773483
Clinical Child Psych Test 4
- Anxiety and OCD
- Social Anxiety Disorder
- DIAGNOSTIC CRITERIA
- A. Fear of social situations where they might be judged, observed, or must perform in front of others
- B.Fear that they will be embarrassed and rejected
- C. The social situations almost always provoke fear or anxiety
- expressed by crying, tantrums, freezing, clinging, shrinking, or failing to socially speak
- expressed by crying, tantrums, freezing, clinging, shrinking, or failing to socially speak
- D. Social situations avoided or endured with intense anxiety
- E. Fear or anxiety is out of proportion
- F. Fear/ anxiety/ avoidance lasts 6 months or longer, usually
- G. Anxiety causes setbacks in functioning
- H. Not attributable to any substance
- I. Not another mental disorder for sure
- J. Fear/ anxiety unrelated if the person has medical conditions
- A. Fear of social situations where they might be judged, observed, or must perform in front of others
- Child can speak but refuses to speak or speaks quietly, caused by fear or embarrassment
- Can be limited to performance situations only
- Treatment: exposure, knowledge through experience
- Treatment: exposure, knowledge through experience
- FEARS
Nota:
- Side note: you are most likely to perform well if you are not thinking about others watching you, it was just automatic
- Reading aloud
- Performance activities
- Eating with others
- Etc, but all this stuff happens all the time
- SOURCE --> inhibition system
- Over-controlling/protective parents
- Over-controlling/protective parents
- DIAGNOSTIC CRITERIA
- Panic Disorder
Nota:
- This should actually be under "Anxiety and OCD"
- DIAGNOSTIC CRITERIA
- Panic attacks reach their peak within 10 mins
- 4 plus symptoms occur
- Heart irregularities, sweating, trembling, can't breath, chest pain, nausea, dizzy or light-headed, chills/heat flashes, numbness/tingling, feels surreal, fear of losing control or dying
- Heart irregularities, sweating, trembling, can't breath, chest pain, nausea, dizzy or light-headed, chills/heat flashes, numbness/tingling, feels surreal, fear of losing control or dying
- And one of these two happens for the next month or more
