3645479
Descripción

Fichas por Natashia Reyes, actualizado hace más de 1 año
|
|
Creado por Natashia Reyes
hace más de 9 años
|
|
| Pregunta | Respuesta |
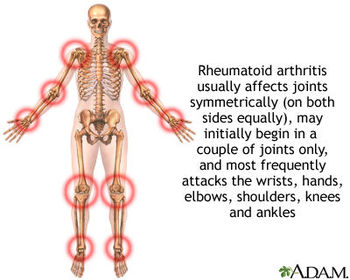
| Rheumatoid Arthritis what is it How is it characterized Which Joints Age | It is a chronic system autoimmune disease characterized by inflammation of the synovial joints with periods of remission and exacerbation accompanied by extraarticular manifestations peaking at 30-50 years |
| Antigen trigers formation of what immunoglobulin What is RF (rheumatoid factor) What happens with the immunoglobulin | abn. Immunoglobulin IgG RA characterized by auto-antibodies against IgG RF is auto-antibodies against IgG it combines with IgG to form immune complexes that deposit initially on synovial membranes/superficial articular cartilage o |
| Neutrophil Part T Helper Cells (CD4) What are the primary inflammatory factors | Attack the site of inflammation and release proteolytic enzymes damaging articular cartilage cause synovial thickening stimulate monocytes, macrophages, and synovial fibroblasts to secrete proinflammatory cytokines Il-1, iL-6 and TNF |
| Genetic link | Strongest evidence Human Leukoxyte antigens HLA especially HLA-DR4 and HLA-DR1 antigens |
| Four Stages of Rheumatoid Arthritis I: II: III: IV: | I: Early no destructive changes on x-ray no evidence of osteoporosis II: Moderate-X-Ray evidence of osteoporosis w/w/o slight bone or cartilage destruction. NO joint deformities, adjacent muscle atrophy, possible presence extraarticular sof |
| Nonspecific Manifestations | Fatigue, anorexia, weight loss, generalized stiffness all preceed arthritic complaints. Stiffness becomes more localized in following weeks to months. |
| Precipitating Factors | Infections, Stress, Physical exertion, Child Birth, Surgery, or Emotional |
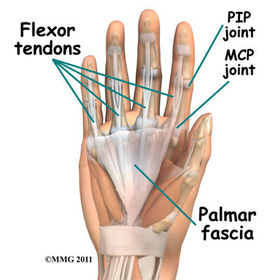
| Specific articular involvement Manifestations How do Joint Symptoms Occur and where | -pain, stiffness, limitation of movement, signs of inflammation (Heat, Swelling, Tenderness) -they occur symmetrically affecting the small joints of hands (PIP and MCP) larger joints may be involved wrists, elbows, knees, hips, and ankles |
| Characteristic Joint Stiffness Morning Stiffness May Last What typically swells | Occurs after periods of inactivity one to several hours PIP MCP |
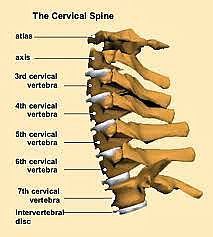
| Cervical spine effect of RA and Axial Skeleton | Cervical spine may be affected but axial skeleton spared (Spine and bones connected to it) |
| When can spindle shaped fingers occur Why Effect of motion on pain Is it always porportionate | Early on synovial hypertrophy and thickening of joint capsule Joint becomes painful, tender, and warm to touch Pain increases with motion, varies in intensity and no is not always equal |
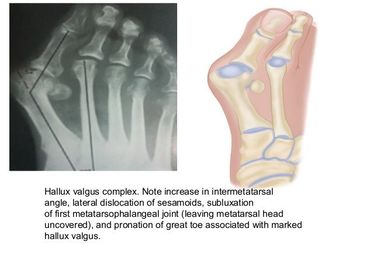
| What is Subluxatoin | Atrophy of muscles and destruction of tendons around joint cause one particular surface to slip past another |
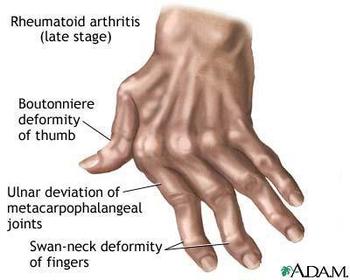
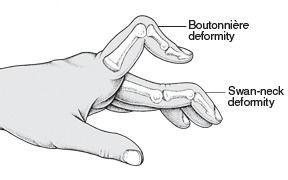
| Swan Neck | |
| Boutonniere Deformity | is a deformed position of the fingers or toes, in which the joint nearest the knuckle (PIP) is permanently bent toward the palm while the farthest joint (DIP) is bent back away (PIP flexion with DIP hyperextension) |
| Extraarticular Manifestations | Common in those with high levels of Biomarker RF: Rheumatoid Nodules, Peurisy, Pleural effusion, pericarditis, pericardial effusion, cardio myopathy, loss of vision from sclera nodules |
| Sjogren's Syndrome | Can occur by itself or in conjunction with RA like systemic lupus and is diminished lacrimal and salivary gland secretion, leading to dry mouth, burning itching eyes, decreased tearing, photosensitivity |
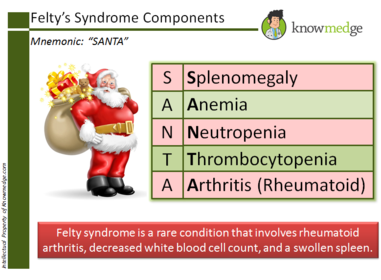
| Felty Syndrome | is a disorder that involves rheumatoid arthritis, a swollen spleen, decreased white blood cell count, and repeated infections. |
| DIAGNOSTICS: What is the Key Diagnostic What hapens to synovial fluid What indicates inflammation What indicates progressive joint damage What level is Synovial fluid at | Positive RF only in 80% ESR and C-reactive good indicators of inflammation ANA only in some pts leave alone (Antinuclear antibody) ACPA (IS KEY) Anti-citrullinated protein antibody is IMPORTANT diagnostic more specific than RF and allows earlier and more accurate dx Synovial fluid straw colored fluid with fibrin flecks Prog JD is MMP-3 increased in synovial fluid 25,000/uL elevated |
