6612835
Descripción
Fichas por Andrew Street, actualizado hace más de 1 año
|
|
Creado por Andrew Street
hace alrededor de 8 años
|
|
| Pregunta | Respuesta |
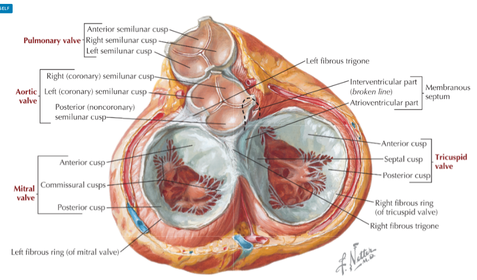
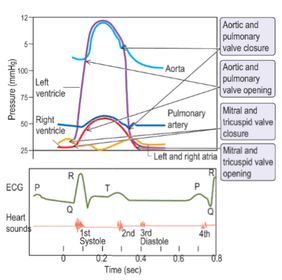
| 1074 Explain the cardiac cycle & describe how each valve opens & shuts during this cycle. | |
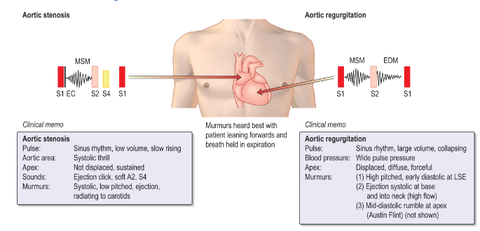
| 1076, 1078, 1081 Describe murmurs associated with aortic stenosis & regurgitation. | |
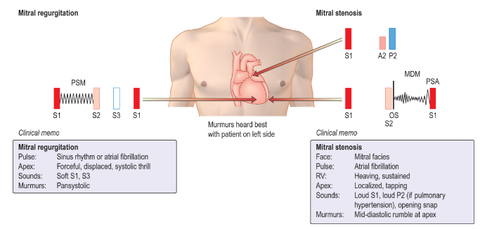
| 1076, 1078, 1081 Describe murmurs associated with mitral stenosis & regurgitation. | |
| List S & Sx of aortic stenosis. | Usually there are no Sx until aorta is a 1/3 of its normal size. * CP * Breathlessness * Syncope & pre-syncope * Fatigue. K & C p746. |
| List causes of aortic stenosis. | * Calcific stenosis of a trileaflet aortic valve - the commonest cause of aortic stenosis and mainly occurs in the elderly * Stenosis of a congenitally bicuspid valve (occurs in 1-2% of live births) * Rheumatic aortic stenosis - aortic valve is affected in 30-40% of cases * Other causes - CKD, Paget’s DS of bone, previous radiation exposure, homozygous familial hypercholesterolaemia. K & C p746. |
| Ix of aortic stenosis. | * CXR usually reveals a relatively small HT with a prominent, dilated, ascending aorta. This occurs because turbulent blood flow above the stenosed aortic valve produces so-called ‘post-stenotic dilatation’. The aortic valve may be calcified. The CTR ^ when HF occurs. * ECG - shows LVH & L atrial delay. A LV ‘strain’ pattern due to ‘pressure overload’ (depressed ST segments and T wave inversion in leads orientated towards the LV, i.e. leads I, AVL, V5 and V6) is common when the DS is severe. Usually, sinus rhythm is present, but ventricular arrhythmias may be recorded. * Echocardiograph - readily demonstrates the thickened, calcified and immobile aortic valve cusps, the presence of LVH, & can be used to determine the severity of aortic stenosis. TOE - rarely indicated. * Cardiac catheterization - rarely necessary since all of this information can be gained non-invasively. * Coronary angiography is necessary before recommending surgery. * CMR & CT - indicated for assessing the thoracic aorta for aneurysm, dissection or coarctation - rarely necessary. K & C p747. |
| Rx of aortic stenosis. | Sx are a good index of severity & *all symptomatic pt's should have aortic valve replacement*. Patients with a BAV and ascending aorta >50 mm or expanding at >5 mm/year should be considered for surgical intervention. Asymptomatic pt's should be under regular review for assessment of Sx & echocardiography. Surgical intervention for asymptomatic people with severe aortic stenosis is recommended in those with: Sx during an exercise test or with a drop in BP A LV ejection fraction of <50% Moderate–severe stenosis undergoing CABG, surgery of the ascending aorta or other cardiac valve.. Critical aortic stenosis in childhood or adolescence can be treated by valvotomy - provides temporary relief before valve needs replacement. K & C p747. |
| S & Sx of aortic regurgitation. | Significant Sx occur late & do not develop until LVF occurs. As with mitral regurgitation, a common Sx is *pounding of the HT* because of the ^LV size & its vigorous pulsation. Angina pectoris is a frequent complaint. Varying grades of dyspnoea occur depending on the extent of LV dilatation & dysfunction. Signs The signs of aortic regurgitation are many & are due to the hyperdynamic circulation, reflux of BD into the LV & the ^LV size. The apex beat is displaced laterally and downwards & is forceful in quality. The pulse is bounding or collapsing. Other signs such as De Musset’s & 'pistol shot' femorals are rare. K & C p748. |