- Fear of 2+ of these
- Public transportation
- Open spaces
- Enclosed spaces
- Standing in line / crowds
- Being away from home alone
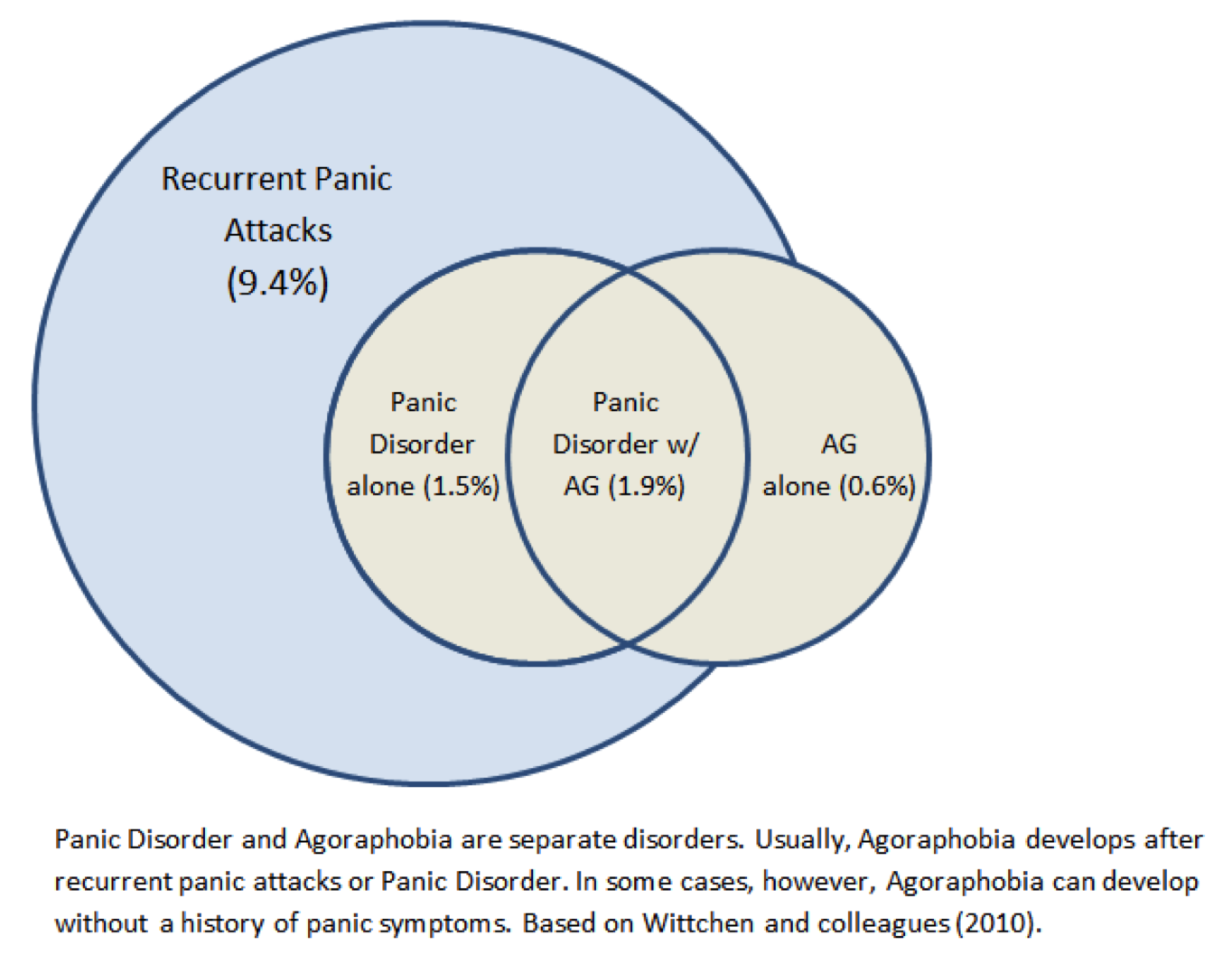
- (THESE ARE SYMPS OF AGORAPHOBIA, which is not the same as PD
- How might agoraphobia develop in terms of panic disorder?
- Negatively reinforced by avoiding situations in which they might have a panic attack
- Negatively reinforced by avoiding situations in which they might have a panic attack
- Public transportation
- Must be able to escape or be helped in a situation, in case they have a panic attack
- Agoraphobia
- Fear is excessive
- Persists for 6 months
- For sure to another mental disorder
- Fear of 2+ of these
- Panic attacks reach their peak within 10 mins
- You can have a panic attack without having panic disorder
- 1/3 of adults // 1/10 of children
- 1/3 of adults // 1/10 of children
- TYPES OF PANIC ATTACKS
- Type A: Calm>PANIC>Calm
- (Probs not PD yet)
- (Probs not PD yet)
- Type B: Calm>PANIC>Anxious
- Type C: Anxious>PANIC>Calm
- Type A: Calm>PANIC>Calm
- It becomes panic disorder when you start to fear panic attacks happening again
- Generalized Anxiety Disorder
- "kiddo" that worries about everything
- SYMPTOMS
- Tension, Apprehensive expectations, negative self-image, need for reassurance, irritability, physical complaints, concentration problems, brooding, fatigue, psychomotor agitation, sleep problems
- Tension, Apprehensive expectations, negative self-image, need for reassurance, irritability, physical complaints, concentration problems, brooding, fatigue, psychomotor agitation, sleep problems
- THINGS THEY WORRY ABOUT THE MOST IN ORDER
- Health of others
- Family matters
- The little things
- School
- Self health
- Health of others
- Reassurance seeking > negative reinforcement rapidly throughout the day
- Internalizing Symptoms
- Anxious-Misery Symptoms (last a long time)
- Major Depressive Disorder
- Dysthymic Disorder
- GAD
- Major Depressive Disorder
- Fear Symptoms (symptoms occur abruptly and then go away and may only occur in certain situations)
- Specific Phobia
- Social Phobia
- Agoraphobia
- Panic Disorder
- Specific Phobia
