3768310
| Pregunta | Respuesta |
| Define Efficacy | How well an agonist evokes an active response. |
| Define Affinity | How well the drug binds to a receptor |
| Explain 'selectivity' | At a specific concentration a drug may primarily hit one target. However no drug only ever hits one target. |
| Drug Binding Equation | D + R >< DR Rate of association = K+1 (D)(R) Rate of dissociation = K-1 (DR) |
| Define Kd | Kd is the concentration of the drug that occupies 50% of the receptors. The lower the Kd the higher the affinity of the drug. |
| How do you can you calculate Kd using D and DR | Kd = (D)(R)/(DR) |
| What is Rt | Rt is the total no. receptors. Rt = (DR) + (R) Total no. receptors is equal to bound receptors + free receptors. |
| What does P stand for? How do you calculate P? | Fractional receptor occupancy P = (D)/(D) + Kd |
| What is the rearrangement of the fractional occupancy equation to give Kd? | Kd = ((D)/P) - (D) |
| Under which conditions is the receptor occupancy equation valid? | 1) Equilibrium 2) Drug conc. at receptor is the same as that applied to the system 3) One drug molecule combines with one receptor molecule 4) A negligible amount of the drug is added is added (otherwise the conc. would be altered) 5) Binding of one drug molecule does not influences the binding of the other (i.e. no cooperativity. |
| Why are semi-log plots more useful than linear? | 1) Rapid change in binding in proportion to (D), hard to plot and read accurately. 2) Hard to measure Kd off graph. 3) Ro is hard to reach on linear plot. |
| Which 2 parameters does the ability of an agonist to produce a pharmacological response depend on? | 1) Binding of drug to receptor (dependent on affinity) 2) Following binding, activation of the receptors and production of response (dependent on efficacy) |
| a (D) + (R) <> (DR) <> (DR*) B What determines how many bound receptors are in the activated state? | The higher the efficacy of the agonist the more drug receptor compounds that will be in the activated state. i.e. a high a and low B |
| What does E stand for? | E = intrinsic efficacy It refers to the ability of the drug to form (DR*) |
| What is Furchgott's equation for response? | Response = f E(Rt)(D)/(D) + Kd f=fudge factor and Rt are intrinsic to the tissue. The other components are drug-dependent |
| Define EC50 | EC50 = The concentration of the drug that evokes 50% of maximum response that drug can produce. |
| Why is the EC50 always lower than the KD? | EC50 is also dependent on efficacy, binding precedes response. Not all receptors have to be bound to produce a response because of efficacy. The greater the efficacy the greater the gap between Kd and EC50. The greater the efficacy the great the no. receptors left over. |
| What does Potency depend on? Why is potency useful? | Affinity, efficacy and receptor number. Potency can be used to compare drugs. The most potent drug is the most leftward. |
| In what three different scenarios can potency be used. | 1)Different drugs on same receptor 2) Different drugs on same receptor 3) Same drug on different tissues |
| If testing a drug on 4 different tissues what information could you tell? | As 1) binding will be the same as drug works on same receptor type and 2) Intrinsic efficacy should be the same so you should be able to deduce something about receptor number. |
| What does 'a' stand for? | a = intrinsic affinity |
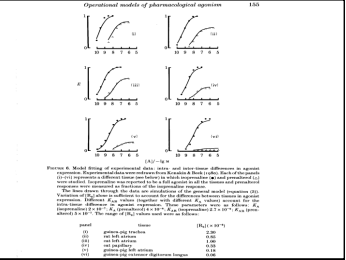
| Where will a partial agonist curve lie in compare to that of a full agonist in a concentration response curve? | The partial agonist will always lie to the right of the full agonist and except under certain substances, will have a suppressed maximum. |
| When can a partial agonist elicit a full response? | If there are enough receptors, however if you decreased the number of receptors the agonist would no longer produce a full response. |
