13414933
Descripción
Mapa Mental por david gonzalez, actualizado hace más de 1 año
|
|
Creado por david gonzalez
hace más de 6 años
|
|
Coronary Artery
Disease
- RISK FACTORS
- Non-Modifiable
- Gender
- men > women until 65 yr of age
- men > women until 65 yr of age
- Ethnicity
- Whites > Blacks
- South asians
- South asians
- Whites > Blacks
- Increasing Age
- Genetic
Predisposition
- Family History
- Gender
- Modifiable
- Obesity
- ↑ hypertension risk
- Enlarged
heart
- ↑ myocardial oxygen
consumption
- ↑ myocardial oxygen
consumption
- ↑ BMI
- ↑ hypertension risk
- Physical Inactivity
- ↓ HDL levels
- No collateral circulation encouragement
- atherosclerosis causes chronic ischemia, allowing
time for collateral circulation to develop. Well
developed collateral circulation might reduce the
mortality rate associated with coronary artery
disease. Coronary collateral development is
negatively related to ejection fracture. (Akgullu, 2014)
- atherosclerosis causes chronic ischemia, allowing
time for collateral circulation to develop. Well
developed collateral circulation might reduce the
mortality rate associated with coronary artery
disease. Coronary collateral development is
negatively related to ejection fracture. (Akgullu, 2014)
- ↓ HDL levels
- High homocysteine
levels
- damaging inner lining of blood
vessels
- promoting plaque build up
- altering clotting mechanism
- damaging inner lining of blood
vessels
- Tobacco
use
- ↓ estrogen levels
- menopausal women ↑ risk
- menopausal women ↑ risk
- nicotine
- ↑ catecholamine release, ↑ HR, ↑
peripheral vasoconstriction, ↑ BP, ↑
platelet adhesion
- ↑ catecholamine release, ↑ HR, ↑
peripheral vasoconstriction, ↑ BP, ↑
platelet adhesion
- ↓ estrogen levels
- Diabetes
- ↑ tendency for CT degeneration and endothelial
dysfunction
- ↑ cholesterol and triglyceride
levels
- ↑ tendency for CT degeneration and endothelial
dysfunction
- Depression
- ↑ circulating
catecholamines
- endothelial injury, inflammation, ↑ platelet
activity
- endothelial injury, inflammation, ↑ platelet
activity
- ↑ circulating
catecholamines
- BP >/ 140/90
- endothelial
injury
- ↑ rate of atherosclerotic development
