2978954
Descripción
Fichas por Annie Nguyen, actualizado hace más de 1 año
|
|
Creado por Annie Nguyen
hace más de 9 años
|
|
| Pregunta | Respuesta |
| List the 7 steps for Spirometry interpretation | 1. Six seconds long 2. Flow volume loop shape 3. FEV1/ FVC >70% 4. FVC > 80% 5. FEV1 > 80% 6. ID pattern 7. Classify Severity |
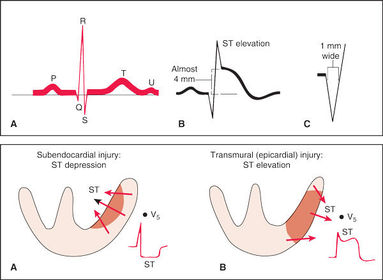
| LV hypertrophy: Increased R wave peak time:Left ventricular strain pattern: *T wave inversion in the lateral leads V5-6* | |
| Proventil HFA, ProAir, Xopenex is an example of ? | SABA: Short- acting beta agonist ( short-acting bronchodilator) |
| Aerospan, Flovent, Pulmicort and Qvar are examples of ? | ICS- inhaled corticosteriods |
| Foradil and Serevent are examples of ? | LABA |
| Atrovent, Combivent, Tudorza, and Spiriva are examples of ???? | Anticholinergics |
| Advair, Breo, Dulera, and Symbicort are examples of????? | Combo Medications: ICS and LABA |
| Gold Standard DX for COPD | Spirometry |
| Diagnostics for Asthma | 20% variation in PEF (liters/mins) Spirometry |
| Peak Flow Measurement 1. Stand___ 2. Cursor at _____ 3. Blow _____& _____ 4. Best of _____ attempts 5. Record _______ best. | 1. Stand up 2. Cursor at zero 3. Blow hard & fast 4. Best of 3 attempts 5. Record personal best. |
| Deaths from Asthma is best reduced by.... 1. written _______ plan 2. Oral _______ prior to severe attack 3. Use of Peak _____ meter ( Liters/mins.) | 1. written Action plan 2. Oral corticosteroids prior to severe attack 3. Use of Peak Flow meter ( Liters/mins.) |
| This type of Asthma Medication benefits those who are obese, smoke, or triad of asthma | Leukotriene medications: Singulair |
| Triad Asthma criteria | Nasal polyps ASA sensitivity Severe asthma |
| Asthma Control Test A score of ____ is controlled asthmatic. | <19 not controlled >20 is well controlled |
| What medication increase the risk of pneumonia in COPD patients? | Corticosteroid do not cause Pneumonia or osteoporosis in asthmatics, however those with COPD . |
| Peak Flow Monitoring 1. best lung function __ pm & lowest __am 2. ___% fluctuation is healthy 3. ___% variation DX of asthma 4. NOT USED FOR _____. | 1. best lung function 4 pm & lowest 4am 2. 8% fluctuation is healthy 3. 20% variation DX of asthma 4. NOT USED FOR COPD. * effort dependent* |
| Schedule of Asthma Follow up 1st F/U within ____ month. Routine visit ___ to ___ months. | 1st F/U within 1 month. Routine visit 1 to 6 months. *assess correct use of inhaler, spacer, peak flow meter (PFM)* |
| COPD is not fully ________. | COPD is not fully reversible. Preventable and treatable. |
| Productive cough for 3 consecutive months for 2 consecutive years. | Chronic Bronchitis |
| COPD SOB manifest at __ % of lung function | SOB manifest at 50 % of lung function |
| PATHO of COPD 1. increases in ______ and neutrophils. 2. ______ hyperplasia. 3. Bronchiolar ______. 4. Peribronchiolar ________. 5. Loss of _______ attachments. | 1. increases in macrophages and neutrophils. 2. bronchiolar hyperplasia. 3. Bronchiolar edema. 4. Peribronchiolar fibrosis. 5. Loss of alveolar attachments. |
| COPD presentation 1. SXS present at 1 PPD for > ____ years. 2. manifestation at _____ decade: chronic cough after viral infx. 3. Dypsnea at ___ or ____ decade. | 1. SXS present at 1 PPD for > 20 years. 2. manifestation at fifth decade: chronic cough after viral infx. 3. Dypsnea at sixth or seventh decade. |
