
4224035
| Pregunta | Respuesta |
| What are the two sub categories of ACh receptors | Nicotonic (nAChR) Muscarinic (mAChR) |
| Where are mAChR found and how are they structured? | postganglionic parasympathetic synapses; brain |
| What are the two subtypes of nAChRs? | Muscarinic (NMJ) and Neuronal |
| Describe the structure of the NMJ nAChR | Pentameric. 2a subunits B, d, Y/E |
| What is the structure of neuronal nAChRs? | Pentameric. a2-10, B2-4 Usually 2(a3) 3(B4) |
| Where are neuronal nAChRs found in the PNS? | Ganglionic synapses, adrenal medulla, presynaptic receptors at NMJ |
| Where are neuronal nAChRs found in the CNS? | Neurones in brain and spinal cord |
| Where is the ligand binding site on the nAChR? | a1 or a2 |
| Are nAChRs selective? | No they allow Na+ to flow in and K+ to flow out |
| What roughly is the RMP for nAChR usually? | ~60mV |
| How do K+ and Na+ currents relate at rest through an nAChR? | Na+>>K+ |
| Define endplate potential? | Depolarisations of skeletal muscle fibres by the binding of neurotransmitters to the postsynaptic membrane in the NMJ |
| What are the precursors to acetylcholine? | Choline and Acetyl-CoA |
| Which enzyme synthesises Acetylcholine? | Choline acetyltransferase |
| Which enzyme breaks down acetylcholine | acetylcholinesterase |
| What percentage of acetate and choline are recaptured? | 50% |
| Which two drugs act presynaptically to prevent exocytosis? | Botulinum and Tetanus Toxin |
| Give an example of a non-depolarising blocker | Tubocurarine |
| What effect on end plate current does a non-depolarising blocker have? | End plate potential never reaches threshold for AP. |
| What would you expect to see with inhibition of neuromuscular transmission? | Flaccid Paralysis - muscle relaxation |
| What would be the expected order of muscle relaxation? | Eyes + small facial muscles Limbs Pharynx Respiratory Muscles |
| What effect to non-depolarising blockers have on pain perception and consciousness? | None. |
| What are the benefits of non-depolarising blockers? | Poor oral absorption (not taken across gut) Quickly excreted Don't cross the placenta |
| What is a common side effect in non-depolarising blockers? | Histamine release. |
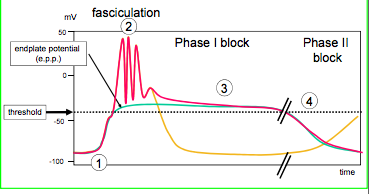
| Give an example of a depolarising blocker | Suxamethonium |
| Explain the four stages | 1) nAChR activated 2)Fasciculations - lots of impulses when agonist first applied 3)Phase 1 block - Na+ channels desensitise 4)Phase 2 block - nAChR desensitise |
| Why is the desensitisation of nAChR a slow process? | Secondary messengers |
| What are the four key differences in depolarising v. non-depolarinsing drugs? (fasciculations, post-op,reversibility) | 1) Depolarising drugs cause fasciculations 2) Depolarising drugs often cause post operative pain 3) Depolarising block, suxamethonium is hydrolysed by plasma cholinesterase 4)Non-depolarising block is reversible by anticholinesterase drugs. |
| What effect does prolonged presence of an anticholinesterase cause? | Build up of acetylcholine causes a depolarising block |
| What are the two sites on acetycholinesterases? | Esteric and anionic |
| Which part of the acetycholine molecule is attracted to which part of the acetycholinesterase? | Acetate (CH3COO) bonds to esteric site (Hydolysed to CH3COOH) Choline (With N+ binds to anionic site) |
| What are the main causes of myasenthia gravis? | 1) Genetic (mutation for nAChR receptor, or protein (rapsin) which takes nAChR to endplate) 2) Autoimmune disorder |
| What is the main underlying problem with myasthenia gravis | Too low number of nAChR receptors - less transmission leads to muscle weakness |
| What are the symptoms of myasthenia? | Drooping eyelids muscle weakness |
| How do you test for myasthenia gravis? | Give Edrophonium - restores muscle strength rapidly |
| What 3 anticholinesterases do you use to treat myasthenia gravis? Where do they act? | Neostigmine Physostigmine Pyridostigmine Act at NMJ |
| Which anticholinesterase would you give to reverse a non-depolarising block after surgery? | Neostigmine |
| Which two anticholinesterases can be used to treat alzheimers? | Donepezil and Rivastigimine (Can cross blood brain barrier) |
| Give an example of two organophosphates? Why are they so damaging to people? | Malathion Ecothiopate Depolarising block is irreversible |
| Why does myasthenia gravis cause a rightward shift in a concentration response curve for a given amount of endogenous agonist? | Loss of spare receptors |
| Why do medium lasting anticholinesterases last longer than short duration? | Bind more strongly to active site, hydrogen bond with serine from carbamyl, glut binds with N+ groups |
| Why is edrophonium short acting? | Weak nucleophilic bonds |
| Why are irreversible blocks irreversible? | Covalent bond at serine |
| What are the side effects of anticholinesterase intoxication at the: | Begin |
| Eye | Mitosis, blurred vision |
| Heart | Bradycardia |
| Lung | Bronchoconstriction |
| GI Tract | Vomiting, diarrhoea |
| Glands | Sweating/Salvation |
| NMJ | Convulsions, followed by flacid paralysis |
| CNS | Agitation followed by respiratory arrest |
| How can you reverse/help the effects of anticholinesterase poisoning? | Life support Atropine (muscarinic agonist) Cholinesterase reactivation (for iireversible anticholinesterase) |
| What drug can you use to combat the effects of irreversible anticholinesterases? | Pralidoxime, phosphate group/bond gets attracted to N+ group on pralidoxime. Unblocks acetylcholinesterase |
{kind=link}
0 comentarios
¿Quieres crear tus propias Fichas gratiscon GoConqr? Más información.