5156433
| Pregunta | Respuesta |
| What are the three main damaging consequences of thrombosis? | 1) Tissue ischaemia 2) Infarction 3) Embolism |
| What are the two non-harmful consequences of a thrombus? | 1) Dissolves - either naturally or with treatment (heparin). Effectiveness is dependent on time 2) Recanalization/reorganisation - endothelial cells line thrombus and vascular cavities form through thrombus reestablishing some blood flow. |
| What is an embolus? | Intravascular solid, liquid or gaseous mass which is carried by the blood from its point of origin |
| How do emboli cause damage? | Come into contact with vessel which is too small - occlusion. |
| What % of events are thromboembolic? Of these what % originate from the venous circulation? | 1) 99% 2) 95% - predominantly deep vein of the pelvis or lower extremity. |
| How do superficial thrombi present? | Dark blue, oedema, painful and skin ulceration. |
| What % of deep vein thrombosis are silent? | 50% have no clinical presentation. |
| What is a thromboembolism? Where do the majority of them travel to? | Chunk of thrombus breaks off. Towards the lung (as most originate from venous circulation) |
| What is PE? Who is at high risk for this? | 1) Pulmonary embolism. 2) People who have a lot of bed rest - ie following surgery |
| Why is surgery a risk factor for embolism? | 1) Increased amount of coagulation factors 2) Increased relative platelet concentration due to dehydration 3) Having to be immobilised - muscle contraction helps to keep blood moving etc |
| What is and what would DVT cause systemically and locally? | 1) Deep vein thrombosis 2) Could cause occlusion/ischaemia - locally causes congestion and swelling. |
| How many deaths per year are due to DVT? | 25K deaths |
| Where do the majority of DVT travel to? | Heart then lungs |
| What are the effects of DVT embolism? | 1) If small enough resolved at site ie through recanalization 2) Pulmonary hypertension in the lung even if only small caliber vessel occluded 3) Lung hemorrhage is medium caliber occluded. |
| What increases the risk of DVT embolism having a thrombotic event? | If it is the second thromboembolism form the DVT even if the first was asymptomatic/resolved resulting in pulmonary hypertension. |
| What % occlusion of circulation to the lung results in death? | 60% |
| When would a patient particularly have to be observed after surgery? (2) | 1) Tachypnea - increased rate of respiration 2) Confusion/dizziness |
| Without prophylaxis what % of people having hip surgery have DVT?PE? Knee? | 1) 45% 2) 60% |
| How does deep vein thrombosis present? How common/rare are these presentations? | 1) Unilateral pain - common 2) Swelling - common 3) Tenderness - common 4) Discolouration - common 5) Dilated superficial veins - uncommon 6) Venous gangrene - Rare |
| How does the size of the clot relate to symptoms? | It doesn't |
| Why is venous gangrene rare? | Deep veins are part of a system, if one specific vein is occluded there may a collateral which can function as a bypass. |
| Describe the movement of a deep vein thrombus (in a pulmonary thromboembolism). | Deep vein - femoral vein - inferior vena cava - RHS atria heart - RHS ventricular outflow - pulmonary artery - lung occlusion. |
| What do pulmonary thromboembolism look like? | Very long - up to 30cm long. If that size it will completely occlude the circulation through the lungs and bring the entire circulation to a halt. |
| Other than from deep veins what other parts of circulation might thromboembolism result from? | From the heart (intracardiac thrombi) or thrombotic material from arteries. From heart embolism/thrombotic material could travel anywhere. |
| What else can cause a thromboembolism? Where causes this? | Air or gas enters the circulation: 1) Medical mishap (eg laparoscopy, poorly managed vascular cannulae) 2) Many small bubbles from scuba diving 3) Many small bubbles in Caisson disease 4) Fat emboli 5) Embryonic emboli |
| What is the main problem which result from arterial thrombi? | Can be embolic but main issue is the local occlusion. |
| What is a laparoscopy? | Laparoscope and grasper inserted into small gap into abdominal cavity. To see organs inflate a small amount of air - that air could enter blood vessel. |