| What is the therapeutic value of a partial agonist? Give an example. | There may be enough receptors in one tissue to elicit a full response and not enough in another. For example Salbutamol is a full agonist in the lungs (B2 receptors) but has little effect on the heart which has far less B2 receptors. |
| When might a full agonist not produce a full response? | If even though it has full efficacy, if there are not enough receptors a full response won't be produced. |
| Isoprenaline is a full non-selective B agonist. Prenaline is a partial agonist. Prenaline seems very effective in Trachea due to high receptor no. Rightward shift of Isoprenaline in last graph due to low receptor no. | |
| How does receptor number affect a partial agonist in comparison to a full? | The position of a full agonist depends on receptor no. A partial agonist graph is completely dependent on receptor no. |
| Name the four types of Antagonism. | 1) Competitive 2) Non-competitive 3)Uncompetitive 4)Physiological |
| Define Competitive antagonism. | The antagonist binds at the agonist recognition site preventing access of normal ligand. |
| Define Non-competitive antagonism. | Antagonist does not bind at the agonist site but inhibits agonist binding in another way |
| Define Uncompetitive binding | The binding of the antagonist occurs to an activated form of the receptor (use dependent e.g. Local Anaesthetic |
| Which type of antagonist can have efficacy? | Physiological |
| What is the Gaddum-Schild Equation and what can it be used for? | (D1)/(D1)' = 1 + (B)/Kb (D1)/(D1)' = Dose Ratio (B) = Concentration of antagonist Kb = Dissociation constant of antagonist The equation describes competitive antagonism. Allows you to find Kb and describe rightward shift of the graph. |
| How do you find Kb from the graph? | Kb is at Log(D) at which the Response = 50% |
| What is the equation for a Schild Plot. What must the slope be? | y = mx + c Log(CR-1) = Log(B) - Log(Kb) CR = Concentration Ratio The slope must be equal to one for the antagonist to be competitive. |
| What is pA2? What is it therefore equal to? | pA2 for an antagonist is the negative log of the molar concentration of antagonist which gives a dose ratio of 2. pA2 = -log(Kb) |
| Worked example: If a drug has a pA2 value of 9 what does this tell you about the drug? | At 1x10^-9 M the drug produces a dose ratio of 2. It is very potent. |
| For the next few flashcards describe the receptors that the drug acts on and the effect/use. Propanalol | B adrenoreceptors. Decreases heart rate (Antihypertensive). Now used for panic attack. |
| Haloperidol | D2 receptors. Antipsychotic, used to to treat schizophrenia |
| Atropine | Muscarinic Ach receptors. Causes dilated pupils and increased secretions. Used as a pre med. |
| Ranitidine | Histamine H2 receptors. Decreases gastric acid secretions. Used to treat gastric ulcers. |
| D-tubocurarine | Nicotonic Ach receptors. Neuromuscular block, used in major surgeries. Patients must be ventilated. |
| What is irreversible competitive antagonism? How does it look graphically? | The antagonist binds covalently, the graph will show a rightward shift and a decrease in maximum response. However max response may not decrease for the first few concentrations of antagonist if there are enough receptors. |
| How do non-competitive antagonists work? What is another term for non-competitive antagonists? | Either by allosteric modulation or by blocking some point of the downstream signalling chain between binding and response. Often called NEGATIVE ALLOSTERIC MODULATORS |
| Explain physiological antagonism. | One drug may antagonise another via action on an independent target. |
| For the next few flash cards explain what the agonist does and how the physiological antagonist prevents this. Noradrenaline/Acetylcholine | Noradrenaline increases HR and dilates pupils by acting on a adrenoreceptors. Acetylcholine acts on Muscarinic ACH receptors to decrease HR and constrict pupils. |
| Endothlin/Nitrates | Endothlin increases BP, Nitrates decrease BP. Act on different receptors. |