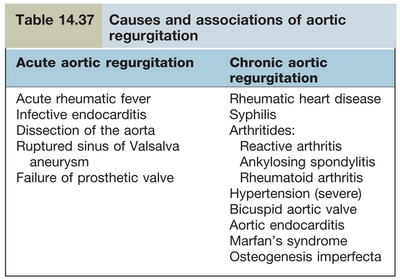
| Causes of aortic reguritation. | |
| Ix of aortic regurgitaion. | * CXR - features are those of LV enlargement & possibly of dilatation of the ascending aorta. The ascending aortic wall may be calcified in syphilis, & the aortic valve calcified if valvular DS is responsible for the regurgitation. * ECG - appearances are those of LVH due to ‘volume overload’ – tall R waves & deeply inverted T waves in the L sided chest leads, & deep S waves in the R sided leads. Normally, sinus rhythm is present. * Echocardiogram - demonstrates vigorous cardiac contraction & dilated LV. The aortic root may be enlarged. Diastolic fluttering of the mitral leaflets or septum occurs in severe aortic regurgitation. TOE may provide additional information about the valves & aortic root. * Cardiac catheterization - required to assess for CAD in pt's requiring surgery. Cardiac magnetic resonance and cardiac CMR and cardiac CT - may be indicated for assessing the thoracic aorta in cases of aortic dilatation or dissection. Cardiac MR can be used to quantify regurgitant volume. K & C p |
| Rx of aortic regurgitation. | * Rx underlying cause of aortic regurgitation e.g. syphilitic aortitis or infective endocarditis * Pt's with acute aortic regurgitation may require Rx with vasodilators & inotropes. * ACEi - useful in pt's with LV dysfunction * Beta-blockers - may slow aortic dilatation in Marfan pt's. Because Sx do not develop until the myocardium fails & because the myocardium does not recover fully after surgery, operative valve replacement may be performed before significant Sx occur. Aortic surgery is indicated in: * Acute severe aortic regurgitation e.g. endocarditis * Symptomatic pt's with chronic severe aortic regurgitation * Asymptomatic with LVEF ≤50% * Symptomatic with LVEF >50% but with a dilated LV (end-diastolic dimension >70 mm or systolic dimension >50 mm) * Undergoing CABG, surgery of ascending aorta or other cardiac valve. * Mechanical prostheses & tissue valves are used. Tissue valves are preferred in the elderly & when anticoagulants are CI, but are CI in children/young adults due to rapid calcification & degeneration. K & C p749. |
| S & Sx of mitral stenosis. | Sx Usually no Sx until valve orifice is moderately stenosed (i.e. has an area of 2 cm2). Because of pulmonary venous HT & recurrent bronchitis, progressively severe *dyspnoea* develops. A *cough productive of blood-tinged, frothy sputum or frank haemoptysis* may occur. The development of pulmonary HT eventually leads to *RHF* & its Sx of weakness, fatigue & abdo or lower limb swelling. The large L atrium favours *AF*, giving rise to Sx such as *palpitations* & ^risk of stroke, & mesenteric, renal and peripheral emboli. Signs * Mitral facies or malar flush. - bilateral, cyanotic or dusky pink discoloration over the upper cheeks due to arteriovenous anastomoses & vascular stasis. * Pulse - small-volume pulse which is usually regular initially, however, as DS progresses, many patients develop AF. * Raised JVP if RHF has developed. * Auscultation - opening snap followed by low-pitched ‘rumbling’ mid-diastolic murmur. K & C p741. |
| Causes of mitral stenosis. | * Rheumatic HT DS secondary to previous rheumatic fever due to infxn with group A β-hemolytic streptococcus. Inflammation leads to commissural fusion and a reduction in mitral valve orifice area. Over many years the condition progresses to valve thickening, cusp fusion, calcium deposition, a severely stenotic valve orifice & progressive immobility of the valve cusps. Other causes include: * Lutembacher’s syndrome - combination of acquired mitral stenosis & an atrial septal defect * Congenital mitral stenosis (rare) * In the elderly, a syndrome similar to mitral stenosis, which develops because of calcification and fibrosis of the valve, valve ring & chordae tendineae * Carcinoid tumours metastasizing to the lung, or primary bronchial carcinoid. |