| What do air/gas embolisms result in? | Large mass of air if transported to the heart leads to sudden absence of the blood in the contracting ventricle leads to loss of normal contractile rhythm and acute heart failure. |
| What is Caisson disease? | Caissons are underwater containers where people work on construction. Gas arises in circulation as the result of decompression sickness. The increases levels of pressure result in increased quantities of nitrogen dissolved in the blood and tissue. If you don't resurface gradually then gas can form air bubbles in blood and spread through circulation. Same as in scuba divers. |
| What does Caisson disease cause? | Multifocal occlusion of different blood vessels |
| What are the signs of decompression sickness? | 1) Acute - pain in muscles and joints 2) Chronic - ischaemic necrosis in both the bone and brain. Manifestations may be delayed many years after the initial injury. |
| What causes a fat embolus? | Fracture/injury results in bone marrow breaking off and entering the circulation. |
| What is bone marrow made of? What properties does it have? | Bone marrow is made of haematopoietic cells and adipose tissue. Strong thrombogenic capacity - activate the coagulation cascade. |
| What usually happens to a fat embolism? What happens if it doesn't? | Fat is metabolised in the pulmonary circulation. If this doesn't happen globular fat passes into the systemic circulation. |
| What/why/where do fat embolisms cause damage? | Impact cerebral vessels causing ischaemic necrosis. Occlude them mechanically and by activating coagulation cascade. |
| What percentage of patients following major fractures don't have fat embolisms? What percentage appear symptomatic? What percentage have severe manifestations, what causes this? | 1) 95% 2) 10% 3) Very small amount - due to diffuse thrombocytopenia. Presents with breathing issues. |
| What is the most severe consequence of a fat embolus? | Multiple petechial hemorrhages (very small and spread throughout brain) within the white matter - cerebral edema and herniation may follow. |
| In the US where does amniotic fluid embolisms rank in terms of deaths in the late stages of pregnancy? | 4th |
| What is the normal order of birth? How is this disrupted to cause amniotic fluid embolisms? | 1) Labour starts with rupture of amniotic sac - release amniotic fluid followed by delivery of the baby and then the placenta. 2) With precipitate labour the rupture of the amniotic sac may occur simultaneously with the delivery of the baby - placenta separates from uterine wall. This exposes uterine vessels allowing amniotic fluid to enter maternal circulation during contraction |
| What is amniotic fluid rich in? What effect does amniotic fluid have in the maternal circulation? | 1) Thromboplastin (prothrombotic) and fetal components (cells, lanugo, vernix and keratin lamellae) 2) Promotes immune reaction and activates coagulation cascade leading to DISSEMINATED INTRAVASCULAR COAGULATION. |
| What is disseminated intravascular coagulation? What two things does this call? | Multifocal activation of the coagulation cascade - massive consumption of coagulation factors so dispersed clotting and huge amounts of bleeding at the same time - can result in death of the mother. |
| Which coagulation pathway would the amniotic fluid activate? | The extrinsic pathway by releasing TF (tissue factor - thromboplastin) |
| X | |
| X | |
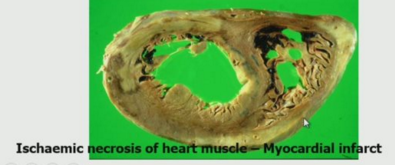
| What is the localised damaging consequence of thrombosis? | Infarction - infarct is a localised area of tissue necrosis resulting from sudden reduction of either its arterial supply or its venous drainage. DECREASED PERFUSION. |
| Brown colour as fixed in formalin - dark areas indicate hemorrhage. Coronary artery may have had a thrombus. Lumen may have been occluded by more than 60% so associated area of heart has died. That area of heart can no longer pump blood. Endocardium is also damaged and result in thombi. | |
| Describe the stages of myocardial infarction. | 1) Intravascular thrombus 2) Localised infarction 3) Endocardial damage 4) Intracardiac thrombi which can spread as embolisms |
