4234621
| Pregunta | Respuesta |
| Circadian Rhythms | biological rhythms that last "about a day" -diurnal: active during the day (light periods) -nocturnal: active during the night (dark periods) |
| Zeitgeber | -German: "Time giver" - cues from the environment used to entrain an animal's circadian rhythm -entrainment - the process of synchronizing one's biological rhythm too a cue in the environment |
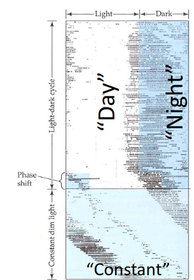
| Why do we stick to circadian rhythms? | to test the role that zeitgebers play in circadian rhythms, scientist studied the sleep and waking behaviors of hamsters in a laboratory setting where they could control them "day" and "night" -"day" - lights on -"night" - lights off -"constant" - constant dim lighting, absences of zeitgeists |
| Hamsters: nocturnal | active at night, inactive during the day, they're nocturnal |
| hamsters sleep: | when it appears to be day (lights on) and runs on the wheel it appears to be night (lights off) |
| Constant lighting: | the hamster still goes to sleep at roughly the same time, and wakes up at roughly the same time |
| Why do we stick to circadian rhythms? | -circadian behavior is influenced by light/dark, but not really -even in the absence of zeitgebers (in constant dim lighting), the circadian rhythm persists -to explain this phenomenon, we must look inside the brain |
| Circadian rhythms | - the brain has a biological clock the suprachiasmic nucleus (SCN) -the SCN releases the chemical that affect --lower body temperatures --lower blood pressures --digestion -the SCN does this with 24-hour periodicity |
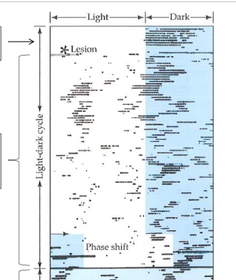
| What happens without the SCN? | intact hampster is active at night, inactive during the day. Even when "day" and "night" are not clear, the behavior is nearly circadian |
| Lesion of the SCN | causes less order to the hamster's circadian behavior |
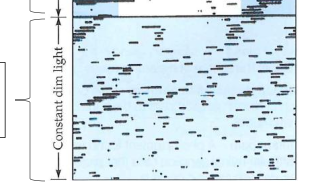
| SCN lesion & dim lighting | cause totally random circadian behavior |
| Why do we stick to circadian rhythms? interim review | -we stick to circadian rhythms because of external cues, known as zeitgebers -we also stick to circadian rhythms because of the activity of an internal biological clock, known as the SCN |
| the optic nerve | sends messages to the SCN to tell when its light or when its dark |
| Melanopsin | photopigment within certain retinal ganglion cells that project to SCN -melanopsin does not mediate vision, but tells whether its dark or light |
| Melanopsin | when it is light, melanopsin containing retinal ganglia inhibit hormone release by the SCN When it is dark, melanopsin containing retinal ganglia set off a chain reaction, ultimately causing the Pineal Gland to release a hormone called melatonin |
| Melanopsin - light | causes the inhibition of melatonin |
| Melanopsin : dark | causes release of mlatonin |
| Melatonin & circadian rhythm | -experts recommends "powering-down" electronic devices at night so that the SCN may appropriately signal the release of melatonin -how else might we "reset" the circadian rhythm --exogenous melatonin |
| exogenous melatonin - a sleep aid? | ability for melatonin to speed up the tie necessary for a person to fall asleep (in minutes gained) |
| Melatonin (relative to placebo) | -reduced sleep onset to latency by ~4 min. (compared to 15-20 min, normally) -increased sleep "efficacy" (more time sleeping, while in bed) and duratior sleeping longer ~13 |
| insomnia | -clinically defined as 30+ minutes latency to falling asleep, a difference of 4+ minutes could be mean a difference in clinical diagnosis |
| melatonin | -does not come with adverse side-effects of other commonly used substances to help sleep (e.g. bonzos, alcohol) |
| EEG | electroencephalogram - enables researches to observe the brain's behavior, even without the participant having to be awake |
| REM | rapid eye movement -four distinct stages of sleep -awakefulness |
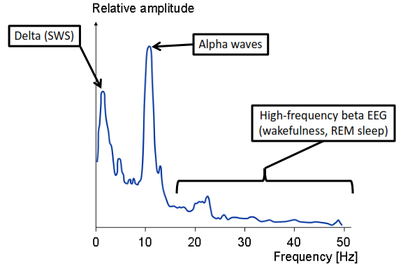
| Spetogram of EEG | |
| What is sleep? | ? |
