2734240
The Kidney and Drug Elimination
- Identify the role of kidneys in
the excretion and regulation of
the blood pH
- Production of hormones
- rennin to control blood pressure
- rennin to control blood pressure
- Filtering blood, to form urine
- Regulation of plasma
osmolarity and volume
- Regulation of plasma
osmolarity and volume
- Maintain water, ionic and pH balance in body fluids
- Elimination of nitrogen containing metabolic waste
- Urea= amino acid break down
- Uric acid = nucleic acid break down
- Urea= amino acid break down
- Indirectly regulate composition of extra cellular fluid too
- Production of hormones
- Identify processes contributing to the renal excretion and implement this
on elimination of drugs
- ELIMINATION
- ADME
- irreversible removal of the
drug form the body
- = metabolism + excretion
- kindeys contribute to
excretion
- parent drugs are often lipophillic so they remain in the
body for longer, one mechanism to remove drugs involves
converting these into polar, hydrophilic metabolites so
they are easier to eliminate
- unchanged drugs eliminated via renal excretion,
dominant route
- parent drugs are often lipophillic so they remain in the
body for longer, one mechanism to remove drugs involves
converting these into polar, hydrophilic metabolites so
they are easier to eliminate
- some metabolising in
kidenys too
- dependant on
physicochemical
properties of drug
- kindeys contribute to
excretion
- ADME
- Glomelular filtration = non
selective, passive
- Samll sugars, water, urea,
uric acid, K Na Cl- ions
- No cells or large proteins
- No cells or large proteins
- Drugs unbound to plasm proteins
- Samll sugars, water, urea,
uric acid, K Na Cl- ions
- Tubular Secretion
- Selective transport from peritubular fluid
to lumen of renal tubules
- Occurs in poximal and distal tublues via
different tansportet proteins OAT, OCT
- SATURABLE PROCESS, once the conc of drug is
increased, transporter proteins become
saturated- limit rate of excretion
- acidic and basic drugs excreted this way
- SATURABLE PROCESS, once the conc of drug is
increased, transporter proteins become
saturated- limit rate of excretion
- Occurs in poximal and distal tublues via
different tansportet proteins OAT, OCT
- Selective transport from peritubular fluid
to lumen of renal tubules
- Tubular Reabsoprtion
- From renal tubules membrane back
in to plasma either passive or use of
trnasporters
- lipophillic unionised drugs, nutrients
absorbed too - often with WA or WB
depending urine pH
- Descending loop of Henle not permeable to NA+
Ascending loop of Henle – active reabsorption of
Na+, not permeable to H20
- From renal tubules membrane back
in to plasma either passive or use of
trnasporters
- ELIMINATION
- Identify main transporters involved in renal elimination
- OAT1, 2, 3
- Organic anion transporter
transport small anionic
drugs
- OAT1
- transmembrane
- mainly on basolateral membrane of proximal tubular cells
- mainly on basolateral membrane of proximal tubular cells
- transmembrane
- OAT1
- Organic anion transporter
transport small anionic
drugs
- OCT2
- Organic cation transporter,
move hydrophilic small
cations
- Potential DDI via inhibition of OCT eg penicillin and preobenicin
- Potential DDI via inhibition of OCT eg penicillin and preobenicin
- Organic cation transporter,
move hydrophilic small
cations
- OAT1, 2, 3
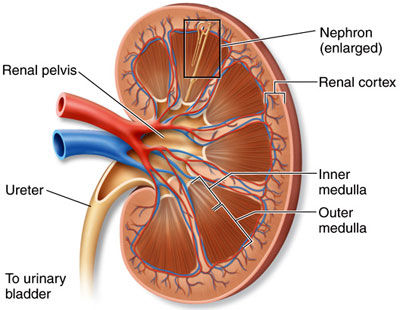
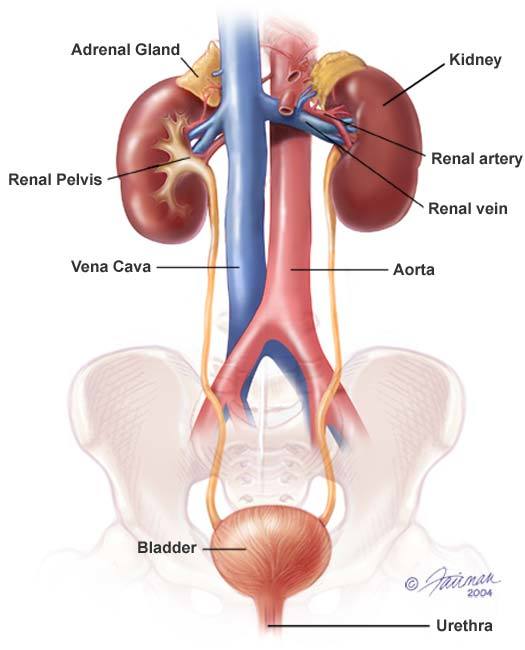
- Structure
- highly perfused,
receives around 20% of
cardiac output
- Cortex
- Medula
- Pyramids
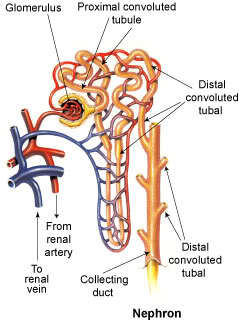
- Nephrons
- Bowman's
capsule
- Glomerulas = cluster of capillaries
- Filters the blood,
remaining blood
leaves via
efferent ateriole
- Glomerulas = cluster of capillaries
- Secretion of drugs- proximal tube
Reabsorption - distal tube
- 180L blood filtered
per day
- Diabetes mellitus
- glucose in urine, increase in osmotic
pressure in renal tubule, less water
reabsorbed and more urination
- glucose in urine, increase in osmotic
pressure in renal tubule, less water
reabsorbed and more urination
- Bowman's
capsule
- Nephrons
- Pyramids
- Medula
- GFR = glomerular
filtration rate
- Creatine or inulin used- do not bind to plasma proteins
- 120-110 ml/min
- Creatine or inulin used- do not bind to plasma proteins
- highly perfused,
receives around 20% of
cardiac output
- Dose
adjustment
- Fraction of drug excreted unchanged (via kidneys) is > 50%
For drugs with narrow therapeutic index - e.g., digoxin
Impaired metabolism
- Fraction of drug excreted unchanged (via kidneys) is > 50%
For drugs with narrow therapeutic index - e.g., digoxin
Impaired metabolism
Recursos multimedia adjuntos
{kind=link}
{kind=link}
{kind=link}
{kind=link}
¿Quieres crear tus propios Mapas Mentales gratis con GoConqr? Más información.