| Histamine/Salbutamol | Histamine acts on Histamine receptors to constrict the bronchioles. Salbutamol relaxes the bronchioles by acting on B2 receptors. |
| What is Constitutive Activity? | Constitutive activity is underlying activity in a tissue. Receptors can move between an active an inactive state with no agonist bound. |
| What can be used to reduce constitutive activity and how? | An inverse agonist. The inverse agonist binds to R* and inactivates it and stabilises receptors in inactive DR complex. DOES NOT BIND TO SAME SITE AS AGONIST. |
| How does an inverse agonist curve compare to that of an agonist? | The inverse agonist curve is a mirror image of the agonist curve from the baseline. The Maximum may be slightly less as the tissue may still be displaying some baseline activity. |
| What causes a tissue to become desensitised? | Over exposure to a drug, either i) Tissue in the presence of the drug for too long ii) Drug additions to tissue are too frequent. Causes changes to receptors, channels, coupling to G-proteins or second messengers |
| Which type of desensitisation is recoverable? | Tachyphylaxis |
| What is drug Tolerance? | Repeated administration of the drug may lead to adaptive down-regulation (internalisation) of receptors. |
| How can tolerance be used therapeutically? | Patients suffering with depression have low levels of 5-HT. SSRI blocks the uptake of 5-HT at nerve terminal, leading to a build up of 5-HT. Natural 5-HT stops being released, the autoreceptor (which prevents seretonin release) on the pre-synaptic terminal membrane is down-regulated. Decreased no. autoreceptors leads to increased seretonin levels. |
| List five properties of receptors. | 1) Present in very low concentrations in cell 2) Binding of ligand to receptor is normally reversible (Covalent v. rare) 3) Are Saturable 4) Clear Structure-Activity Relationships (SARS) 5) Only a small proportion of receptor protein is involved in binding of the drug. |
| Is selectivity greater for agonists or antagonist? | Agonists. |
| What is co-operativity in drug action? | The binding of one drug helps another at a (different) binding site. |
| How can you see co-operativity graphically? | The slope of the (Agonist) response curve becomes more steep. |
| What is the Hill equation? | P = (D)^n/(D)^n + Kd |
| What does 'n' stand for? | 'n' is the Hill coefficient, the greater the value the co-operativity. It has nothing to do the number of molecules binding. |
| What do values of 'n' <1< signify? | If 'n' is greater or less than 1 then usually there is more than one binding site. |
| What information do you plot a graph from a saturation binding experiment? | y-axis : bound drug (fmol/mg protein) x-axis : concentration (nM) Plot total, specific and non-specific binding (Specific = total - non) |
| What are the 5 advantages of radioligand binding? | 1) Specific measure of receptor-ligand interactions 2) Direct measure of receptor densities and affinities 3) Characterisation of binding of non-labelled drugs (e.g. is it competitive, can the non-labelled drug be displaced?) 4) Characterisation in absence of function response 5) Useful as probes during receptor purification and characterization |
| What is the half life (years) and specific activity (Ci/mA) of the following Isotopes? 3H | Beta, 28.8, 12.3 |
| 14C | Beta, 62.4, 5730 |
| 35S | Beta, 1494, 87.4 |
| 125 I | Gamma, 2176, 60 days |
| 32P | Beta, 9131, 14.3 days |
| What must be taken into consideration in radioligand binding experiments? | 1) The compound must bind with sufficient affinity and specificity 2) The compound must be of sufficiently high specific activity to detect few receptors 3)The radio half-life must be long enough to do the experiments 4) The compound should not be metabolised during the course of the experiments 5) Cost and safety |
| What are the 3 stages of radioligand binding? | 1) Incubate constant amount of receptor prep. with increasing amount of labelled ligand 2) Allow reaction to come to equilibrium R+L = RL* 3) Separate bound from free ligand and measure for bound reactivity. |