- Anxious-Misery Symptoms (last a long time)
- Worrying + Problem Solving = Normal
- Worrying + Rumination = GAD
- (rumination is usually past oriented)
- (rumination is usually past oriented)
- "kiddo" that worries about everything
- OCD
- Compulsion: ex-washing/grooming
- Repetitive behaviors/thoughts to prevent anxiety or a dreaded event--won't realistically prevent or neutralize
anything
- but the compulsion doesn't have to fix the obsession in a sensible way
- Repetitive behaviors/thoughts to prevent anxiety or a dreaded event--won't realistically prevent or neutralize
anything
- Obsession: ex-germs
- often related to religion or sexual imagery
- 1. Persistent thoughts, urges, images that come as intrusive thoughts and cause anxiety
- 2. Attempts to ignore the thoughts and to neutralize them with another thought/action
- often related to religion or sexual imagery
- trying to ignore an intrusive thought = a compulsion
- DIAGNOSTIC CRITERIA
- A The presence of obsessions, compulsions, or both:
- B. Time consuming / Impairs functioning
- C. Not the result of drugs
- D. For sure not another mental disorder
- A The presence of obsessions, compulsions, or both:
- Classifying OCD
- With good or fair insight
- realizes beliefs are probe not true
- realizes beliefs are probe not true
- With poor insight:
- Thinks beliefs are probe true
- Thinks beliefs are probe true
- With absent insight:
- Completely convinced of beliefs
- Completely convinced of beliefs
- Tic-related:
- history of tic disorder
- history of tic disorder
- With good or fair insight
- Comorbidity with ASD
- Disregulation of the cortico-stratial-thalamic circuit
- Compulsion: ex-washing/grooming
- More Information
- Well-learned tasks are performed better in front of an audience
- Poorly learned tasks are performed even more poorly
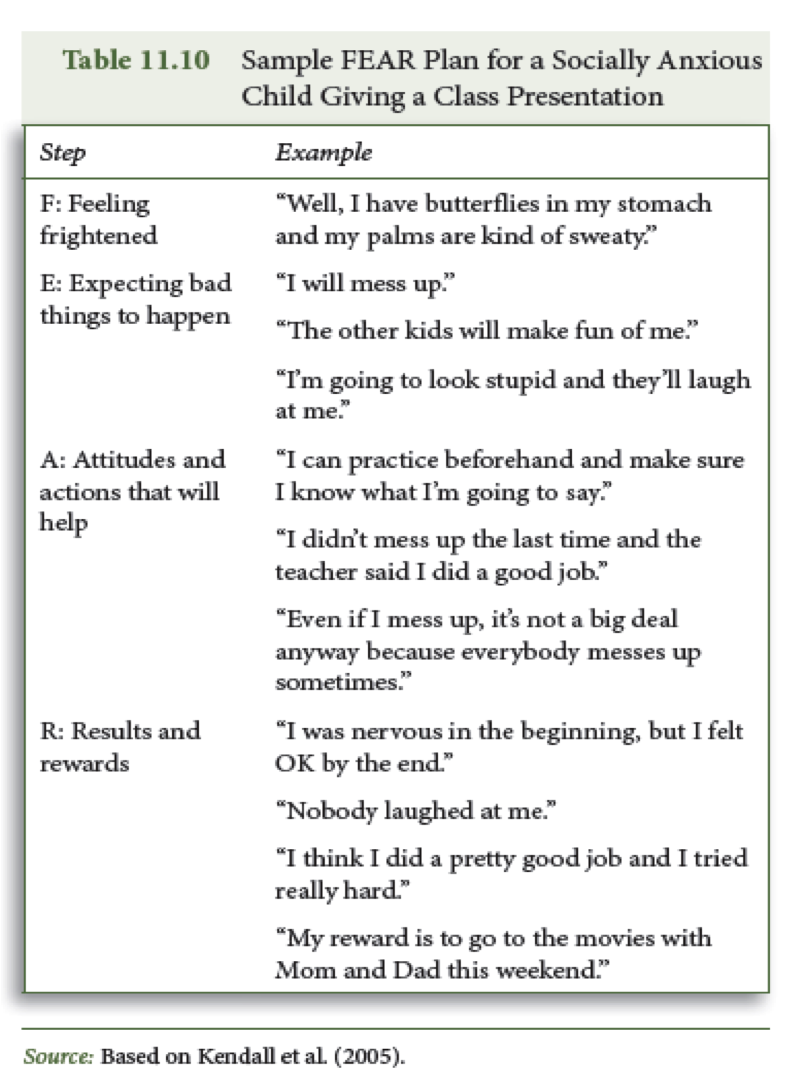
- FEAR Plan
- CBT for Parent and Child is the most effective treatment
- CBT and Sertraline (meds) do not work as well to relieve anxiety alone as they do together, but anything is better that a placebo
- Well-learned tasks are performed better in front of an audience
- Social Anxiety Disorder
- Focus on cognitive and behavioral symptoms!