- endothelial
injury
- substance
abuse
- coronary spasms resulting in myocardial ischemia & chest pain
- coronary spasms resulting in myocardial ischemia & chest pain
- ↑ triglyceride & LDL levels
- ↑ mortality rate
- ↑ mortality rate
- ↓ HDL
levels
- Obesity
- Non-Modifiable
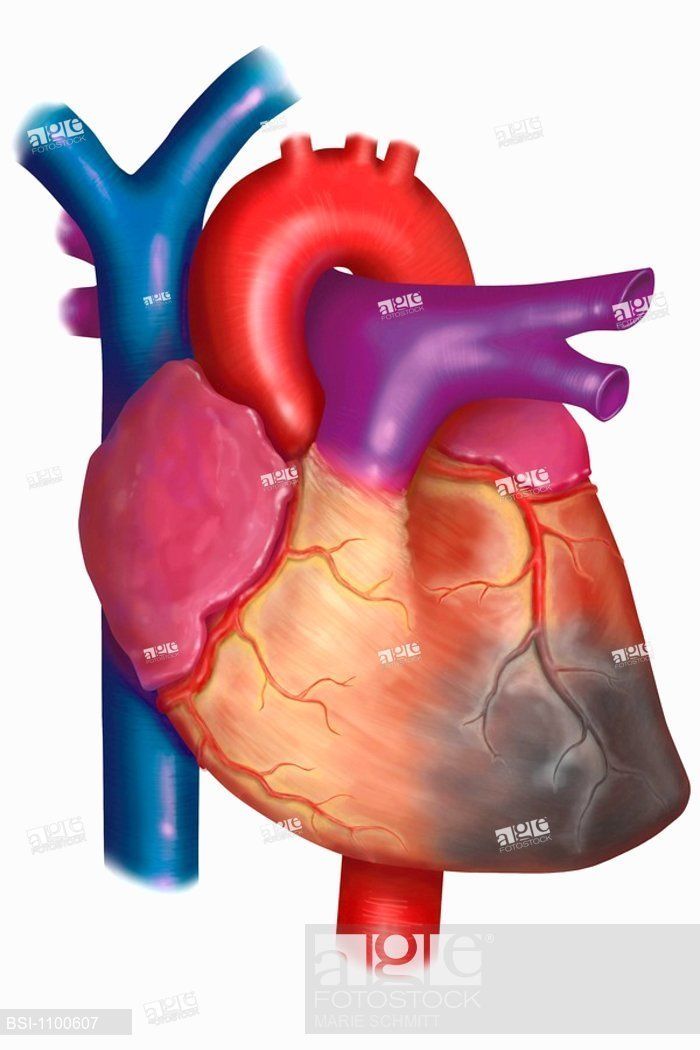
- ETIOLOGY &
PATHOPHYSIOLOGY
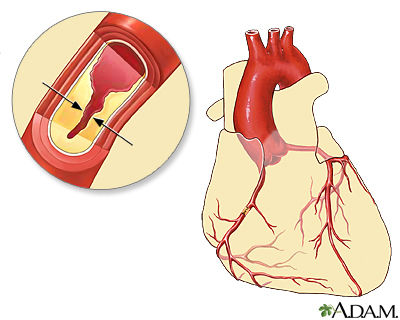
- Atherosclerosis
- Atherosclerotic Developmental Stages
- 1. Chronic Endothelial
Injury
- Causes of endothelial lining injury: tobacco use, hyperlipidemia,
hypertension, diabetes and infection, leading to inflammation
- Causes of endothelial lining injury: tobacco use, hyperlipidemia,
hypertension, diabetes and infection, leading to inflammation
- 2. Fatty Streak & Lipid
Core
- lipoprotein molecules enter arterial wall & are modified by oxidation.
Macrophages then ingest them & form foam cells. reversible, lipid filled
smooth muscle w/ yellow tinge
- lipoprotein molecules enter arterial wall & are modified by oxidation.
Macrophages then ingest them & form foam cells. reversible, lipid filled
smooth muscle w/ yellow tinge
- 3. Fibrous Plaque
Formation
- arterial wall changes, lipoproteins transport cholesterol and other lipids into
the arterial intima, fatty streak covered by collagen made by smooth muscle
cells, narrowing of vessel lumen. increased accumulation of lipids forms
pools causing cell necrosis in the wall.
- arterial wall changes, lipoproteins transport cholesterol and other lipids into
the arterial intima, fatty streak covered by collagen made by smooth muscle
cells, narrowing of vessel lumen. increased accumulation of lipids forms
pools causing cell necrosis in the wall.
- 4. Complicated
Lesion
- continued inflammation may result in plaque instability, ulceration and rupture,
platelets accumulate and thrombus forms, increased narrowing or complete occlusion
of the lumen. lethal ischemia through flow restriction.
- continued inflammation may result in plaque instability, ulceration and rupture,
platelets accumulate and thrombus forms, increased narrowing or complete occlusion
of the lumen. lethal ischemia through flow restriction.
