2933685
Descripción
Fichas por jenny schneider, actualizado hace más de 1 año
|
|
Creado por jenny schneider
hace más de 9 años
|
|
| Pregunta | Respuesta |
| True or False: Drugs will differ in their apparent volume of distribution | True |
| True or False: A Vd of only a few litres suggests that the drug stays mainly in the vasculature system | True |
| What are two main factors that influence the RATE of drug distribution in the body? | membrane permeability of drug and tissue perfusion rate |
| What factors will affect membrane permeability? | MW of drug (small molecules can pass through easily) lipid solubility of drug (lipid soluble drugs can pass through membranes easily) pKa of drug can determine extent ionised and ionised drug is less lipid soluble; unionised can pass through membranes easily |
| True or False: permeability of drugs is increased in renal capillaries by pores in membrane of the endothelial cells while pores do not exist in the blood brain barrier, making passage of many drugs difficult | True |
| Which of the following tissues is/are highly perfused? heart, lungs, kidney, fat, bone | heart, lungs, kidney are highly perfused while fat tissue and bone is poorly perfused |
| What factors will affect the EXTENT of distribution of drug in body? | lipid solubility of drug pH and pKa of drug plasma protein binding tissue protein binding |
| What are some proteins in blood that drugs may bind to? | albumin alpha1 acid glycoprotein (AAG)\ lipoproteins |
| Acidic drugs usually bind to: a. albumin b. AAG | albumin |
| Basic drugs usually bind mainly to: a. albumin b. AAG | AAG |
| True or False: It is only the unbound or free drug that can exert effect at receptor/site of action | True |
| What doe we mean by total drug concentration in blood? | Drug may be present as drug bound to plasma proteins and as unbound drug in plasma. Therefore the total concentration is the sum of the drug bound to proteins and the unbound drug |
| If it is unbound or free drug which exerts effect, why can we often measure the total concentration and use this to relate to effect? | In many cases the fraction unbound does not change with dose or total concentration, therefore any changes in total concentration will be proportional to changes in the unbound concentration |
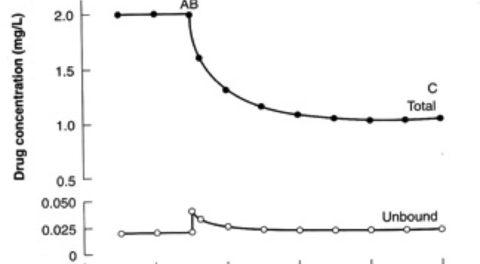
| Explain this plot where patient is receiving A and B is administered (both A and B are highly bound to same protein) | Drug B displaces A which is now free to distribute more widely in body, reducing plasma concentration or to be eliminated (e.g. kidney or liver and this will also lower concentration). After an initial "blip" the unbound concentration will remain same and the total drug concentration will have decreased |
| Explain what can happen to phenytoin binding in the presence of renal or hepatic disease and why | phenytoin is highly protein bound. In liver disease, there may be a decrease in albumin present in blood and this can lead to increase in fu. In renal disease, there can be a change in affinity of drug for the albumin, leading to a change in fu |
| Why might a free (or unbound) drug concentration be requested for phenytoin in presence of liver disease or renal disease? | Because the fu differs in these patients- it may change from 10% to 20%. The total drug concentration may drop but fu increases. The therapeutic range for free concentration is 1-2mg/L. The therapeutic range for total concentration is 10-20mg/L. In patients without liver or renal disease, fu=01., so total concentration of 10-20mg/L will lead to 1-2mg/L as free drug. In disease, total concentration may drop to 5-10mg/L and fu increase to 20% so free drug is still in range 1-2mg/L but if we used total concentration, we may decide to increase dose when it does not need to be increased. |
| Explain why some drugs may concentrate in breast milk | Blood has pH7.4 and drug that is unionised at this pH may cross into breast milk. pH of breast milk is lower than blood and this may cause some drugs to ionise (e.g. weak bases) and they will not be able to cross back out of breast milk back into blood |
| True or False: With an obese patient, for a drug that distributes into body fat, we would tend to use total body weight if calculating Vd expressed in L/kg while if drug does not distribute well into adipose tissue, we would tend to use IBW | True |
| Using physiology model: Vd=Vp + (fu/fut)Vt what would happen to Vd of a drug if another drug was co-administered and the fu was increased? (assume Vp, Vt and fut do not change) | Vd would increase as fu increased |
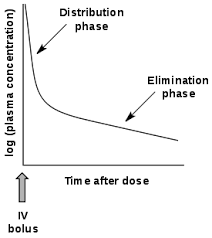
| After dosing a patient with digoxin, when should we take a blood sample for drug level monitoring? 3h after dose or wait at least 6h | wait at least 6h as digoxin follows two compartment model-has distribution phase- drug has to distribute to cardiac tissue and effect correlates best with trough level |
{kind=link}
{kind=link}
¿Quieres crear tus propias Fichas gratiscon GoConqr? Más información.