| Ix of mitral stenosis. | * CXR - usually shows a generally small HT with enlarged L atrium. Pulmonary venous HT is usually also present. Late in DS a calcified mitral valve may be seen on a penetrated or lateral view. Signs of pulmonary oedema or pulmonary HT may be apparent when the DS is severe. * ECG - may show a bifid P wave owing to delayed L atrial activation. However, AF is frequently present. As the DS progresses, the ECG features of RVH (right axis deviation and perhaps tall R waves in lead V1) may develop. * Transthoracic echocardiography should be used to determine L & R atrial & ventricular size & function. * TOE - performed to detect presence of L atrial thrombus or prior to consideration of surgical or percutaneous intervention. * CMR - can accurately show mitral valve anatomy although it is rarely used in mitral stenosis. * Cardiac catheterization - seldom required & is only used if co-existing cardiac problems (e.g. mitral regurgitation or CAD) are suspected. R HT catheterization may be required to determine pulmonary artery pressure in pts referred for valve intervention. K & C p742. |
| Rx of mitral stenosis. | Mild mitral stenosis often no Rx except: * Prompt Rx of bronchitis * Mild dyspnoea - Rx with diuretics * Onset of AF - digoxin & anticoagulation If pulmonary HT develops or Sx of pulmonary congestion persist -> surgery. 4 types: 1) Trans-septal ballon valvotomy - ballon is passed into L atria and splits the commissures 2) Closed valvotomy - fused cups are forced apart by a dilator passed through the apex of the LV 3) Open valvotomy 4) Mitral valve replacement - indicated if regurgitation is present, badly diseased/calcific valve, moderate or severe mitral stenosis & thrombus in the L atrium despite anticogulation. K & C p743. |
| S & Sx of mitral regurgitation. | Can be present for many years before Sx occur: * Palpitations - due to ^stroke volume * Dyspnoea & orthopnoea - due to pulmonary HT * Fatigue & lethargy - due to reduced CO * Sx of RHF in late stage Signs: |
| Causes of mitral regurgitation. | Mitral regurgitation can occur due to abnormalities of the valve leaflets, annulus, cchordae tendinae or papillary muscles, or LV. This can be caused by: * Degenerative DS (myxomatous - 'a pathological weakening of connective tissue.' Wiki) * IHD * Rheumatic HT DS * Infectious endocarditis * Dilated & hypertrophic cardiomyopathy * Rheumatic AI DS - eg SLE * Collagen DS - eg Marfan's & Ehlers-Danlos syndrome * Drugs - centrally acting appetite suppressants & dopamine agonists. K & C p743. |
| Ix of mitral regurgitation. | * CXR - may show L atrial & LV enlargement, ^CTR, & valve calcification * ECG - bifid P waves, LVH (50% of pt's), AF may be present * Echocardiogram - dilated L atrium & LV, chordal or papillary muscle rupture features may be seen, TOE may be helpful before/during surgery * Cardiac catheterization - changes in atrial systolic pressures can be seen & contrast regurgitating back into the L atrium. K & C p745. |
| Rx/Mx of mitral regurgitation. | * Mild DS without Sx -> serial echocardiograms * If evidence of cardiac enlargement -> early surgical intervention with valve repair or replacement * If surgery is innaproriate/or to be performed at a later date -> ACEi, diuretics, possibly anticoagulants. K & C 745. |
| S & Sx of tricuspid regurgitation. | * Sx of RHF due to ^R atrial & systemic venous pressures - SOB, swelling of feet & ankles, nocturia, ^JVP, palpitations, fatigue, weakness, fainting * Large jugular 'cv' wave * Palpable liver that pulsates in systole * Blowing, pansystolic murmur * AF is common * Echo shows dilatation of the RV with thickening of the valve. K & C p750. |
