4719104
Type 1 Diabetes Mellitus
- Collaborative care
- Primary goals of care
(must be individually
tailored
- Reach ideal blood
sugar levels and
maintain it
- educate both client and parent
regarding the necessary skills
and knowledge to manage the
disease
- decrease symptoms
and promote
well-being
- prevent acute and
non-acute
complications
- delay onset and
progression of
long-term complications
- optimize quality of life for client and family
- Reach ideal blood
sugar levels and
maintain it
- Nursing Care
- b) Insulin Therapy
- # of injections, timing, and dose of insulin per day
- dependent on age, lifestyle,
meal plan, general health
and motivation
- depends on family socioeconomic factors, and
family, physician preferences
- dependent on duration of diabetes
- 1) Honeymoon period -
two years after initial
dianosis
- low insulin
required (< 0.5
units/kg/day)
- low insulin
required (< 0.5
units/kg/day)
- 2) After the two years, intensive
diabetes management
- 1) Honeymoon period -
two years after initial
dianosis
- dependent on age, lifestyle,
meal plan, general health
and motivation
- Types
- i) and ii) used in conjunction with each other
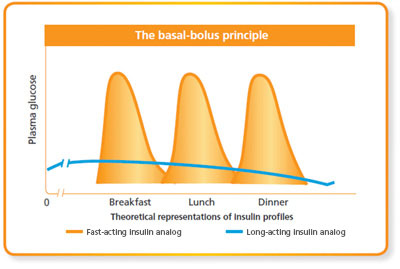
- i) basal-bolus regimens
- Study: long and rapid-acting
insulin-determir and
glargine
- improves fast-acting blood glucose
levels and fewer episodes of
nocturnal hypoglycemia
- improves fast-acting blood glucose
levels and fewer episodes of
nocturnal hypoglycemia
- Study: long and rapid-acting
insulin-determir and
glargine
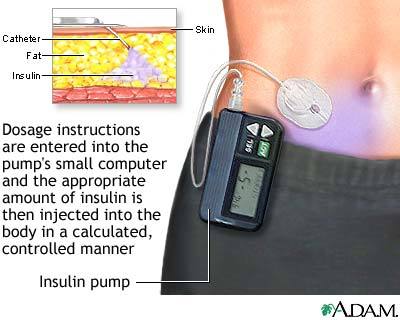
- ii) continuous subcutaneous
insulin fusion (insulin pump
therapy)
- reduction in glycated
hemoglobin (A1C) with
reduced hypoglycemia for
12-24 mos.
- reduction in glycated
hemoglobin (A1C) with
reduced hypoglycemia for
12-24 mos.
- i) basal-bolus regimens
- i) and ii) used in conjunction with each other
- # of injections, timing, and dose of insulin per day
- a) Glucose Monitoring
- 1) self-monitoring of glucose
- useful in evaluating
individual response to
therapy, to see if
glycemic targets are
being achieved
- computerized blood glucose
meters most accurate and
precise but proper patient
education is mandatory
- computerized blood glucose
meters most accurate and
precise but proper patient
education is mandatory
- prior to meals
and snacks, at
bedtime, and
before exercise
- useful in evaluating
individual response to
therapy, to see if
glycemic targets are
being achieved
- 2) Glycosylated Hemoglobin
(HbA1c) Testing
- long-term
assessment of
glucose control
- evaluate whether
planned insulin
regimens is effective
- patient with
stable glycemic
levels: perform
2x/year
- patient with unstable glycemic levels or
have recently changed their therapy:
perform every 2-3 months
- patient with
stable glycemic
levels: perform
2x/year
- evaluate whether
planned insulin
regimens is effective
- long-term
assessment of
glucose control
- 1) self-monitoring of glucose
- b) Insulin Therapy
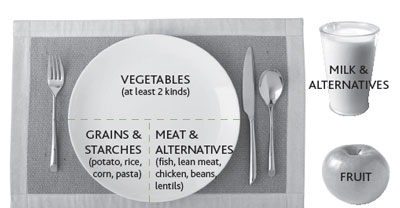
- Nutrition
- Follow 4 Canadian food groups
- Individualized to one`s
nutritional needs, eating
habits and lifestyle
- planned and evaluated
at least annually
- planned and evaluated
at least annually
- Teach using plate method
- Follow 4 Canadian food groups
- Lifestyle
- Smoking cessation
- increase risk for macrovascular and
microvascular diabetes
complications
- Teach
about
smoking
prevention
- Teach
about
smoking
prevention
- increase risk for macrovascular and
microvascular diabetes
complications
- Safe sex
- avoid unplanned
pregnancy
- increased risk of STDs,
and other maternal and
fetal complications
- education about
sexual health and
contraception
- education about