| What are the general factors which mediate the response of a tissue to a reduction in blood flow? | 1) Blood supply 2) Rate of development of ischaemia 3) Tissue vulnerability 4) Individuals genetic predisposition/enhancements. (General status of the organism) |
| Give examples of the general state of an organism which may cause an exacerbated response by the tissue to oxygen deprivation | Reduced oxygen carrying capacity: Anaemia Hypoxaemia Cardiac disease Lung disease |
| Which organs have double circulation? Why? How does this affect the likelihood of a massive infarction? | Lung and liver - To perform their own function and to perfuse/filter blood. Decreases - very rare. Also in arm (two major arteries) |
| Which organs have parallel circulation? | Brain and arm |
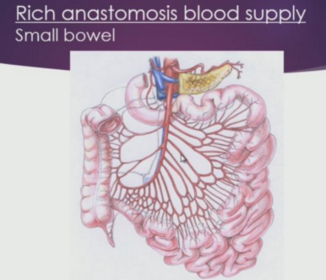
| Which organ has rich anastomosis? | Small bowel |
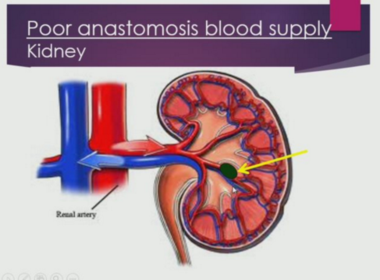
| Which organ has poor anastomosis? | Kidney |
| What is an anastomosis? How does this affect the risk of infarction? | Network of blood vessels. Unless main vessel is completely blocked, risk of infarction decreases - many alternative vessels to bypass occluded vessel and ensure that organ is perfused. |
| X | |
| What is the benefit of parallel circulation? | Other branches can provide blood if one is occluded. |
| Even if one of the more peripheral vessels is occluded the tissue is still like to infarct. | |
| How does the rate of occlusion development/ischaemia affect amount of infarction? | If occlusion is slow then it gives anastomotic blood supply to develop. |
| Give an example of a tissue which is resistant to ischaemia. Why is this the case? | 1) Cartilage 2) No blood vessels directly to cartilage - perfused by adjacent articular space/subchondral vessels |
| TISSUE VULNERABILITY How long can neurons/glia survive without oxygen? | 4 minutes |
| How long can heart muscle/kidney tubules go without oxygen? | 20-30 minutes |
| How long can connective tissue go without oxygen? | 100 minutes |
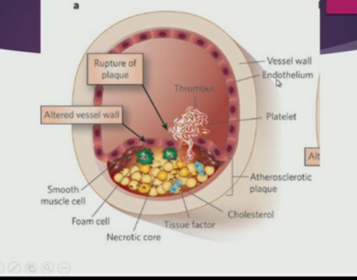
| What is an important factor in ischaemia and infarction? | Athersclerosis |
| Define atherosclerosis | A disease of the arterial lining intima in which there is an accumulation of lipid debris with an associated inflammatory reaction |
| How long does the process of atherosclerosis take? | Develops very slowly - over a period of 30-40 years, progressive occlusion of arterial vessels. |
| Describe the structure of an artery | Endothelium - basement membrane - tunica intima - tunica media - tunica adventitia |
| What are the components of the tunica intima? | 1) Lamina propria - smooth muscle and connective tissue 2) Internal elastic membrane. |
| What are the components of the tunica media? | 1) Smooth muscle 2) External elastic membrane |
| When does the damage of atherosclerosis occur? | Tunica intima (underneath the endothelium) |
| X | |
| What is found to accumulate in the tunica intima? Where? | Low density lipoprotein - in the subendothelial space. |
| What causes LDL to recruit inflammatory cells? What does this result in? | 1) If they are oxidized 2) Macrophages etc accumulate in the subendothelial layer. They can grow, activate and become necrotic. Inflammatory reactions. Also recruits fibroblasts - produces connective tissues. |
| All in all how does atherosclerosis occur? | Accumulation of oxidized LDL, macrophages and connective tissue - deforms vessel wall (plaque) |
| What happens if the plaque is stable? Unstable? | 1) Progressive slow occlusion vessel 2) May break through surface triggering thrombosis. |
| X | |
| What are the consequences of a complicated fibrous plaques? | 1) If sudden increase in size tissue may infarct (slow gives a change for anastomosis) 2) Surface thrombosis due to exposure/loss of endothelial cells - may lead to embolism or be incorporated into the plaque making it larger. 3) Intraplaque hemorrhage - causes sudden increase in plaque size. |
| Why do intraplaque hemorrhages arise? | Rupture of new vessels in the base of the plaque which originate in the inflammatory response to the free fat of the plaque. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
¿Quieres crear tus propias Fichas gratiscon GoConqr? Más información.