16978900
Descripción
Mapa Mental por Fatima Alkhateeb, actualizado hace más de 1 año
|
|
Creado por Fatima Alkhateeb
hace casi 6 años
|
|
Breast cancer
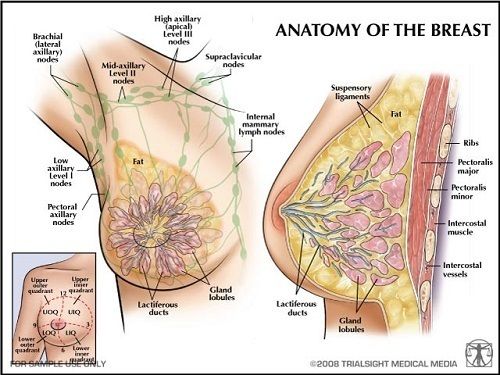
- Anatomy of the breast
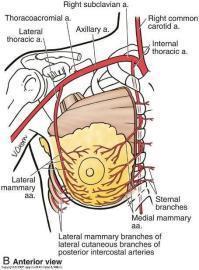
- Blood supply
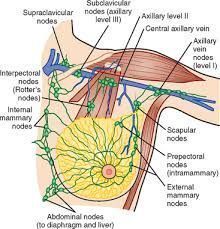
- Lymphatic drainage
- Blood supply
- Risk factors
- Early menarche
- Not breastfeeding
- Using hormone
replacement therapy
- Obesity
- Early menarche
- Signs and symptoms
- Change in breast size or shape
- Nipple discharge
- Lump in the breast
- Redness, dimpling of the skin
- Change in breast size or shape
- Tumors of the breast
- Benign
- Fibroadenoma
- Small, well-defined, mobile mass,
increased size and tenderness with
high estrogen, women < 35 years old
- Small, well-defined, mobile mass,
increased size and tenderness with
high estrogen, women < 35 years old
- Intraductal
papilloma
- Small fibroepithelial tumor within lactiferous ducts, typically
beneath areola, most common cause of nipple discharge
- Small fibroepithelial tumor within lactiferous ducts, typically
beneath areola, most common cause of nipple discharge
- Phyllodes tumor
- Large mass of connective tissue and cysts with
“leaf-like” lobulations, most common in 5th decade
- Large mass of connective tissue and cysts with
“leaf-like” lobulations, most common in 5th decade
- Fibroadenoma
- Malignant
- Non-invasive
- DCIS
- Fills ductal lumen (neoplastic cells in duct; engorged blood
vessel). Arises from ductal atypia. Often seen early as
microcalcifications on mammography
- Cribriform type
- Comedo type
- Central
necrosis
- Central
necrosis
- Cribriform type
- Fills ductal lumen (neoplastic cells in duct; engorged blood
vessel). Arises from ductal atypia. Often seen early as
microcalcifications on mammography
- LCIS
- Proliferation of cells in lobules, Discohesive growth, round cells clumped together
- Proliferation of cells in lobules, Discohesive growth, round cells clumped together
- Paget's
disease
- Results from underlying DCIS or invasive breast cancer. Eczematous
patches on nipple . Paget cells = intraepithelial adenocarcinoma cells.
- Results from underlying DCIS or invasive breast cancer. Eczematous
patches on nipple . Paget cells = intraepithelial adenocarcinoma cells.
- DCIS
- Invasive
- Invasive ductal carcinoma
- Firm, fibrous, “rock-hard” mass with sharp margins and small,
glandular, duct-like cells. Tumor can deform suspensory
ligaments. Classic morphology: “stellate” infiltration
- Firm, fibrous, “rock-hard” mass with sharp margins and small,
glandular, duct-like cells. Tumor can deform suspensory
ligaments. Classic morphology: “stellate” infiltration
- Invasive lobular carcinoma
- Orderly row of cells (“single file”), due to loss of E-cadherin
expression. Often bilateral with multiple lesions in the same location.
- Orderly row of cells (“single file”), due to loss of E-cadherin
expression. Often bilateral with multiple lesions in the same location.
- Medullary carcinoma
- Fleshy, cellular, lymphocytic infiltrate, good prognosis
- Fleshy, cellular, lymphocytic infiltrate, good prognosis
- Inflammatory breast cancer
- Dermal lymphatic invasion by breast carcinoma. Peau d’orange
(skin texture resembles orange peel due to edema leading to
tightening of Cooper’s suspensory ligament)
- Dermal lymphatic invasion by breast carcinoma. Peau d’orange
(skin texture resembles orange peel due to edema leading to
tightening of Cooper’s suspensory ligament)
- Invasive ductal carcinoma
- Non-invasive
- Benign
- Physical
examination
- Look for symmetry,
irregular lumps, change
in shape and size,
tenderness, discharge
- Look for symmetry,
irregular lumps, change
in shape and size,
tenderness, discharge
- Investigations
- FNA biopsy
- very thin, hollow needle attached to
a syringe used to aspirate tissue
from suspicious area
- Contraindications
- coagulopathy or
platelet disorder
- coagulopathy or
platelet disorder
- very thin, hollow needle attached to
a syringe used to aspirate tissue
from suspicious area
- FNA biopsy
- Treatment and management
- Surgery
- chemotherapy
- Radiation
- Surgery
Recursos multimedia adjuntos
{kind=link}
{kind=link}
{kind=link}
¿Quieres crear tus propios Mapas Mentales gratis con GoConqr? Más información.