sexual health and
contraception
- increased risk of STDs,
and other maternal and
fetal complications
- avoid unplanned
pregnancy
- Smoking cessation
- Psychological Issues
- Early identification, early
intenvention to avoid impact
over course of development
- increased risk for
depression, anxiety, eating
disorders
- associated with
poor glycemic
control
- affected by
family distress-
maternal
anxiety and
depression
- associated with
poor glycemic
control
- increased risk for
depression, anxiety, eating
disorders
- be aware of insulin
omissions in young adult
females to maintain body
image
- Early identification, early
intenvention to avoid impact
over course of development
- Primary goals of care
(must be individually
tailored
- Nursing Management
- 1) Assessment
- Non-Acute/Post
stabilization of
acute
complications
- obtain complete
health hx, and
conduct physical
assessment
- Look for: S&S of DKA,
hemorrhages and exudates
in the retina, presences of
scars and wounds especially
around feet, peripheral
sensory loss, peripheral
edema, presence of ankle
and knee reflexes using a
tendon hammer, carotid
bruits for artherosclerosis
- Assess for history of
mental health services,
presence of family and
social support for
diabetes self-care tasks,
alcohol and substance
abuse history
- Look for: S&S of DKA,
hemorrhages and exudates
in the retina, presences of
scars and wounds especially
around feet, peripheral
sensory loss, peripheral
edema, presence of ankle
and knee reflexes using a
tendon hammer, carotid
bruits for artherosclerosis
- measure fasting
blood glucose, urine
ketone levels,
hemoglobin A1c,
- psychological/social
health
- Ability to perform
self-care and to
learn self-care skills
- visual, motor,
and neuronal
deficits, and
literacy skills
- visual, motor,
and neuronal
deficits, and
literacy skills
- presence of family support and financial resources
- Ability to perform
self-care and to
learn self-care skills
- obtain complete
health hx, and
conduct physical
assessment
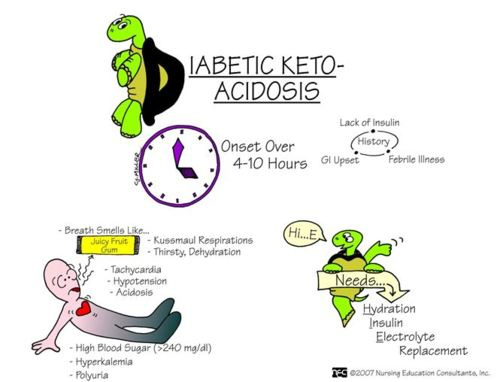
- Acute
- DKA
- S&S: ketonuria, Kussmaul
respirations, OHypo, lethargy,
fruity breath odour nausea,
vomiting, abdominal pain
- arterial blood pH < 7.3,
serum bicarbonate level
< 15 mEq/L, moderate to
high levels of ketone in
urine
- arterial blood pH < 7.3,
serum bicarbonate level
< 15 mEq/L, moderate to
high levels of ketone in
urine
- S&S: ketonuria, Kussmaul
respirations, OHypo, lethargy,
fruity breath odour nausea,
vomiting, abdominal pain
- acute hypoglycemia
- S&S: weakness, fatigue,
hunger, shakiness,
nervousness, sweating,
light-headedness,
sleepiness, confusion,
difficulty speaking, anxiety
- serum glucose level: <50
mg/dL in men, <45 mg/dL in
women, <40 mg/dL in children
- serum glucose level: <50
mg/dL in men, <45 mg/dL in
women, <40 mg/dL in children
- S&S: weakness, fatigue,
hunger, shakiness,
nervousness, sweating,
light-headedness,
sleepiness, confusion,
difficulty speaking, anxiety
- DKA
- Non-Acute/Post
stabilization of
acute
complications
- 2) Planning
- i) maintain optimal blood
glucose level, fluid, and
electrolyte balance
- ii) promote
quality of life
- improve ability to perform
self-care
- manage anxiety,
depression
- improve nutritional
intake and meet
healthy weight goals
- improve ability to perform
self-care
- ii) promote
quality of life
- i) maintain optimal blood
glucose level, fluid, and
electrolyte balance
- 3) Implementation
- Acute intervention
- maintain fluid and
electrolyte balance
- IV fluid and/or oral
fluids as prescribed
- IV fluid and/or oral
fluids as prescribed
- insulin therapy
- Initially give IV bolus
- as pt condition improves
gives subcutaneous
injections
- as pt condition improves