- Trauma and Child Maltreatment
- PTSD
- DIAGNOSTIC CRITERIA (2+ primary criterion)
- Behavioral
- Cognitive
- Intrusion Symptoms - one or more
- Distressing memories
- Distressing dreams
- Flashbacks
- Physiological reactions to internal cues
- Distressing memories
- Intrusion Symptoms - one or more
- emotional
- physiological
- Alterations in arousal and reactivity
- Angry outbursts
- Reckless/self-destructive
- Hypervigillance
- Exaggerated startle response
- Concentration Probs
- Sleep disturbances
- Angry outbursts
- Alterations in arousal and reactivity
- trauma
- sexual trauma
- REQUIRED for PTSD diagnosis
- sexual trauma
- Exposure - one or more
- Direct experience
- Witnessing
- Learning about event involving fan member / friend
- Repeated exposure to details
- Internal or external cues cause distress
- Internal or external cues cause distress
- Children are more likely to have PTSD symptoms/ PTSD if they are directly exposed to a traumatic event (>indirect>no exposure)
- Direct experience
- Persistent Avoidance
- Negative alterations in cognitions and mood
- Amnesia
- Negative beliefs about oneself, others, or the world
- Detachment from others
- Detachment from others
- Blaming oneself
- Negative emotional state
- Lack of interest in activities
- Inability to be happy
- Amnesia
- Duration of disturbance > 1 month
- Disrupts normal functioning
- Behavioral
- Critical Incidence Stress Debriefing > not helpful
- not due to substance or medical condition
- Cortisol reduces the size of the hippocampus in large qualities (depression)
- DIAGNOSTIC CRITERIA (2+ primary criterion)
- Child Abuse
- Definition
- Harm Standard:failure to act on the part of caregiver, results in death/physical/emotional harm/sexual abuse/exploitation
- Endangerment Standard: act/failure to act that presents risk of serious harm
- Harm Standard:failure to act on the part of caregiver, results in death/physical/emotional harm/sexual abuse/exploitation
- Symptoms in order of how common they are
- Avoidance of people/places
- Irritability and tantrums
- Sleep disturbance/Distress from reminders
- Avoidance of people/places
- GENERAL MALTREATMENT STATISTICS
- Over 900,000 children victims of maltreatment in 2006
- 12.1 per 1000 children in general population
- Nearly 3.6 million received investigation
- Over 900,000 children victims of maltreatment in 2006