- (Insull, 2009)
- 1. Chronic Endothelial
Injury
- ↑ CRP - non-specific marker of
inflammation
- Atherosclerotic Developmental Stages
- Atherosclerosis
- MANIFESTATIONS
OF CORONARY
ARTERY DISEASE
- Sudden Cardiac Death
- Prinzmetal angina
- caused by coronary
vasospasm
- can occur with or
without CAD
- can occur with or
without CAD
- caused by coronary
vasospasm
- Silent ischemia
- no subjective symptoms
- no subjective symptoms
- Chronic Stable
Angina
- Diagnosis
- coronary
angiography
- echocardiogram
- stress
test
- ECG
- ST-segment depression and/or T wave
insertion
- ST-segment depression and/or T wave
insertion
- coronary
angiography
- Precipitating Factors
- emotional stress
- ↑ SNS, ↑ Cardiac workload
- ↑ SNS, ↑ Cardiac workload
- Tobacco
Use
- ↑ catecholamine release, ↑
HR
- ↑ catecholamine release, ↑
HR
- Sexual Activity
- ↑ SNS, ↑ Cardiac
workload
- ↑ SNS, ↑ Cardiac
workload
- Stimulants
- ↑ HR, ↑ myocardial oxygen
demand
- ↑ HR, ↑ myocardial oxygen
demand
- Consumption of Heavy
Meal
- ↑ cardiac workload, more blood to GI, less to coronary
arteries
- ↑ cardiac workload, more blood to GI, less to coronary
arteries
- physical activity
- emotional stress
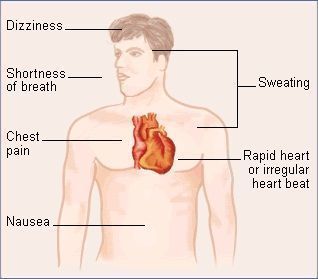
- Features & Symptoms
- triggered by physical activity or emotional
stress
- may still experience angina at rest
- may still experience angina at rest
- promptly relieved by sublingual
nitroglycerin
- dyspnea
- fatigue
- chest pain
- radiating
- radiating
- nausea
- shortness of breath
- breathlessness
- recurrent
belching
- anxiety
- diaphoresis
- triggered by physical activity or emotional
stress
- predictable pattern of chest pain with physical
exertion or stress due to atherosclerosis
- Diagnosis
- Acute Coronary
Syndrome
- Unstable Angina
- Diagnosis
- stress
test
- serum cardiac
markers
- echocardiogram
- ECG
- coronary
angiography
- stress
test
- Features & Symptoms
- easily provoked by minimal or no
exertion
- unpredictable emergency
- unexplained fatigue from chronic stable angina or first clinical
manifestation
- nausea
- anxiety
- diaphoresis
- chest pain, new
onset
- occurs at
rest
- radiates to upper extremities (left side) or
back
- occurs at
rest
- shortness of breath
- nitroglycerine may not help
- worse over time
- easily provoked by minimal or no
exertion
- unexpected chest pain at rest due to a thrombotic occlusion
secondary to atherosclerosis
- Diagnosis
- Myocardial
Infarction
- Clinical Manifestations
- severe immobilizing chest
pain
- activity or at
rest
- substernal, retrosternal & epigastric
(radiating)
- unrelieved by Nitroglycerine
- activity or at
rest
- SNS
stimluation
- catecholamine
release
- clammy cool
skin
- catecholamine
release
- fever 38°C, 24 hours - 1
week
- nausea and
vomitting
- diaphoresis
- denial
- fatigue & extreme weakness
- Cardiovascular
changes
- initial BP/HR
elevation
- BP later drops because of decreased
CO
- initial BP/HR
elevation
- necrotic zone
formation
- at 6 weeks, scar tissue replaces necrotic
tissue
- anxiety
- dyspnea
- hiccuping
- belching
- tinnitus
- severe immobilizing chest
pain
- Complications
- Cardiogenic
Shock
- severe left ventricular failure causing inadequate oxygen & nutrient
supply to tissues. Not pumping enough blood for body needs.
- severe left ventricular failure causing inadequate oxygen & nutrient
supply to tissues. Not pumping enough blood for body needs.