gives subcutaneous
injections
- Initially give IV bolus
- maintain fluid and
electrolyte balance
- health promotion
- address any
misconceptions pt or
family has about diabetes
- provide
emotional
support,
setting aside
time to talk
with pt and.or
family
- especially in a newly
diagnosed patient
- in adult-diagnosed
T1DM patients,
sudden and new
approach to daily
life is needed
- barriers: not obtaining
enough info about T1DM,
limited time and access to
appropriate healthcare
network, social stigma
with living with diabetes
- barriers: not obtaining
enough info about T1DM,
limited time and access to
appropriate healthcare
network, social stigma
with living with diabetes
- in adult-diagnosed
T1DM patients,
sudden and new
approach to daily
life is needed
- provide
opportunities to
express feelings
about his ilness
- especially in a newly
diagnosed patient
- educate family and pt
about diabetes
self-care, nutrition,
and healthy lifestyle
- focus on client-centred
care, and promote
client freedom and
choice
- provide positive
reinforcement for
increasing involvement in
self-care activities
- establish mutual and
specific short-term and
long-term goals for
self-management in
controlling blood glucose
- adult patients and
family of younger
patients should have
adequate information
to participate in
decision making
- establish personal
network of
supportive
healthcare
professionals and
family members
- establish personal
network of
supportive
healthcare
professionals and
family members
- 2 years before child turn into
adult (18 yrs of age), health care
provider must begin to
collaboratively develop a
transition plan from pediatric to adult diabetes care
- adult patients and
family of younger
patients should have
adequate information
to participate in
decision making
- establish mutual and
specific short-term and
long-term goals for
self-management in
controlling blood glucose
- provide positive
reinforcement for
increasing involvement in
self-care activities
- focus on client-centred
care, and promote
client freedom and
choice
- address any
misconceptions pt or
family has about diabetes
- Acute intervention
- 4) Evaluation
- observe the
stabilization of
acute situations
- are blood glucose, ketone
levels, and vital signs
stabilized?
- yes
- Are they meeting the blood
glucose, ketone level goals
as individualized by their
healthcare practitioners?
- yes
- Has patient's
psychological/emotional
status improved in
comparison to the
beginning of the
encounter?
- Does the patient
have a better
understanding
on the self-care
interventions as
suggested?
- Does the patient
have a better
understanding
on the self-care
interventions as
suggested?
- Has patient's
psychological/emotional
status improved in
comparison to the
beginning of the
encounter?
- no
- How can I correct/re-align
their level of
understanding of T1DM?
- How can nurse
educational methods
be adjusted to be
more acceptable for
the patient?
- How does the nurse feel about
her experience with the
patient?
- What improvements
can be made next
time?
- What improvements
can be made next
time?
- How does the nurse feel about
her experience with the
patient?
- How can nurse
educational methods
be adjusted to be
more acceptable for
the patient?
- Does the patient
seem receptive to
the lifestyle
changes as
proposed?
- Make referrals to
nutritionists,
psychologists, and other
healthcare professionals
as needed
- Make referrals to
nutritionists,
psychologists, and other
healthcare professionals
as needed
- How can I correct/re-align
their level of
understanding of T1DM?
- yes
- Are they meeting the blood
glucose, ketone level goals
as individualized by their
healthcare practitioners?