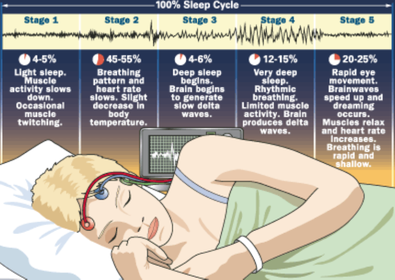
| Awake/alert | Fast (13-30Hz, beta), low amplitude EEG wave |
| Eyes closed, relaxed | Slower (8-13 Hz, alpha) higher amplitude EEG waves |
| Stage 1 | Even slower (4-8 Hz, theta) low amplitude EEG waves |
| Stage 2 | EEG looks like a stage 1, punctuated by K-complexes and sleep spindles |
| Stages 3&4 | slow-waves sleep (SWS) is characterized by predominately high-amplitude delta (1-4Hz) rhythms |
| REM sleep | occurs during "emergent" stage 1 sleep and is characterized by rapid eye movements (REM) -stages 1-4 without REM are called non-REM, NREM -the EEG during REM sleep looks like |
| Stage 2: K-complexes reflect neuronal "down-states" | Neurons like to have resting postsynaptic potentials (PSPs) that are either "up" (slightly depolarized, ready for action potentials) or "down" (slightly hyperpolarized, silent and not ready to fire an action potential) |
| cortical neurons "down-states" | less receptive to inputs from the thalamus. Down state inhibits sensory input/arousal |
| K-complexes in stage 2 lead to theta and delta waves in slow-wave sleep (SWS) in stages 3 & 4 | When cortical neurons are in "down-states", they are less receptive to input from the thalamus. - |
| Sleep Cycle | |
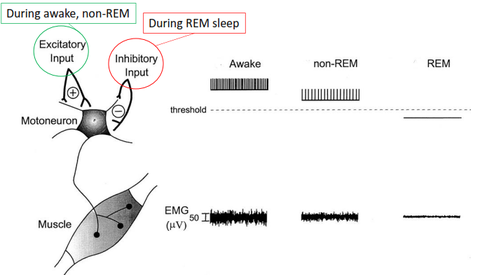
| REM sleep looks like wakefulness | "paradoxical sleep" because EEG looks like wakefulness -Brain EEG and eye EOG activity of awake person and REM sleeper looks almost identical -Muscle EMG activity of REM sleeper is almost absent; REM sleep is paralyzed |
| Motor neurons are inhibited during REM | |
| REM sleep looks like wakefulness | -lab rats kept from REM sleep will die in a matter of weeks -Human kept from REM sleep (e.g. for a few nights) tend to show REM rebound --the increased amount of REM sleep experienced after it has been missed for several nights |
| REM sleep & dreaming | -dreaming is limited to REM sleep, although it is when most (80%) dreaming takes place --REM dreams: emotional, illogical, sudden shifts in plots --non-REM dreams : shorter, commonplace themes Persons woken up from REM often recall dreams; less often if woken up during non-REM --the amount of time spent in REM correlates with how long a person thinks he/she has been dreaming -external stimuli (eg water droplets in face) presented during REM can be incorporated into one's dreams |
| Broad categories of sleep disorders | -insomnia (lack of sleep) -hypersomnia (too much of sleep) |
| insomnia | most common form of sleep disturbance -20 min+ to fall asleep -waking to early -not being able to fall back asleep if woken in middle of the night -insomnia is often linked to stress, relationship problems, medication, illness, working late or variable shifts, jet lag, drinking caffeine, excessive napping |
| Insomnia (lack of sleep) | pharmacological treatments -melatonin (endogenously secreted available over counter) -depressant drugs --benzodiazepines (Valium, Xanax) --non-benzos (e.g. ambien) --alcohol |
| Most sleep-aide drugs come with chance of dependency | -individuals that use depressant drugs may need that drug in order to fall asleep -withdrawal from these drugs includes anxiety, irritability, restlessness, and may actually cause insomnia |
| Hypersomnia (too much sleep) | Narcolepsy -frequent 5-10 minute extreme seep attacks occur every 90 minutes -cataplexy - sudden loss of muscle tone (despite being fully conscious) -skeeter! The narcaleptic pup -dysfunction of the neuropeptide orexin seems to influence narcolepsy |
| orexin neurons in the hypothalamus serve as sleep/wake "switch" | -orexin neurons projects to other sleep-related brain regions -symptoms of narcalepsy often co-occur with degeneration of hypothalamic orexin neurons --orexin keeps sleep "at bay" prevents rapids progression from wakefulness to REM sleep |
| Narcolepsy treatment | may be treated with stimulant drug (e.g. amphetamines) caffeine, or modafinil (Provigil) |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
¿Quieres crear tus propias Fichas gratiscon GoConqr? Más información.