7327782
Descripción
Mapa Mental por jessica malia, actualizado hace más de 1 año
|
|
Creado por jessica malia
hace casi 8 años
|
|
John Bowlby (1907-1990)
- Defintion
- AB: ‘any form of behaviour that results in a person attaining or
maintaining proximity to some other clearly identified individual who is
conceived as better able to cope with the world. It is most obvious
whenever the person is frightened, fatigued, or sick, and is assuaged by
comforting and caregiving’ (Bowlby, 1982: 668).
- strong emotional bond (infant & caregiver)
- AB: ‘any form of behaviour that results in a person attaining or
maintaining proximity to some other clearly identified individual who is
conceived as better able to cope with the world. It is most obvious
whenever the person is frightened, fatigued, or sick, and is assuaged by
comforting and caregiving’ (Bowlby, 1982: 668).
- History
- Psychoanalytical
- normal resolution of the
oral stage of psychosexual
dev - oral needs (e.g.
sucking) are met
- normal resolution of the
oral stage of psychosexual
dev - oral needs (e.g.
sucking) are met
- Behavioural
- formed through
reinforcement: food
=PR -> associated
with mother = SR
- formed through
reinforcement: food
=PR -> associated
with mother = SR
- Psychoanalytical
- 1940
- maladjusted’ children, who were
affectionless and prone to
stealing and traced their
symptoms to histories of
maternal deprivation and
separation.
- maladjusted’ children, who were
affectionless and prone to
stealing and traced their
symptoms to histories of
maternal deprivation and
separation.
- 1948 (with J Robertson)
- observed the distress
hospitalised children
separated from their
parents experienced
(protest, despair and
detachment) = WHO
report (1951).
- observed the distress
hospitalised children
separated from their
parents experienced
(protest, despair and
detachment) = WHO
report (1951).
- 1958
- first formal statement of attachment theory
- at birth, babies are
equipped with
species-characteristic
instinctual behaviours
that promote proximity
with a caregiver (e.g.
crying, smiling).
- infant able to discriminate between
people and direct these behaviours
appropriately. With development of
internal representations of principal
caregivers, infant can form
attachments.
- at birth, babies are
equipped with
species-characteristic
instinctual behaviours
that promote proximity
with a caregiver (e.g.
crying, smiling).
- Stage theory of attachment
- Pre-attachment: (0-2months) indiscriminate
social responsiveness
- Attachment in the making (1-6months)
orientation to social stimuli directed towards
one or more discriminated caregivers
- clear-cut attachment (6-30months)
maintenance of proximity to attachment
figures, separation protest and wariness of
strangers.
- Goal-corrected partnership (24-48months)
insight into the caregiver’s feelings & goals
leading to co-operative interaction &
partnership.
- Goal-corrected partnership (24-48months)
insight into the caregiver’s feelings & goals
leading to co-operative interaction &
partnership.
- clear-cut attachment (6-30months)
maintenance of proximity to attachment
figures, separation protest and wariness of
strangers.
- Attachment in the making (1-6months)
orientation to social stimuli directed towards
one or more discriminated caregivers
- Schaffer and Emerson (1964):60 infants (2-yrs)
measured separation protest & stranger anxiety. 1/2
showed 1st specific attachment between 6-8months,
Fear of strangers began about a month later (stage 2
& 3 of B’s theory). 18 months 87% had more than one
attachment figure; 75% had attached to the father,
mother was most commonly.
- role of the primary caregiver is to
provide a safe haven in the event of a
threat and a secure base from which to
explore the environment = basis for MA
theory
- Pre-attachment: (0-2months) indiscriminate
social responsiveness
- first formal statement of attachment theory
- Internal Working model
- From birth, the infant gradually construct
expectations of regularities in what happens to
them. They then organises these expectations
internally into ‘Internal Working Models’.
- (1969): a child’s attachment relationship with
their primary caregiver leads to the
development of an internal working model.
This internal working model is a cognitive
framework comprising mental
representations for understanding the world,
self and others. They can be of the physical
environment, of ourselves, of others, or of
relationships.
- Internal working models of the self and primary
caregiver have special significance (‘attachment
representations’): If the primary caregiver is
available and supportive, a working model of the
self as ‘lovable’ is constructed or, if the caregiver is
rejecting, the model of the self is constructed as
being unworthy. i.e. when your young, the way
others treat you influences how you see yourself.
- A person’s interaction with others is guided by
memories and expectations from their internal
model which influence and help evaluate their
contact with others (Bretherton, & Munholland,
1999). Around the age of three these seem to
become part of a child’s personality and thus
affects their understanding of the world and future
interactions with others (Schore, 2000).
- A person’s interaction with others is guided by
memories and expectations from their internal
model which influence and help evaluate their
contact with others (Bretherton, & Munholland,
1999). Around the age of three these seem to
become part of a child’s personality and thus
affects their understanding of the world and future
interactions with others (Schore, 2000).
- According to Bowlby (1969) the primary
caregiver acts as a prototype for future
relationships via the internal working
model. There are three main features of
the internal working model: (1) a model
of others as being trustworthy, (2) a
model of the self as valuable, and (3) a
model of the self as effective when
interacting with others
- It is this mental representation
that guides future social and
emotional behavior as the
child’s internal working model
guides their responsiveness to
others in general.