- no
- re-assess
- re-assess
- yes
- are blood glucose, ketone
levels, and vital signs
stabilized?
- observe the
stabilization of
acute situations
- 1) Assessment
- Etiology and
Epidemiology
- happens most often in
childhood, but adults can
also develop it later in
life
- general population risk:
1/300, 6/100 chance if a
first degree relative
was diagnosed (sister,
brother, son, daughter
- More than
300,000
Canadians live
with T1DM.
- pts with
first-degree
diagnosed
relative
- annual screening before
10 yrs old, and 1
additional screening
during adolescence
- annual screening before
10 yrs old, and 1
additional screening
during adolescence
- More than
300,000
Canadians live
with T1DM.
- general population risk:
1/300, 6/100 chance if a
first degree relative
was diagnosed (sister,
brother, son, daughter
- Cause of T1DM is still
unknown, but studies
suggest could be
genetic or viral
- increased risk by
mutation of the
HLA genes
- HLA complex helps
immune system
distinguish the body's
own proteins from
foreign, pathological
proteins
- When HLA complex is mutated,
T-cells recognize endogenous insulin
as invasive, subsequently destroying
them
- When HLA complex is mutated,
T-cells recognize endogenous insulin
as invasive, subsequently destroying
them
- HLA complex helps
immune system
distinguish the body's
own proteins from
foreign, pathological
proteins
- Rubella, mumps,
cytomegalovirus
have been suggested
to destroy
insulin-producing
beta cells
- increased risk by
mutation of the
HLA genes
- happens most often in
childhood, but adults can
also develop it later in
life
- Pathology, Clinical
Manifestations, and
Co-morbidities
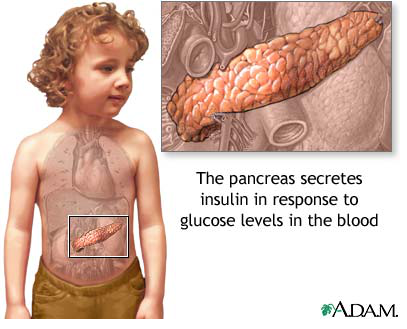
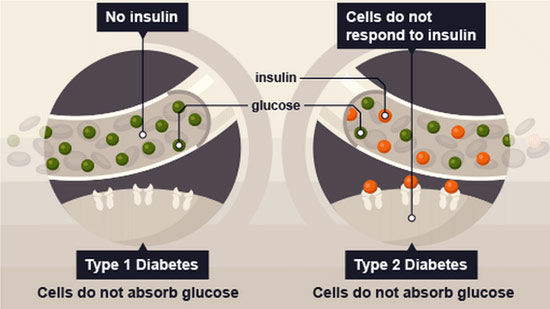
- Body can't
produce insulin
- no hormone to store
glucose from food
intake into liver,
muscle, and fat cells
- unregulated
glucose levels in
blood
- polydipsia, polyphagia, polyuria,
extreme fatigue, blurry vision, slow
healing of cuts and bruises, weight loss