| X-ray and Rheumatoid Arthritis Bone scan and RA | Is inconclusive during early stages only shows soft tissue swelling and possible bone demineralization Bone scans WHERE IT'S AT! detect early changes and confirms dx so treatment can be initiated |
| Factors found in later disease Factors of Advanced Disease What monitors disease progression and tx effectiveness | Narrowing of joint space, destruction of articular cartilage, erosion, subluxation, deformity Malalignment and ankyloses Baseline films |
| Physical Therapy vs. Occupational Therapy | P-maintains joint motion and muscle strength O- develops upper extremity function and encourages joint protection through use of splints or other assistive devices or strategies for activity pacing |
| What is the cornerstone for RA as a drug | DMARDs-because joint damage can occur as early as first year! Methotrexate (Rheumatrex)-rapid antiinflammatory reduces symptoms in days to weeks S/E bone marrow suppression and hepatotoxicity monitor CBC and Chem Panel for hepatic and renal report anemia keep hydrated use contraceptin NEED WEIGHT LOSS |
| DMARDS | MSLP....Mathotrexate (Rheumatrex, Trexall) antimetabolit inhibits DNA, RNA, Protein synthesis sulfasalazine (Azulfinide, Salazopyrin) antiinflamm blocks prostaglandins synthesis-may cause yellow orange discoloration of skin space around he clock take w/8oz water Lefulnomide (Arava) antiinflam inhibits prolif of lymphocytes mon hepticfunction Penicillamine (Cuprimine, Depen) antiinflam montior WBC platelets, UA take 1-2hr before or after meals and 1 hr away from any other drug food or milk |
| Intraarticular or Systemic Corticosteroids | (-LONEs) Intraarticular-methylprednisolone acetate (Depo-Medrol) trimacinolone (Aristospan) inhibits synthesis or release of inflammatory modulators use strict aseptic technique joint may feel worse immediately after injection improvement lasts weeks to months avoid overuse immed after injection OKAY UNTIL DMARD TAKES EFFECT |
| Intraarticular or Systemic Corticosteroids | Systemic(HMDTP) ONE-ONE-ONE-ONE-hydrocortisone (Solu-cortef) methylprednisolone (Sol-medrol) dexamethasone (Decadron) prednisone and triamcinolone (Aristocort) same process only used in Life Threatening Exacerbation!! Or symptoms persist after less potent drugs use limited time step down method symptom exacerbation with abrupt stop monitor bp, weight, CBC, and Potassium Limit Sodium and Report infection!!! Temporarily reduce pain during flare |
| NSAID | ibuprofen (Motrin, Advil, Novo-Profen) naproxen (Naprosyn, Anaprox, Aleve) ketoprofen (orudis, Actron) piroxicam (Feldene, Novo-Pirocam) indomethaxin (Indocin, Indocid) sulindac (Clinoril, APo-Sulin NovoSundac), tolmetin (Tolectin), diclofenac (Voltaren), meclofenamate (Meclomen), nabumetone (Relfen) oxprozin (Daypro), meloxicam (Mobic), celecoxib (celebrix) |
| NSAID method and nursing indicaitons knowledge to know | antiinflammatory analgesic, antipyretic, act by inhibiting synthesis of prostaglandins Administer with food, mild, or antacids report signs of bleeding (tarry stools, bruising, petechiae, nosebleed) edema, skin rashes, persistent headache, visual disturbances monitor BP for fluid retention used regularly for max effect, may be up to 10-18 ASA/d |
| Biologic and Targeted Therapy | Tumor Necrosis factor, Interleukin-1 receptor antagonist, interleukin 6 receptor antagonist, T cell activation inhibitor, B cell depletion Agent |
| Tumor Necrosis Factor | Aentanercept (Enbrel) infliximab (Remicade) adalimumab (Humira) certolizumab (Cimzia) gloimumab (Simponi)---GAACI-SEHCR Binds to TNF thus blocking TNF cell surface receptors decreasing inflammatory response and immune |
| Tumor Necrosis Factor Knowledge | Evaluate for relief of pain, swelling, stiffness, and increase in joint mobility. Advise increased risk TB, yearly PPD needed. Monitor for infection bleeding, and emergence of malignancies. Psoriasis may worsen. Injection site reaction commonly occurs in first moth of treatment and decreases with continued therapy do not receive LIVE VIRUS vaccines during treatment |