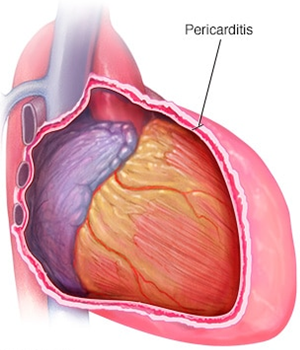
- Dressler's
syndrome
- pleuritic pain, fever, pericarditis, pericardial effusion
- pleuritic pain, fever, pericarditis, pericardial effusion
- Dysrhythmias
- fast HR, slow HR, irregular
beat
- fast HR, slow HR, irregular
beat
- Papillary muscle
dysfunction
- mitral valve regurgitation leading to ↓
CO
- mitral valve regurgitation leading to ↓
CO
- heart
failure
- Post-infarction Pericarditis
- pericardium inflammation causing
pain
- pericardium inflammation causing
pain
- Ventricular
aneurysms
- can rupture ventricle & harbour
thrombi
- can rupture ventricle & harbour
thrombi
- Cardiogenic
Shock
- Diagnosis
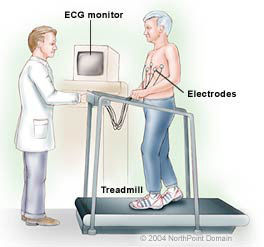
- stress test
- treadmill exercise test. to check heart response,
chest discomfort, BP & ECG changes
- treadmill exercise test. to check heart response,
chest discomfort, BP & ECG changes
- serum cardiac
markers
- MB isoenzyme of creatine kinase (CK-MB)
- cardiac specific troponin C (cTnT)
- cardiac specific troponin I (cTnI)
- MB isoenzyme of creatine kinase (CK-MB)
- echocardiogram
- Provides info about left ventricular function. Identify
non-working areas of the heart
- Provides info about left ventricular function. Identify
non-working areas of the heart
- ECG
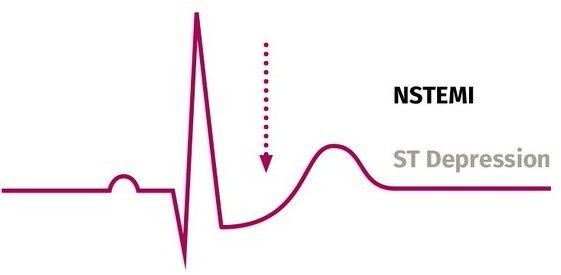
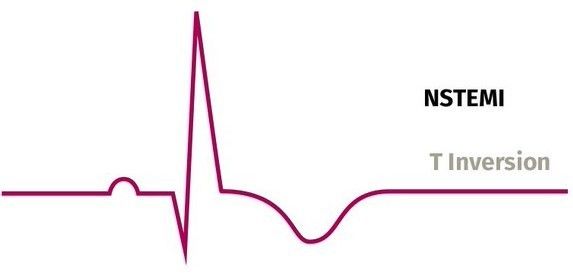
- NSTEMI
- partial blockage of coronary
artery
- No pathological Q wave
- depressed ST wave or T wave
inversion
- partial blockage of coronary
artery
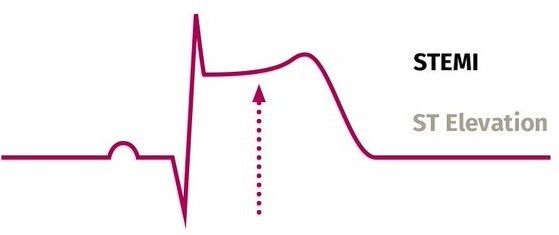
- STEMI
- elevated ST
wave
- pathological Q
wave
- full blockage of coronary
artery
- elevated ST
wave
- NSTEMI
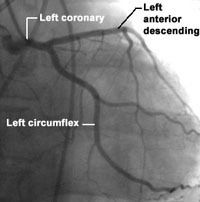
- coronary angiography
- X-ray test with special dye to locate blockage
- X-ray test with special dye to locate blockage
- stress test
- results from sustained ischemia
leading to myocardial necrosis
- Clinical Manifestations
- Unstable Angina
- Sudden Cardiac Death
- NURSING CARE
- 1. Assessment
- Subjective Data
- Risk
factors
- Current health
history
- Past Health
History
- Current
medications
- Pain
- exercise vs
rest
- squeezing, tight,
pressure
- upper chest, neck & jaw, epigastric,
epigastric radiating to neck, jaw &
arms, left shoulder, arms,
intrascapular
- 0-10, 10 being the most
severe pain you could
imagine
- onset, duration,
changes
- exercise vs
rest
- Risk
factors
- Objective Data
- General
- anxiety
- fear
- restlessness
- fatigue
- anxiety
- Integumentary
- cool skin
- diaphoresis
- pale skin
- cool skin
- Cardiovascular
- tachycardia
- arrhythmias
- ↑ levels of serum
lipids
- ↑ WBC
count
- ↑ or ↓ levels of serum
cardiac markers
- tachycardia
- Respiratory
- shortness of
breath
- exercise
intolerance
- exercise
intolerance
- shortness of
breath
- General
- Subjective Data
- 2. Planning
- Patient-centred care
- involvement of
family
- respect for patients'
preferences
- goal priority is patient
directed
- involvement of
family
- Nursing Goals
- relief of
pain
- ↓ risk
factors
- ↓ anxiety
- ↑ rehabilitation plan
involvement
- preserve
myocardium
- appropriate ischemia
treatment
- relief of
pain
- Nursing Diagnosis
- acute pain (angina)
- anxiety
- activity
intolerance
- risk for ↓ Cardiac
Output
- deficient knowledge
- ineffective self-health
management
- ineffective self-health
management
- risk for altered tissue
perfusion
- acute pain (angina)
- Patient-centred care
- 3.