| What are the different methods for separating bound and free ligand for a) particulate fractions (cells,membranes) and b) Soluble receptors? | a) Filtration, centrifugation and dialysis b) Precipitation (Ethylene glycol), dialysis, adsorption (Charcoal) and centrifugation (high gmax) |
| What is the simplest model/equation for receptor-ligand binding? | (L*R) = (Ro)(L*)/Kd + (L*) Ro = Receptor Occupancy |
| What would you plot to find Kd, Ro and Bmax? | y = mx + c (L*R) = (L*) + Kd |
| What is the equation for Bmax? | Bmax = Ro/(Protein) (mg/ml) |
| How do you find non-specific binding of the radioligand? | Carry out a parallel assay in a high conc of unlabelled ligand is present. This saturates the specific binding sites and the radioligand now only binds to the non-specific sites (they are low affinity and non-saturable). |
| What relationship does non-specific binding have with radioligand concentration? | Approximately linear. |
| What are the equations for non-specific binding and total binding? | non-specific binding = k(L*) Total binding = (Ro)(L*)/(Kd + (L*)) + k(L*) |
| What is the equation for a radioligand scatchard plot | (L*R)/(L*) = (Ro)/Kd - 1/Kd(L*R) |
| How do you estimate non-specific binding? | Carry out parallel assay with high conc. of displacing ligand. All specific binding sites will be saturated by displacing ligand. Remaining radioactivity is due to non-specific binding. |
| Define IC50 | Concentration of competing ligand which displaces 50% of the radioligand |
| Define Ki | Dissociation constant measured using a competition binding study using a known radioligand |
| What do you plot to find IC50 in a competition assay? | (L*R) against Log(Inhibitor) |
| How do you find the IC50 graphically? | The IC50 is the point at which 50% of the L*R is bound |
| What equation can you use to find Ki in a competition binding assay? | Ki = IC50/(1 + (L)/KD) |
| What information do you get from a competition binding assay? | Information about the affinity of the displacing ligand |
| What are the advantages of a saturation assay? (6) | 1) Binding site densities 2) Ligand affinities 3) Binding site heterogeneity - existence of receptor sub types 4) Cooperativity of between binding sites 5) Pharmacological profiles of unlabelled agonists 6) Competitive vs. Non-competitive binding. |
| What are the disadvantages of saturation binding assays? | 1) Normally only high affinity binding may be measured 2) The equilibrium state is often not the functional state e.g a ligand gated ion channel, bound receptors are often desensitised. 3)No information is given on how the complex has reached the equilibrium state |
| INTRODUCTION TO ION CHANNEL PHARMACOLOGY LECTURE | NEIL MARRION |
| What four states can a Voltage-Gated channel exist in? | Closed/resting, open, inactivated,deactivated. |
| Define the refractory period | The time taken for the channel to go from the inactivated state to the closed state |
| What happens if you stimulate a cell during the refractory period? | Nothing - you can't generate an AP when the channel is in this state |
| If cations flow into a cell, what type of current will be observed? | A negative current. Graphically you would see a downward inflection |
| Using physiological concentrations what types of current will Na+ and K+ always generate? | Na+ --- Negative current K+ --- Positive current |
| What could yo use to block sodium channels? | TTX - Tetrodotoxin (from Japanese puffer fish) |
| Why does current through a channel reduce despite a constant voltage? | Inactivation of channels |
| How many subunits make up voltage-gated ion channels? | Four |
| Why does K+ channels only require 1/4 of the DNA required for Na+ and Ca2+ channels? | One long piece of DNA encodes the entirety of Na+ and Ca2+. For K+ channels, one gene codes for one subunit and those four subunits come together. |