- CHARACTERISTICS OF FAM / PERPETRATOR
- Low SES
- Single parent / large household
- Parents - 85%
- Sexual abuse: 50% parents, 50% not
- Neglect: 90% mothers
- Low SES
- Definition
- Six Types of Psychological Abuse
- Spurning - reject/degrade child
- Terrorizing - threatening
- Isolating - no interaction w peers
- Exploiting - encourage antisocial acts, transport drugs, porn, prostitution
- Denying emotional responsiveness
- Health and educational neglect
- Spurning - reject/degrade child
- Common Types of Maltreatment (Greatest->least)
- Any maltreatment
- Physical Abuse
- toddlers, preschoolers, young adults, boys=girls
- toddlers, preschoolers, young adults, boys=girls
- Physical Abuse
- Neglect
- children 1-3
- children 1-3
- Sexual abuse
- 12 or older, 80% girls
- 12 or older, 80% girls
- Psychological abuse
- toddlers, preschoolers, young adults
- toddlers, preschoolers, young adults
- Any maltreatment
- PTSD
- Depressive Disorders
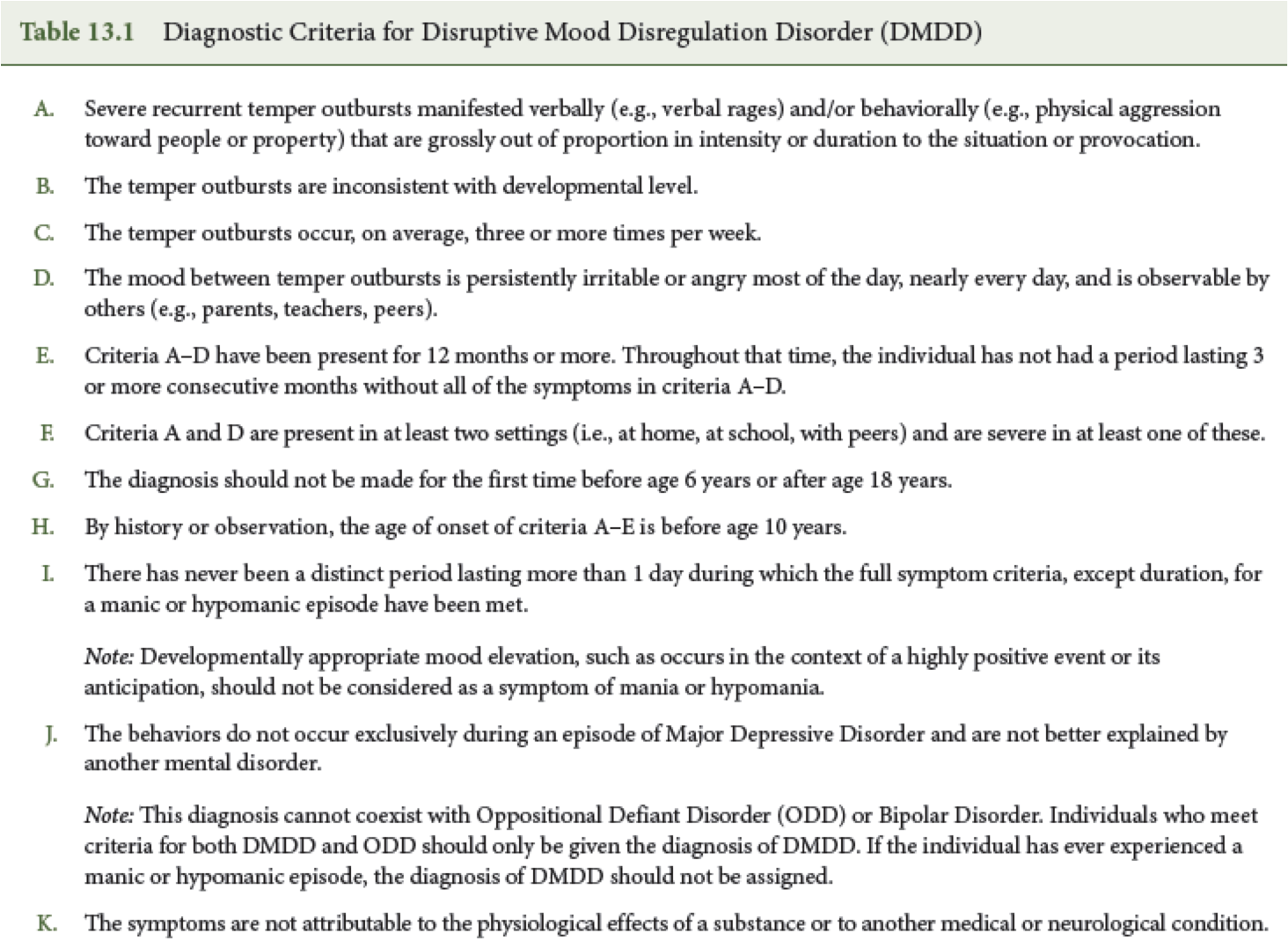
- Disruptive Mood Disregulation Disorder (temper tantrum disorder)
- Cannot coexist with ODD or bipolar disorder--if they are diagnosed with both, they really just have DMDD
- are more likely to develop depression (1.3-1.8 times more likely) or anxiety (1.7), but not bipolar disorder
- More activity in Anterior Cingulate Cortex and Medial Frontal Gyrus
- Risperdall seems to treat it, but there was no control group
- Cannot coexist with ODD or bipolar disorder--if they are diagnosed with both, they really just have DMDD
- PRIDE SKILLS (parent child interaction therapy)
- labeled praise
- Reflection / praise
- Immitation
- Description
- Enthusiasm
- labeled praise
- HOW TO SOLVE PROBLEMS
- survey options
- brainstorm solution
- Evaluate Choices
- Select one
- Impliment it
- Monitor outcome
- survey options
- Major Depressive Disorder
- symptoms must last for at least 2 weeks
- There has never been a manic/hypomanic episode
- Disrupts regular functioning
- There has never been a manic/hypomanic episode
- Must have 5 of these symptoms
- ANHEDONIA- absence of seeking pleasure
- irritable/sad mood nearly every day, most of the day
- weight or eating disregularity
- sleeping probe nearly every day
- noticeably restless or slow
- Worthlessness / guilt
- Fatigue
- hard time concentrating
- thoughts of death