| Interleukin Receptor 1 Antagonist | anakinra (Kineret) blocks the action of IL-1 decreasing inflammatory response Evaluate for relief of pain, swelling, stiffness and increased joint mobility. Advise joint site reaction generally occur in first month and decrease with continued therapy Evaluate renal function, monitor for infection DO NOT TAKE with TNF |
| Interleukin Receptor-6 Antagonist | tocolizumab (Actemra) Blocks action of IL-6 thus decreasing inflammatory response for pt's RA that has failed to respond to other infections monitor BP and for infection. Advise GI effects (perforation) monitor liver enzyme and LDL level |
| T Cell Activator | abatacept (Orencia) inhibits T cell activation thus suppressing immune system Not recommended for use with TNF inhibitors eval for relief of pain, swelling, stiffness, increased joint mobility |
| B Cell Depleting Agent | Rituximab (Rituxan) monoclonal antibody binding to CD20, an antigen on B celss destroying B cells and suppressing immune response Monitor for infection and bleeding, advise patient do not receive live virus monitor for Low BP if also taking bp med. Fatigue is common |
| Surgery: Synovectomy Arthroplasty | S-removal of joint lining synovium A-total joint replacement |
| Acute Intervention | Reduce inflammation, manage pain, maintenance of joint function, prevention or minimization of joint deformity |
| Nursing interventions | Balance rest and activity with joint protection, heat and cold application, exercise, pt and caregiver teaching, physical and occupational therapist, social worker to resport function and make lifestyle adjustements new dx tx outpatient hospitalization for extraarticular manifestations and advancing disease req surgery |
| Possble Diagnostic Findings | Positive RH factor, Elevated ESR, anemia, Elevated WBC in synovial fluid, evidence of joint space narrowing, bony erosion and deformity on x ray, osteoporosis with advanced disease |
| Intervention Assessments Begin With | Assessment of Joint pain, swelling, ROM, and general health status, sex, stress, finances, etx |
| Splinting | Lightweight splints to rest inflamed joint and prevent deformity from muscle spasms and contractures. Remove splints at regular intervals, give skin care, preform ROM exercises, after reapply as prescribed |
| Stiffness Care | Plan care around morning stiffness, sitting or standing in warm shower, sitting in tub with warm towels around shoulders, soaking hands in warm basin |
| REST Total Bed Rest Bed Flexion vs. Extension Pillow under knees | alternating periods of rest relieves pain, rest BEFORE exhaustion, NO total bed rest even mild disease needs daytime rest and 8-10 hours of sleep modify activities to avoid overexertion meal prep while sitting in a stool in front of sink. Firm mattress or bed board Encourage extension not Flexion decrease contracture by NEVER placing pillow under knee. EVER!!! only small flat pillow under head and shoulders |
| Joint Protection | Simplification techniques, work done in short periods with breaks or pacing, time saving such as can opener, carts to carry supplies, buttonhooks, lightweight plastic dishes, raised toilet seat, walker, shoes with velcro |
| Heat and Cold Therapy | Relief of stiffness Pain and Spasm Ice-during disease exacerbation Hot for chronic disease stiffness Heat should NEVER EXCEED 20 minutes COLD should never exceed 10-15 minutes Avoid heat cream with external heating devices |
| I Participate in Recreational Activity... So I Don't Need Therapeutic Exercise, Right? | Wrong walking or swimming does not eliminate this need |
| Exercise How Often What Allows Easier Movement During Accute Inflamation What? | ROM done daily, practice with supervision, Aquatic movement offering two way resistance, acute inflammation exercise done one or two repetitions |
| What Does Each DO: NSAID DMARDs CORTICOSTEROIDS BIOLOGICS | NSAID-reduces inflammation DMARD-Modify the course of disease Corticosteroids-quick acting antiinflammatory while waiting for NSAID and DMARD to take effect BIOLOGICS-subset of DMARDs work more quickly than DMARDs injected or given by infusion MAY Slow, Modify, or STOP the Disease |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
¿Quieres crear tus propias Fichas gratiscon GoConqr? Más información.