| COPD Physical Exam 1. ______ and _____ expiration. 2. Chest wall _______inflation. 3. Distant _____ and ____ sounds. 4. Pursed ____ breathing. 5. Cor ______: JVD, edema, heptomegaly | 1. Slow and prolonged expiration. 2. Chest wall hyperinflation. 3. Distant heart and breath sounds. 4. Pursed lip breathing. 5. Cor pulmonale: JVD, edema, heptomegaly |
| COPD Chest Xray | COPD Chest XRAY 1. flat diaphragm 2. tear shaped heart 3. Increase AP/ retrosternal airspace *Emphysema: pruning of pulmonary vessels and bullae* |
| COPD assessment test (CAT) < 10 > 10 | Group A: low risk, less SXS (CAT< 10) Group B: low risk, more SXS (CAT>10) Group C: high risk, less SXS (CAT< 10) Group D: high risk, high SXS (CAT >10) *GROUP B &D: 5x risk for cardiovascular dx and cancer* |
| COPD Treatment : 1st Choice Group A and B | Group A: SAAC (Atrovent/ combivent) or SABA (Proair, Proventil) Group B: LAAC (spiriva/anora ) or LABA (Foradil/ Serevent) * add- on exercise and pulmonary rehab* |
| COPD 1st choice treatment for Group C and D | Group C: LAAC (Anora/Spriva) and (+)LABA ( Foradil/Serevent) Group D: ICS (Flovent/ Pulmicort) and(+)LABA or LAAC * add- on exercise, oxygen therapy pulmonary rehab* |
| Spirometry List the predicted values/ criteria. | 1. Gender 2. Race 3. Age 4. height |
| ____ _____ _____ (FVC) maximum volume of air exhaled _____ _____ ______ (FEV1): volume exhaled during the first second. | Forced Vital Capacity: maximum volume of air exhaled Forced Expiratory Volume: volume exhaled during the first second. |
| Normal Lung Volume Values FEV / FVC1 >____% FVC > _____% FEV1 > _____% | Normal Lung Volume Values FEV / FVC1 >70% FVC > 80 % FEV1 > 80 % |
| Obstructive vs Restrictive Disease pattern Obstructive: FEV1 / FVC _____, FVC _____ FEV1_____ | Obstructive: FEV1 / FVC down , FVC normal, FEV1 down |
| Obstructive vs Restrictive Disease pattern Restrictive : FEV1 / FVC _____, FVC _____ FEV1_____ | Restrictive : FEV1 / FVC normal , FVC down FEV1 down Combined:FEV1 / FVC down, FVC down, FEV1 down |
| Obstructive Lung Diseases | Asthma COPD Bronchiectasis Cystic Fibrosis |
| Obstructive Reversibility defined as a change of ____% post Albuterol (SABA) or Ipratropium (Atrovent) and increase of _______ mL. | Obstructive Reversibility defined as a change of 12 % post Albuterol (SABA) or Ipratropium (Atrovent) and increase of 200 mL. |
| CAD inflammation marker. < 1 low risk for CV events 1-3 intermediate >3 high | High Sensitivity CRP (hs-CRP) |
| Which is an independent risk factor for CHD? HDL, LDL, Triglycerides | Elevated Triglycerides are an independent risk factor for CHD. Low HDL independent predictor (inverse relationship) Normal < 150 Borderline 150-199 High > 200- increased risk for pancreatitis |
| What are the criteria for Metabolic syndrome? Metabolic syndrome- 3+SXS to DX | 1. Abdominal obesity (M >40in. W> 35) 2. Triglyceride> 150 mg/dl 3. Low HDL ( M<40, W< 50) 4. High BP ( 130/85) 5. Fast blood glucose (> 110) |
| DXD for Dyslipidemia | 1. DM 2. Hypothyroidism 3. obstructive liver dx 4. Chronic renal failure 5. Protease inhibitor ( HIV meds) 6. BBB, HCTZ= low HDL 7. Prednisone ( high TG) 8. Tamoxifen- high TG ( Breast CA) |
| Non occlusive thrombus unstable angina and non-Q wave MI | |
| Occlusive thrombus Q wave MI and sudden death | |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
¿Quieres crear tus propias Fichas gratiscon GoConqr? Más información.