despite massive food intake, tingling,
pain, and numbness in peripheries
- Comorbidities
- Diabetic Ketoacidosis (leading
cause of mortality in children
with T1DM)- body digests lipids
instead of glucose, and there is a
buildup of ketones in the body
- prevented through early
diagnosis and initiation of
insulin therapy
- prevented through early
diagnosis and initiation of
insulin therapy
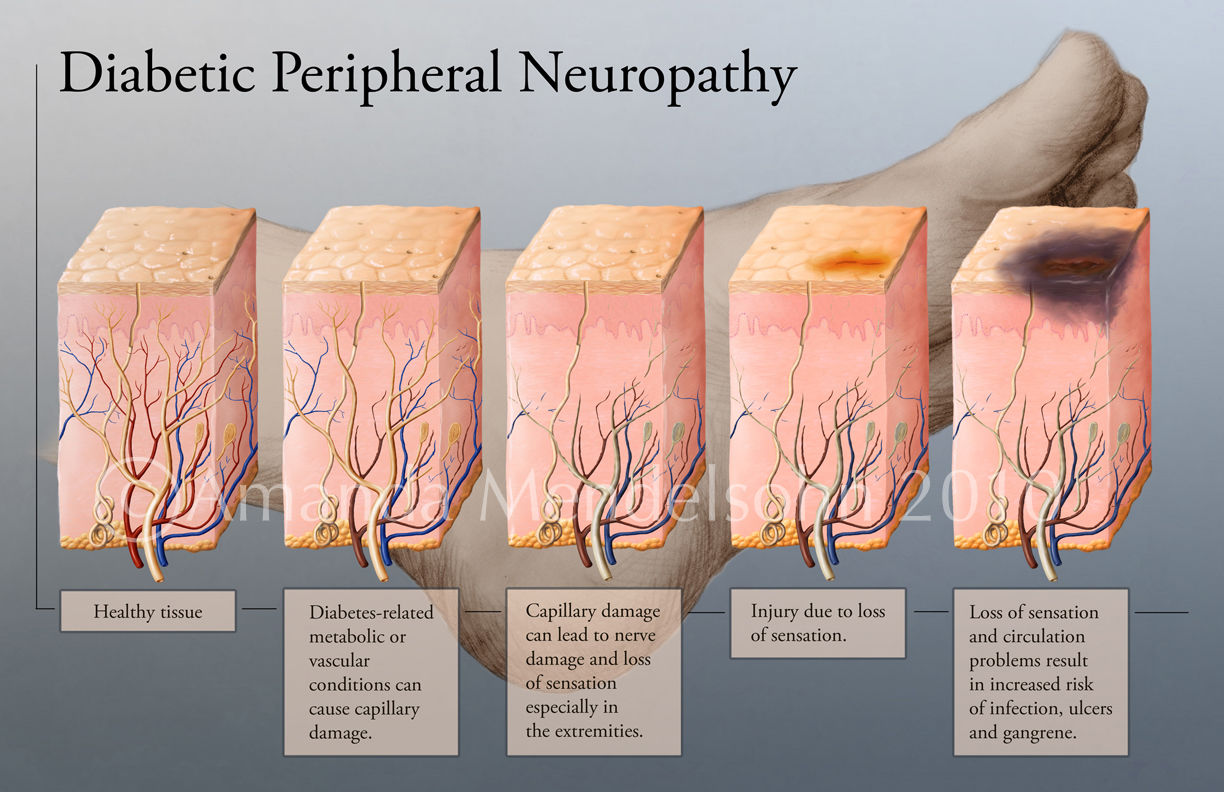
- Nerve,
capillary
damage
- neuropathy,
nephropathy, eye
damage, foot damage,
infections
- neuropathy,
nephropathy, eye
damage, foot damage,
infections
- hypertension,
artherosclerosis
- increased risk for
heart attacks, heart
failure, myocardial
infarction
- increased risk for
heart attacks, heart
failure, myocardial
infarction
- dyslipidemia
- Diabetic Ketoacidosis (leading
cause of mortality in children
with T1DM)- body digests lipids
instead of glucose, and there is a
buildup of ketones in the body
- Comorbidities
- polydipsia, polyphagia, polyuria,
extreme fatigue, blurry vision, slow
healing of cuts and bruises, weight loss
despite massive food intake, tingling,
pain, and numbness in peripheries
- unregulated
glucose levels in
blood
- no hormone to store
glucose from food
intake into liver,
muscle, and fat cells
- Body can't
produce insulin
- Diagnosis
- Glycated hemoglobin A1C >= 6.5
- If A1C not available or
pregnant
- Random blood sugar test
or a 75 g oral glucose
tolerancetest >= 11.1
mmol/L
- Fasting blood sugar
test >= 7 mmol/L on 2
separate tests
- Check for symptoms of
polyphagia, polydipsia,
and polyuria
- Ketone test to
confirm type 1,
not type 2
- Ketone test to
confirm type 1,
not type 2
- Check for symptoms of
polyphagia, polydipsia,
and polyuria
- Random blood sugar test
or a 75 g oral glucose
tolerancetest >= 11.1
mmol/L
- If A1C not available or
pregnant
- Glycated hemoglobin A1C >= 6.5
Recursos multimedia adjuntos
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
¿Quieres crear tus propios Mapas Mentales gratis con GoConqr? Más información.