| What are the 5 states a ligand-gated channel can exist in? | R>>LR>>LR*>>LRd>>Rd>>R |
| Where do you find nicotinic acetylcholine receptors? What do they require to activate? | 1) Muscle 2) Two molecules of Ach |
| How many subunits does a nicotinic acetylcholine receptor have? | Four |
| What are the subunits that make up a nicotinic acetylcholine receptor and how does this change at birth? | a1,a2, B and d Until birth y subunits were expressed, switched for d. d subunits transmit greater currents which allows for faster movements, thoughts etc. |
| How many transmembrane segments does a glutamate receptor have? | Three |
| How are voltage-gated channels classified? (4) | 1) Permeant ion 2) Physiological role 3) Or subtype 4) Gene |
| How are ligand-gated channels classified? (3) | 1) 'specific ligand' 2) lettering or numbering 3) 'receptor' |
| What are the two roles of ion channels? | 1) Trigger intracellular events 2) Bioelectricity |
| What 3 things can an increase in intracellular Ca2+ cause? | 1) Vesicle exocytosis 2) Protein kinase activation 3) Altered gene expression |
| Define membrane potential | Difference in charge across the membrane |
| What is Ohm's law? | V = IR |
| How do resistance (R) and conductance (G) relate to each other? | R= 1/G |
| What drives ions through ion channels? | 1) Concentrations gradient 2) Electrical gradient |
| What are the standard physiological concentrations of Na+, K+, Ca2+ and Cl- inside and outside of cells? (mM) | Ion Inside Outside Na+ 145 12 K+ 4 155 Ca2+ 1.5 100 nM Cl- 123 4 |
| What is the Nernst equation? | Eion = (RxT/Zxf) x ln(ion)out/(ion)in Z = Valancy, F = Faraday's constant (96500 C/M), R = Gas constant (8.31 J/K*M), T = Temperature |
| What constants can be used to replace RT/ZF? | 25*ln or 59*log10 Remember to account for charge of the ion e.g. Z of Ca2+ = 2 Therefore for Ca2+ 59/2*log10=RT/ZF |
| How does Eion affect the direction that ion will move in? | An ion will always move in the direction that will take the membrane potential in the direction of Eion. E.g. ENa is roughly +56.3mV, if the membrane is at -70mV the Na+ ions will try to move into the cell to make the membrane potential closer to it's own resting membrane potential. |
| What is the electrochemical gradient? | The gradient which an ion moves across. It depends on the difference in intracellular and extracellular charge as well as the concentration of the ion across the membrane. |
| Define 'equilibrium potential' | The point at which there is no net flow of current as the electrical gradient and chemical gradient are balanced against one another. |
| On a current x voltage graph, how do you find the equilibrium potential of the ion? | The equilibrium potential is the point at which current = 0 |
| When would a channel have an equilibrium potential that fitted no specific Eion? | If the channel was non-selective |
| Why is the equilibrium potential for nicotinic acetylcholine receptors slightly closer to the ENa+ than EK+? | As the channel shows a slight preference for Na+ |
| Why is the delayed opening of potassium channel important during action potentials? | If K+ channels opened simultaneously with Na+ channels there would be no action potential as opposing currents flow through these channels. Activation of K+ channels causes rapid repolarisation of the membrane. |
| What does 'G' stand for? | Conductance |
| What is 'G' the reciprocal of, and what is it represented by on which type of graph? | G is the reciprocal of R (resistance) As R = V/I, G is equal to the slope of an i/V curve. |
| What unit is conductance measured in? | Seinmens (S). Usually pico through a single channel. |
| How does positive feedback affect both K+ and Na+ channels respond to positive feedback? | Depolarisation leads to Na+ channels opening which leads to further depolarisation and so on. K+ channels stay at a constant percentage of open channels when the membrane is at rest. This is self regulated. |