Implementation
- Health Promotion
- Physical activity
- participate in exercise
programs
- ↑ exercise capacity
- ↑ exercise capacity
- ↑ endothelium-dependent
vasodilation
- reduced
rehospitalizations
- ↑ event-free
survival
- 2.5 hours of
exercise/week
- participate in exercise
programs
- Manage stress
- Stop
smoking
- ↓ blood clot formation
- ↓ blood clot formation
- ↑ social & emotional
support
- Health
Education
- teaching good health practices
- lifestyle habits can be positively
influenced at an early age
- teaching good health practices
- Nutritional
Therapy
- ↓ saturated fat and
cholesterol
- 30% of total calories from
fat
- 30% of total calories from
fat
- ↑ complex carbohydrates
- ↓ red meats, eggs
and whole milk
products
- ↓ alcohol and simple sugars
- ↓ serum triglyceride
levels
- ↓ serum triglyceride
levels
- ↑ fatty fish
- x2/week
- ↑ omega-3 fatty acids
- ↑ omega-3 fatty acids
- x2/week
- ↑ garlic
- ↓
hypertension
- ↓
hypertension
- ↑ soy & fiber
- ↓ cholesterol and LDL levels
- ↓ cholesterol and LDL levels
- niacin
- ↓ LDL, ↑
HDL
- ↓ LDL, ↑
HDL
- ↑ steaming, grilling, roasting
- ↓ saturated fat and
cholesterol
- Physical activity
- Acute Intervention
- administer supplemental oxygen
- vital signs
- 12-lead
ECG
- teach relaxation
techniques
- position the patient comfortably
- pain assessment
- prompt relief w/ medication
- prompt relief w/ medication
- reduce anxiety
- patient education
- maintain awareness to
adverse reactions to treatment
- heart
auscultation
- administer supplemental oxygen
- Collaborative Care
- Drug
Therapy
- Chronic Stable Angina
- Short-acting Nitrates
- vasodilators, resulting in ↓
pressures & ↓ wall stress
- vasodilators, resulting in ↓
pressures & ↓ wall stress
- Sublingual Nitroglycerin
- onset 3 mins, duration
30-60 mins
- rapid relief
- rapid relief
- onset 3 mins, duration
30-60 mins
- Long-acting Nitrates
- vasodilators to reduce incidents
of anginal attacks
- ↑ exercise tolerance
- ↑ exercise tolerance
- vasodilators to reduce incidents
of anginal attacks
- β-Adrenergic Blockers
- ↓ myocardial oxygen demand by decreasing HR, SVR,
BP & myocardial contractility
- thus ↑ exercise tolerance
- first line therapy
- first line therapy
- thus ↑ exercise tolerance
- ↓ myocardial oxygen demand by decreasing HR, SVR,
BP & myocardial contractility
- Calcium Channel Blockers
- systemic vasodilation w/ ↓ SVR
- ↓ myocardial contractility
- coronary vasodilation
- indicated for those who can't
tolerate or do not respond enough
to β-Adrenergic Blockers
- indicated for those who can't
tolerate or do not respond enough
to β-Adrenergic Blockers
- coronary vasodilation
- ↓ myocardial contractility
- systemic vasodilation w/ ↓ SVR
- ACE Inhibitors
- ↓ BP
- ↓ BP
- Short-acting Nitrates
- Acute Coronary Syndrome
- IV Nitroglycerin
- ↓ preload and afterload & ↑ the
myocardial oxygen supply
- ↓ preload and afterload & ↑ the
myocardial oxygen supply
- Morphine
Sulphate
- vasodilator
- ↓ anxiety & fear
- ↓ anxiety & fear
- vasodilator
- IV β-Adrenergic Blockers
- ↓myocardial oxygen demand by