- It is this mental representation
that guides future social and
emotional behavior as the
child’s internal working model
guides their responsiveness to
others in general.
- Internal working models of the self and primary
caregiver have special significance (‘attachment
representations’): If the primary caregiver is
available and supportive, a working model of the
self as ‘lovable’ is constructed or, if the caregiver is
rejecting, the model of the self is constructed as
being unworthy. i.e. when your young, the way
others treat you influences how you see yourself.
- (1969): a child’s attachment relationship with
their primary caregiver leads to the
development of an internal working model.
This internal working model is a cognitive
framework comprising mental
representations for understanding the world,
self and others. They can be of the physical
environment, of ourselves, of others, or of
relationships.
- Bartholomew and Horowitz (1991)
model of adult attachment
- Securely: positive views of both self
and others, comfortable with either
intimacy or autonomy (Bartholomew
& Horowitz, 1991). like securely
attached infants
- Preoccupied: negative view of self and a
positive view of others, due to
inconsistent care giving.
- fearful attachment: negative views of both
self and others. socially avoidant because
they are fearful of their own vulnerability
in intimacy.
- Dismissing: positive view of self and a negative view of
others, due to earl unresponsive care.
- Dismissing: positive view of self and a negative view of
others, due to earl unresponsive care.
- fearful attachment: negative views of both
self and others. socially avoidant because
they are fearful of their own vulnerability
in intimacy.
- Preoccupied: negative view of self and a
positive view of others, due to
inconsistent care giving.
- Securely: positive views of both self
and others, comfortable with either
intimacy or autonomy (Bartholomew
& Horowitz, 1991). like securely
attached infants
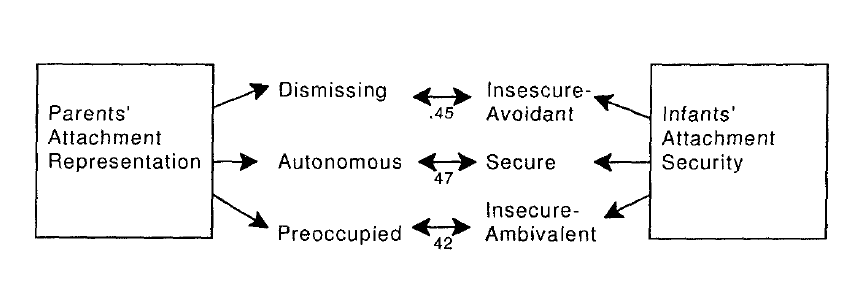
- Intergenerational continuity
- parent's early attachment experiences led to
their attachment style (dismissing, autonomous,
or preoccupied) which then influences their
parenting behaviour therefore influencing their
child’s attachment experiences and so on
- van Ijzendoorn (1995): meta-analysis of 18 studies =
correlation between parent’s attachment and
infant’s attachments.
- van Ijzendoorn (1995): meta-analysis of 18 studies =
correlation between parent’s attachment and
infant’s attachments.
- parent's early attachment experiences led to
their attachment style (dismissing, autonomous,
or preoccupied) which then influences their
parenting behaviour therefore influencing their
child’s attachment experiences and so on
- From birth, the infant gradually construct
expectations of regularities in what happens to
them. They then organises these expectations
internally into ‘Internal Working Models’.
- changing styles
- developmental outcomes are dependent on
entire history of experience, as well as current
circumstances, not just early care. Therefore,
you can create a secure attachment later in life
through others.
- Roisman et al (2002): 23yr & found that
individuals can overcome early negative
childhood experiences and develop secure
working models, referring to these as
‘Earned secure’ people.
- Scharf (2001): Israeli kibbutz = even in
childhood, internal working models can
change. This was shown through Children
who switched to family sleeping
arrangements aged between 3 and 6 years
showed no difference in attachment
representations from family-reared
adolescents.
- Roisman et al (2002): 23yr & found that
individuals can overcome early negative
childhood experiences and develop secure
working models, referring to these as
‘Earned secure’ people.
- developmental outcomes are dependent on
entire history of experience, as well as current
circumstances, not just early care. Therefore,
you can create a secure attachment later in life
through others.
- Biology
- 1969: believed that adult
attachment style remains linked to the
psychological and biological systems that
regulate threat appraisal, stress response,
and recovery from stress.
- Shaver and Mikulincer (2007):
Individuals high in attachment
anxiety are hyper-reactive to
threats, tend to report greater
levels of perceived stress, and
also are much more likely to
ruminate over the event
- Shaver and Mikulincer (2007):
Those high in attachment
avoidance are more likely to
employ defensive regulation
mechanisms, such as repression,
to allow them to control
unpleasant emotionally stressful
situations
- Shaver and Mikulincer (2007):
Those high in attachment
avoidance are more likely to
employ defensive regulation
mechanisms, such as repression,
to allow them to control
unpleasant emotionally stressful
situations
- Shaver and Mikulincer (2007):
Individuals high in attachment
anxiety are hyper-reactive to
threats, tend to report greater
levels of perceived stress, and
also are much more likely to
ruminate over the event
- 1969: believed that adult
attachment style remains linked to the
psychological and biological systems that
regulate threat appraisal, stress response,
and recovery from stress.
Recursos multimedia adjuntos
{kind=link}
{kind=link}
¿Quieres crear tus propios Mapas Mentales gratis con GoConqr? Más información.