| What causes EPSPs? | Non-specific cation channels. i.e. conductances with reversal potential potentials positive to the RMP. |
| What causes IPSPs | Conductances with reversal potentials negative to the RMP, e.g CL- and K+ (potassium will flow out of cell and chloride will flow in, both making the membrane more negative.) |
| Where do tetrododoxin (TTX), saxitoxin (STX) and Phenytonin act, and what are they used to treat? | Na Channel. TTX treats MS STX treats neuropathic pain Phenytonin treats epilepsy |
| Where do sulphonylureas (tolbutamide, glibencamide) act and what are they used to treat? | K+ Channel, treat diabetes |
| DRUG ACTION AT ION CHANNELS Dr. M. Usowicz lectures | Start |
| What are the 3 main benefits of the patch clamp technique? | High Resolution way to: 1) Investigate Ion channel properties 2)Follow in real time changes in activity of individual membrane proteins. 3) Investigate action of drugs on ion channels. |
| What are the benefits of applying light suction to a patch clamp pipette? | Tight seal between membrane and pipette leads to clearer and higher resolution recordings as background noise is removed and membrane is effectively isolated |
| What is the purpose of voltage clamping? | Allows you to record current through specific channel - current created through channel change the potential at the membrane as voltage is clamped and so no other voltage gated channels will be effected (and will not contribute to current recorded) |
| What are the three types of patch clamp configurations? | Whole-cell, inside-out, outside-out |
| To get an perforate whole-cell configuration what must be applied? | Antibiotics to perforate the cell, |
| What is the difference between how and outside-out and inside-out configuration are made? | More suction is applied before the membrane is excised in an outside-out configuration. |
| Where is the external membrane face in an a) outside-out configuration b)inside-out configuration | a) External membrane faces outwards b) Internal membrane faces inwards |
| Why does what you do to the patch of membrane have no effect on the rest of the cell in a whole-cell experiment? | Membrane/seal is electrically isolated (giga seal 1-100Gohms) |
| What information do you learn from single channel currents? How quickly do they open/close? | Whether the channel is open or closed. Less than 10 micro-seconds. |
| How can you determine if a cell is voltage gated? | Frequency of opening depends on voltage. Current varies with voltage in all types of channels due to changes in driving force. |
| What determines the size and direction of a single channel current? | Voltage gradient |
| What is the equation for voltage gradient? | Vg = Vm - reversal potential Where Vm is the clamped voltage and the reversal potential is the potential at which no current flows. |
| How do you identify the reversal potential? Why does this not mean that no channels are open? | The net current will be zero. Channels are open but current is flowing equally in both directions. |
| If the voltage gradient is negative what will positive ions do? And if the voltage gradient is positive? | Positive ions will flow into the cell, positive ions will flow out of the cell. |
| If the driving force/voltage gradient is negative what does this mean in terms of flow of ions and direction of current? | Positive ions will flow into the cell, inward flow of positive ions is a negative current, downward deflection. |
| How would you determine the nature of a voltage gated channel? | Determine the reversal potential of the channel (i=0) and see how this compares to the reversal potential of various ions (NERNST) |
| Why might a an IV graph not be linear? | If a channel is 'clogged'(think Magnesium block NMDA) |
| How can you determine if a channel is ligand gated? | No current will flow without the presence of the ligand. Frequency of opening will not vary with voltage. |