decreasing HR, SVR, BP & myocardial
contractility
- ↓myocardial oxygen demand by
decreasing HR, SVR, BP & myocardial
contractility
- Ace
Inhibitors
- ↓ BP
- slows progression of
heart failure
- ↓ CV death, stroke &
revascularization
- if intolerant use
Angiotensin II blockers
- if intolerant use
Angiotensin II blockers
- ↓ CV death, stroke &
revascularization
- slows progression of
heart failure
- ↓ BP
- Cholesterol lowering drugs
- IV Nitroglycerin
- Chronic Stable Angina
- Surgical
Interventions
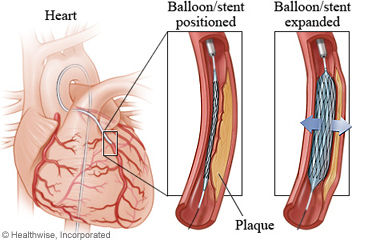
- Percutaneous Coronary Intervention
- non-surgical
procedure
- catheter with stent mounted on balloon
- stent with balloon inflated
- stent in place & balloon withdrawn
- plaque compressed & blocked coronary artery
opened
- symptom relief is immediate & of greater magnitude
compared to medical therapy
- restenosis occurs 20-40% requiring reintervention
- restenosis occurs 20-40% requiring reintervention
- symptom relief is immediate & of greater magnitude
compared to medical therapy
- plaque compressed & blocked coronary artery
opened
- stent in place & balloon withdrawn
- stent with balloon inflated
- catheter with stent mounted on balloon
- non-surgical
procedure
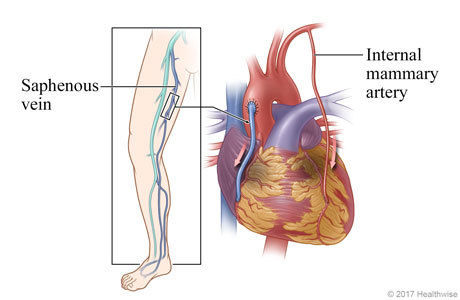
- Coronary Artery Bypass Graft
Surgery
- bypass blocked portion of coronary artery with a healthy
blood vessel from somewhere else in the body
- most commonly used are the left internal mammary artery & saphenous
vein
- arterial conduits preferred to reduce subsequent development of obstructive lesions
- blood reaches the heart muscle through new pathway
- blood reaches the heart muscle through new pathway
- arterial conduits preferred to reduce subsequent development of obstructive lesions
- most commonly used are the left internal mammary artery & saphenous
vein
- bypass blocked portion of coronary artery with a healthy
blood vessel from somewhere else in the body
- Percutaneous Coronary Intervention
- Interprofessional
Collaboration
- primary care
physician
- cardiologist
- nurse
educator
- rehabilitation
nurse
- physical
therapist
- psychiatrist
- social
worker
- dietitian
- cardiovascular
surgeon
- geriatrician
- heart failure nurse
- primary care
physician
- Drug
Therapy
- Health Promotion
- 4. Evaluation
- evaluate whether nursing care was
effective
- conduct evaluation measures to determine if expected outcomes are
met
- evaluate whether nursing care was
effective
- 1. Assessment
- By: David Gonzalez
& Arvin Raras
- References (click
note icon top
right of bubble)
Nota:
- References Akgullu, C., Ufuk, E., Ok, I., Gungor, H., Avcil, M., Dagli, B., Omurlu I.K., Zencir, C. (2014). Predictors of well developed coronary collateral circulation in patients with stable angina pectoris. J Clin Exp Cardiolog, 5(4); 1-7. Cassar, A., Holmes, D.R. Jr., Rihal, C.S., Gersh, B.J. (2009). Chronic coronary artery disease: diagnosis and management. Mayo Clinic Proceedings, 84(12): 1130-46. Coronary Artery Disease: How Your Diet Can Help. (2003). Am Fam Physician, 67(8); 1769-1770. Hajar, R. (2017). Risk Factors