- ANHEDONIA- absence of seeking pleasure
- Categorizing it...
- Single episode: situational depression
- Recurrent: 2+ depressive episodes with 2 month in between
- Mild: few and mild symptoms
- Severe: a lot of severe symptoms
- Single episode: situational depression
- DSM IV -- if you recently lost a loved one, you don't have depression
- DSM V -- you can be diagnosed with depression (self-fulfilling prophecy)
- Cognitions that contribute to depression
- Catastrophizing - expecting something bad to happen
- Overgeneralization - thinking because one situation happens, it applies to all situations
- ex: he broke up with me, I will always be single
- ex: he broke up with me, I will always be single
- Dichotomus thinking - something is either all good or all bad
- Mind reading- or thinking you can
- Personalization - taking responsibility for something that's not your fault
- Absolute thinking - "I must" "I should" "I have to"
- Catastrophizing - expecting something bad to happen
- People with depression have the most Personal Failure Automatic Thoughts (then anxiety, behavior problems)
- Treatment: Prozac, but the best treatment is CBT only and CBT is more effective over the long term
- Tricyclics are not effective
- SSRI's increase suicidal ideation and are less effective over time
- symptoms must last for at least 2 weeks
- Bipolar Spectrum Disorder
- Manic Episode (BIPOLAR 1)
- must have 3 or more of these symptoms and last one week
- inflated self-esteem
- no need for sleep
- talkative
- racing thoughts
- distractibility
- goal oriented
- activities with consequences
- inflated self-esteem
- usually lasts 1-4 weeks
- must have 3 or more of these symptoms and last one week
- Hypomanic Episode (BIPOLAR 2)
- about 4 days
- slightly better than Manic Episodes, because they don't last as long
- about 4 days
- Cyclothymic Disorder
- 2 symptoms of mania / hypomania, 3 symptoms of depression, for 2 years
- Can't go without symptoms for 2 months
- 2 symptoms of mania / hypomania, 3 symptoms of depression, for 2 years
- 70% thoughts of death
- and just read the slides after this....
- Manic Episode (BIPOLAR 1)
- Disruptive Mood Disregulation Disorder (temper tantrum disorder)
Recursos multimedia adjuntos
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
¿Quieres crear tus propios Mapas Mentales gratis con GoConqr? Más información.