| TRUE/FALSE For a ligand-gated ion channel voltage affects: a) Probability of opening b) Single channel current c) Single channel conductance | a) False b) True c) False |
| What is the downfall of excised membrane patches? | Loss of intracellular cascades/responses which may affect response/current |
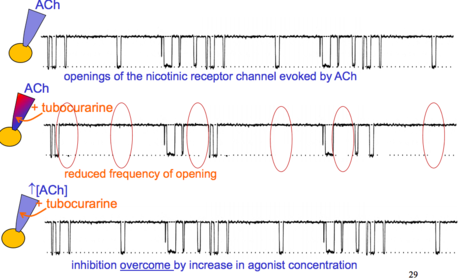
| What type of antagonist is this? | A competitive antagonist. Addition of the antagonist reduces the frequency of opening however with further addition of agonist the frequency of opening normalises. |
| Which antagonist might you use to block the effect of ACh? | Tubocurarine |
| Which antagonist could be used to block voltage gated sodium channels? | Tetrodotoxin (TTX) |
| How might you tell that TTX isn't use dependent on a single channel current recording from a voltage gated channel? | Inhibitory effect on frequency of opening doesn't vary with voltage. |
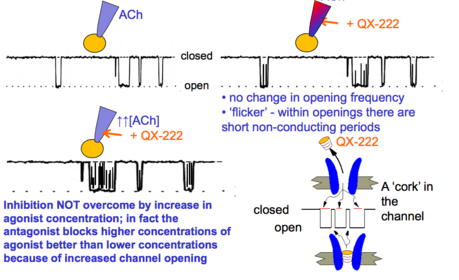
| What type of antagonist is this? | Un-competitive, open channel blocker. Flickers observed within openings which represent short periods of non conductance where the antagonist has bound to the open conformation of the channel. There is no current flow at this point and the current flicks back to zero. |
| What is QX-222? | Fast ion channel blocker. |
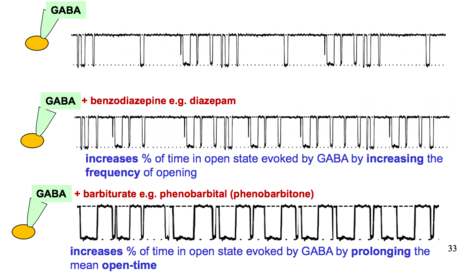
| What classification of substance is causing the effect on openings here? How are the effects different? | Allosteric Modulators 1) % time spent in open state increased by increasing frequency of openings 2) % time spent in open state increased by increasing time spent in open state. |
| PATCH CLAMP RECORDING LECTURES CONTINUED | START |
| What is the advantage of using a whole-cell recording? | Big current - easy to see effects of drugs. Current in scare of 10s of pA to nA |
| What is the disadvantage of a whole cell recording? | Contents of pipette dilute intracellular environment leading to a dampening of current over time |
| What then is the advantage of a perforated-patch whole-cell recording? | Antibiotic channels are impermeable to molecules larger than glucose, no loss of important molecules from intracellular environment. Therefore much slower 'run-down' currents. |
| Which antibiotics could you use to make a perforated-patch whole-cell configuration? (3) | Nystatin Amphotericin B Gramicidin |
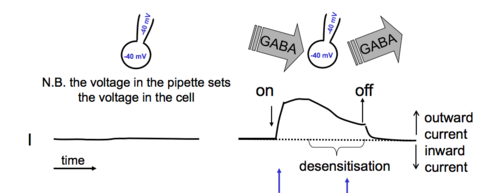
| What type of channel is this recording from? | Ligand-gated |
| Why does the current decrease in a whole-cell recording from a ligand gated channel despite no change in voltage or ligand conc? | Some of the channels become densitised |
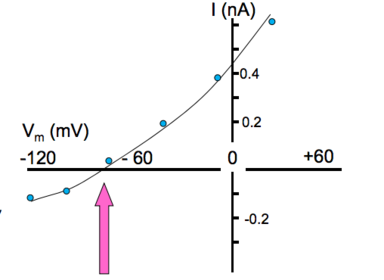
| What type of channel would produce this recording? | A ligand gated channel - specifically chlorine due to the reversal potential value |
| In which direction would chloride flow at 0V and what type of current would you have? | Chloride would flow IN to the cell, reversal potential of chloride is around -65mV, so Vg would be +65 (0-(-65). As chloride is a negative ion it behaves in an opposite way to a cat ion. The inwards flow of chloride produces a positive current. |
| What two drugs could you use to block Ca2+ and K+ currents in order to observe just a Na+ current? | K+ Cs+ applied internally TEA (tetreathylammonium) externally Ca2+ Cd2+ |
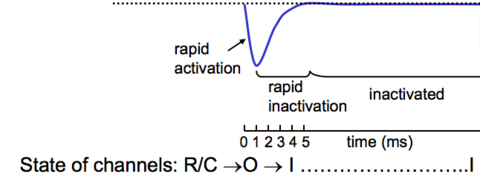
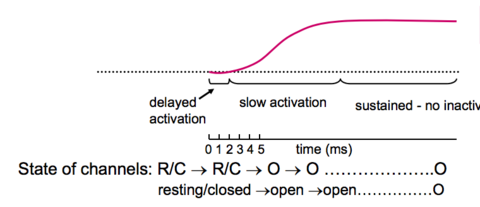
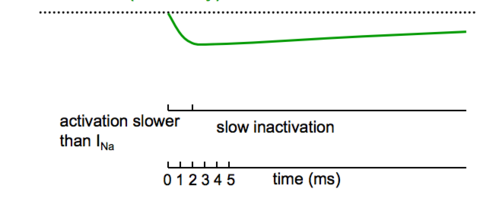
| For the next 3 slides identify the voltage gated channels responsible for the current recorded and explain their inactivation time. | START |
| Sodium channel, rapid inactivation due to desensitisation of channels. | |
| Potassium channel, do not become desensitised so no inactivation of channels. | |
| Calcium channel, slower to inactivate than sodium channels an show little inactivation. | |
| If a drug inhibits current through a voltage gated channel how would you tell if it was a voltage dependent drug or not? (2) | If the drug was not voltage dependent the reversal potential of the channel would not change in the presence of the drug. Percentage inhibition would remain constant throughout the range of voltages. |