for Coronary Artery Disease: Historical and Perspectives. Heart Views, 18(3): 109-114. Health Canada. (2011). Eating well with Canada’s food guide. Retrieved from https://www.canada.ca/content/dam/hc-sc/migration/hc-sc/fn-an/alt_formats/hpfb-dgpsa/pdf/food-guide-aliment/print_eatwell_bienmang-eng.pdf Hembrecht, R., Wolf, A., Gielen, S., Linke, A., Hofer, J. (2000). Effect of exercise on coronary endothelial function in patients with coronary artery disease. N Engl J Med, 342; 454-460. Hillis, G.S. (2002) Management of stable angina and unstable angina/non-st-elevation myocardial infarction. Medicine, 30(4); 64-70. Hombach, V., Grebe, O., Merkle, N., Waldenmaier, S., Hoher, M., Kochs, M., Wohrle, J., Kestler HA. (2005). Sequelae of acute myocardial infarction regarding cardiac structure and function and their prognostic significance as assessed by magnetic resonance imaging. Europaean Heart Journal, 26(6); 549-557. Insull, W Jr. (2009). The pathology of atherosclerosis: plaque development and plaque responses to medical treatment. The American Journal of Medicine, 122(1 Suppl; S3-S14. Jaarsma, T. (2005). Inter-professional team approach to patients with heart failure. Heart, 91(6); 832-838. Kimble, L.P., Dunbar, S.B., Weintraub, W.S., McGuire, D.B., Manzo, S.F., Strickland, O.L. (2011). Symptom clusters and health-related quality of life in people with chronic stable angina. Journal of Advanced Nursing, 67(5); 1000-1011. Kumar, A. Cannon, C.P. (2009) Acute Coronary Syndromes: Diagnosis and Management, Part 1. Mayo Clinic Proceedings, 84(10); 917-938. Lewis, S. L., Dirksen, S. R., Heitkemper, M. M., Bucher, L., & Camera, I. M.(Eds.). (2014). Medical-surgical nursing in Canada: Assessment and management of clinical problems (3rd Cdn. ed.) (M. A. Barry, S. Goldsworthy & D. Goodridge, Cdn. Adapt.). Toronto: Elsevier Canada. Taghipour, B., Nia, H.S., Kaveh, H., Heideranlu, E., Far, S.S., Zeydi A.E., Soleimani, M.A. (2014) Clinical manifestations of myocardial infarction in diabetic and non-diabetic patients. Iran J Crit Care Nurs, 7(2); 116-123. Registered Nurses’ Association of Ontario. (2013). Assessment and Management of Pain. Toronto, Canada: Registered Nurses’ Association of Ontario. Thadani, U. (2004). Current medical management of chronic stable angina. J Cardiovasc Pharamacol Therapeut, 9(Supplement 1); S11-S29. Thompson, E.G., McPherson, J.A., (2010) Coronary artery disease: roles of different doctors. Heallthwise. Retrieved from https://www.uofmhealth.org/node/652182. Wee, Y., Burns, K., Bett, N. (2015). Medical management of chronic stable angina. Aust Prescr, 38(4): 131-136. Zaman, M.J., Philipson, P., Chen, R., Farag, A., Shipley, M., Marmot, M.G., Timmis, A.D., Hemingway, H. South Asians and coronary artery disease: is there discordance between effects on incidence and prognosis? Epidemiology, 99(10); 729-736.
- References (click
note icon top
right of bubble)
Recursos multimedia adjuntos
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
¿Quieres crear tus propios Mapas Mentales gratis con GoConqr? Más información.