal inflammation |
| Arcus senilus | a physiologic change occurring with age appears as a whitish ring in periphery of cornea occurs at age less than 40 may indicate hyperlipidemia |
| What do punctual plugs do? | Hold tears in eye longer Inserted in inner canthus/caruncle Tears have no place to drain out, keep moist |
| Conjunctivitis sicca | Severe form of dry eyes caused by rheumatic arthritis or Sjogren's syndrome causes grittiness, gush of tears in older patients Also can be caused by anticholinergics, diuretics, antihistamines |
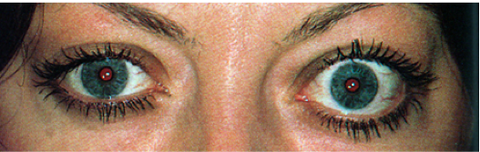
| Pupil Test: Response to Light | Shine penlight in eye with card in middle of eyes shielding the other from light Look for constriction Shine penlight in same eye and look for "consensual response" of opposite pupil. Repeat on other side. |
| Pupil Test: Accommodation | Ask patient to look at distant object Have patient switch focus to near object 10 cm from bridge of nose Pupils should constrict |
| What can cause miosis? (Pupil constriction) | Opioids Antipsychotics Some MAOIs Trazodone |
| What can cause Mydriasis? (pupil dilation) | Anticholinergics Antihistamines SSRIs SNRIs Amphetamine Cocaine Decongestants (phenylephrine) |
| Eye moves towards Nose | Adduction (cross eyed like a duck) |
| Eyes move toward ear | Abduction (eyes both moving outward looks absurd!) |
| Eyes rotating toward nose | INtorsion |
| Eyes rotating toward ear | EXtorsion |
| Eyes moving upward | Elevation |
| Eyes moving downward | Depression |
| Explain corneal light reflex test and what it tests for | Tests for balance of extraocular muscles 1. Point light to the middle of nasal bridge from 1-2 feet away. 2. Ask patient to look at examiner's nose 3. Light should be reflected symmetrically from both eyes. 4. If asymmetrical it is called ________. |
| Lack of parallelism of the visual axes of eyes. What is this called? What are its causes? What are the tests to determine this condition? | Strabismus. Causes: Cranial nerve disease Eye muscle weakness Brain malfunction Cover/Uncover Test, Corneal Light Reflex |
| Lazy eye towards middle | Estropia/Convergence Strabismus |
| Lazy eye towards ear (outward) | Exotropia/Divergence Strabismus |
| Explain the Cover-Uncover test | 1. Patient stares at a fixed point ahead 2. Cover one eye and observe uncovered eye for movement as it focuses on point 3. Remove cover and watch for movement of newly uncovered eye. 4. Repeat, covering the other eye. Movement of either eye may indicate esotropia or exotropia. |
| Explain H test and what it tests for. | Have patient follow finger/pen as you move in H pathway. Want to stress eyes to test for nystagmus and conjugate mvmt. |
| Nystagmus | Movement at exterior eye, where movement is jittery and spasmatic when stressed |
| Describe the Convergence test. | Patient follows pencil as you move it towards nose. Eyes should converge (cross-eyed). |
| When should you use the small aperture on ophthalmoscope? | For undiluted pupil |
| When should you use the large aperture on ophthalmoscope? | For dilated pupil |
| When should you use the fixation aperture on ophthalmoscope? | (crosshair) For measuring size/location. |
| When should you use the slit/streak aperture on ophthalmoscope? | To evaluate tumors and edematous discs |
| When should you use the cobalt filter aperture on ophthalmoscope? | Used with fluorescent dye to see small lesions and abrasions. |
| What structure should you examine last during a fundoscopic exam? | Macula (where all the rods are) |
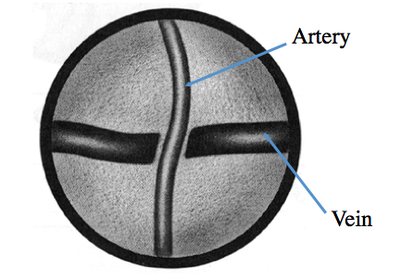
| T/F: When performing a fundoscopic exam, when you see the vasculature, veins are located in front of arteries. | False. Veins are behind the arteries. |
| What causes focal narrowing? | Vasospasms - column of wall narrows in one spot |
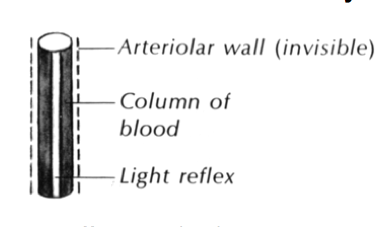
| What is a "copper wire" vascular change? | Light reflex increases more than 1/4 diameter of blood vessel. Copperish in color Vessel looks lighter. Indicates atherosclerosis. |
| What is a "silver wire" vascular change? | 100% light reflecting back, no longer see through blood vessel. Light is bouncing off the vessel walls, rather than column of blood. Indicated atherosclerosis. |
| How much of the blood vessel should the light reflex take up? | 1/4 of the diameter of the blood vessel. |
| What is arterio-venous nicking? | Nick means part of the arteriole is opaque (atherosclerosis). There is a change in arteriolar wall so it is no longer see-through. Because artery is in front of the vein and the part of the wall of the artery is opaque, you can't see it, so it looks like there's a nick. |
| What can happen to the fundus in a hypertensive patient? | Optic disc blurred Increased light reflexes in vessels AV nicking Cotton wool spots Exudates Hemorrhages All due to increased pressure |
| What can happen to fundus in a diabetic patient? | Coalesced exudates Microaneurysms Deep hemorrhages Notes: Microaneurysms caused by neovascularism, where the new blood vessels are not strong and balloon and stretch- easy to damage and bleed Blood, exudates decrease visual acuity, leading to retinopathy |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
¿Quieres crear tus propias Fichas gratiscon GoConqr? Más información.