| Why does the reversal potentials for current flowing through a Ca2+ channel occur at a more negative value than Eca? | At larger positive values (50+) the calcium channel becomes non-selective and allows small monovalent cations (k+ or cs+) to flow out of the cell. This is because their intracellular concentrations are much higher than that of Ca2+. Therefore there is an outward current before Ca2+ is flowing out of the cell. |
| Give an example of a voltage dependent drug. (Agonist at L-type channels) | S Bay K 644 |
| What is the relationship between micro and macroscopic currents? | A macroscopic current is the sum of microscopic currents through single channel recordings. |
| Describe graphically the relationship between ligand gated macro and micro currents. | The two graphs are the same linear shape, as frequency of opening depends on agonist concentration not voltage. |
| Why are I/V graphs of single channel and whole cell recordings different for voltage gated channels? | A whole cell recording is dependent on both probability of opening as well as driving force ('u' shape). |
| Describe why a whole cell voltage gated channel recording is 'U' shaped. | 1) Low Po, High driving force 2)Po increases 3)At max current DF starts to decrease, Po stays at max |
| VOLTAGE DEPENDENT CALCIUM CHANNELS MARIA USOWICZ 19/10/15 | START |
| What two roles do voltage-dependent CA channels have? | 1) Electrogenic (muscle contraction) 2) Regulatory (secretion etc) |
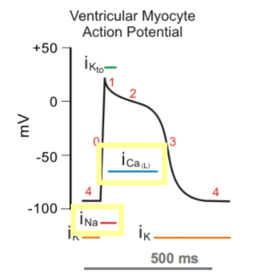
| Where would you expect to see this shape of current? | Ventricular Myocyte Action Potential Calcium current produces the 'bump' |
| Which currents are responsible for which parts of the overall shape? | 1)T-type Calcium channels are responsible for the current until threshold is reached. 2) L-Typer Calcium channels are responsible for the main AP |
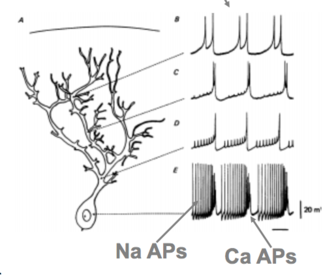
| What type of currents are shown here and in what type of cell? | 1)P-type calcium (slow) an Na (rapid fire) 2) Purkinje |
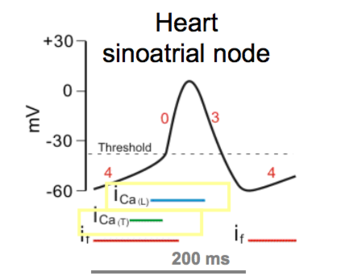
| Which type of calcium channel is low-voltage activated and where is it found? (Below ~-50mV) | 1)T-type 2) Neurons, heart (sinoatrial node), muscle |
| Which types of Ca channels are high-voltage activated (Above ~-50mV), and where are the found? | N,P,R-Type (neurons) L-type (neurons and muscles) P-type mediate the release of ACh from pre-synaptic terminals |
| What 3 classes of compounds act at L-type Ca channels? | 1) Phenylalkylamines 2) Benzothiazepines 3) 1,4-dihydropyridines (DHPs) (sensitivity defines L-type channels) |
| Give an example of a phenylalkamine? | Verapamil |
| What concentration of verapamil is required for 100% block? | 1uM |
| What are the clinical uses of Verapamil? What is an adverse affect? | 1)Treats supraventricular tachycardia (verapamil binds to overactive ca channels more than normal ca channels) 2) Treats hypertension 3) Adverse: Hypotension, inhibition of Ca channels in vascular smooth muscle |
| Give an example of an Benzothiazepine | Diltiazem |
| How do DHP (1,4 - dihydropyridines) antagonists work on L-type channels? | Bind and hold L-type channel in inactivated state, bind to extracellular side. |
| Why would you expect a DHP antagonist to cause greater % inhibition when opened from -50mV than -100mV (to 0mV) (2) | 1) DHP antagonists are voltage dependent 2) More channels are in inactive state (less available for opening) and -50mV than at -100mV |
| Why are DHP antagonists selective for vascular smooth muscle over cardiac? | Vascular smooth muscle is always slightly depolarised >>> more channels in inactivated state. |
| Which DHP antagonist is selective for cerebral arteries? | Nimodipine |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
¿Quieres crear tus propias Fichas gratiscon GoConqr? Más información.