| Causes of tricuspid regurgitation. | Functional tricuspid regurgitation may occur when the RV dilates: * Cor pulmonale * MI * Pulmonary HT Organic tricuspid regurgitation may occur with: * Rheumatic HT DS * IE * Carcinoid syndrome * Congenital abnormalities. K & C p750. |
| Rx of tricuspid regurgitation. | * Functional tricuspid regurgitation usually resolves with medical Mx * Severe organic tricuspid regurgitation - surgical repair may be neccessary * Valve replacement - rare. Prosthetic valve occasionally used for IVDU with IE. K & C p750. |
| S & Sx of pulmonary stenosis. | * Sx of RHF (see previous card) - due to obstruction of RV emptying which leads to R atrium enlargement * Harsh mid-systolic ejection murmur - often associated with a thrill |
| Causes of pulmonary stenosis. | Pulmonary stenosis can be valvular, subvalvular, or supravalvular. * Usually congenital - may be associated with an intact ventricular septum or with an ASD (Fallot's tetralogy). Infection with rubella during pregnancy * Rheumatic fever (rare) * Carcinoid syndrome (rare) |
| Ix of pulmonary stenosis. | * CXR - shows prominent pulmonary artery * ECG - R atrial & RV enlargement. Maybe normal even in severe DS. * Doppler echo - Ix of choice |
| Rx for pulmonaary stenosis. | Severe DS requires pulmonary valvotomy (by ballon or direct surgery). K & C p750. |
| 1088 What are the pros & cons of mechanical vs tissue replacement valves? | Mechanical - more durable, however more thrombogenic (require lifelong anticoagulation) Tissue - degenerate after approx 10 years, require short-term anticoagulation (3/12) |
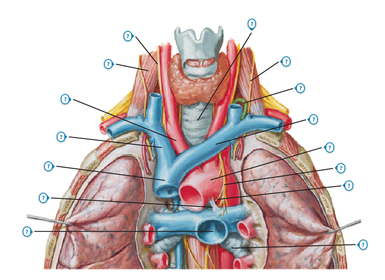
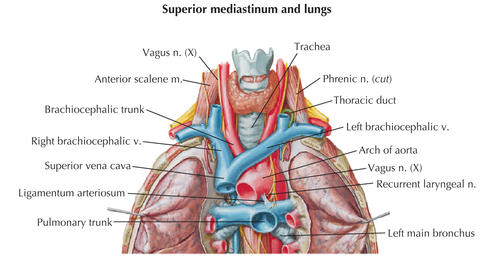
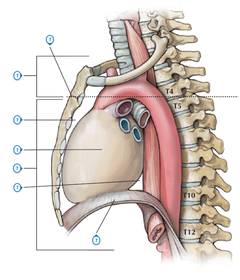
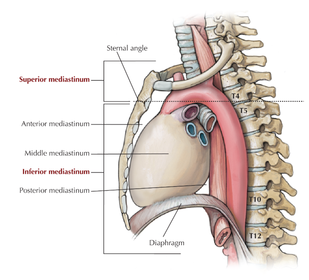
| 1093 Outline the contents of the inferior mediastinum. | * Anterior mediastinum: the region posterior to the body of the sternum & anterior to the pericardium (substernal region); contains a variable amount of fat. * Middle mediastinum: the region containing the pericardium & HT. Posterior mediastinum: the region posterior to the HT & anterior to the bodies of the T5-T12 vertebrae; contains the esophagus & its nerve plexus, thoracic aorta, azygos system of veins, sympathetic trunks & thoracic splanchnic nerves, lymphatics, & thoracic duct. Netters p125. |
| 1093 Outline the autonomic nerve supply to the HT and their respective functions. | * Parasympathetic fibers from the vagus nerve course as preganglionic nerves that synapse on postganglionic neurons in the cardiac plexus or within the HT wall itself. Parasympathetic stimulation: > Decreases heart rate. > Decreases the force of contraction. > Vasodilates coronary resistance vessels (although most vagal effects are restricted directly to the SA node region). * Sympathetic fibers arise from the upper thoracic cord levels (intermediolateral cell column of T1-T4/T5) and enter the sympathetic trunk. These preganglionic fibers synapse in the upper cervical & thoracic sympathetic chain ganglia, & then postganglionic fibers pass to the cardiac plexus. Sympathetic stimulation: > ^HR. > ^force of contraction. > Minimally vasoconstricts the coronary resistance vessels (via alpha adrenoceptors). Vasoconstriction, however, is masked by a powerful metabolic coronary vasodilation (mediated by adenosine release from myocytes), which is important because coronary arteries must dilate to supply BD to the HT as it ^its workload. Netter's p123. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
¿Quieres crear tus propias Fichas gratiscon GoConqr? Más información.