11900771
Description
Flashcards by Ellie Britt, updated more than 1 year ago
|
|
Created by Ellie Britt
almost 7 years ago
|
|
| Question | Answer |
| Targets for injury in the nephron | - Mesangial cells (secrete matrix) - Basement membrane (collagen IV) - Epithelial cells (podocytes) - Capillary endothelial cells - Vasculature. - Tubular structures. - Integrity of glomerulus and tubules |
| extrinsic and intrinsic mechanisms of glomerulonephritis | EXTRINSIC Antibodies. Immune complexes. Complement. Cytokines. Lymphocytes Other infiltrating cells. INTRINSIC Cytokines. Growth factors. e.g. TGF-beta, PDGF, IFN-gamma. e.g. Vasoactive factors. Proteinuria. |
| Kidney biopsy - why - how examined | Required for clinical diagnosis of glomerulonephritis Biopsy of kidney cortex examined under - Light microscopy (glomerular and tubular structure) - Immunofluorescence (looking for Ig and complement) - Electron microscopy (glomerular basement membrane and deposits) Many diseases are a clinical and pathological spectrum |
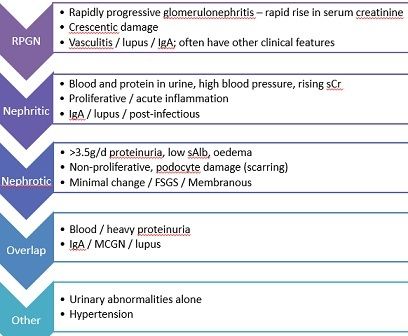
| Subtypes of glomerulonephritis (5) |
Image:
Glom (binary/octet-stream)
|
| Nephrotic syndrome - 4 features - types - risks | - 3.5g proteinuria per 24h (urine PCR >300) - Serum albumin <30 - Oedema - Hyperlipidaemia Non-proliferative, podocyte damage (scarring) Minimal change / FSGS / Membranous Risk of venous thromboembolism Increased risk of infection |
| Nephritic - features - causes | Blood and protein in urine, high blood pressure, rising sCr Proliferative / acute inflammation IgA / lupus / post-infectious |
| RPGN - features - causes | Rapidly progressive glomerulonephritis – rapid rise in serum creatinine Crescentic damage Vasculitis / lupus / IgA; often have other clinical features |
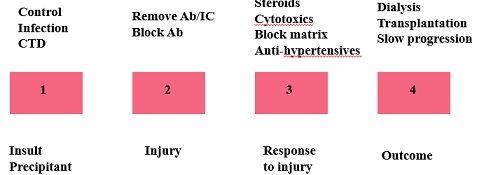
| Glomerulonephritis model and possible therapeutic strategies |
Image:
Model (binary/octet-stream)
|
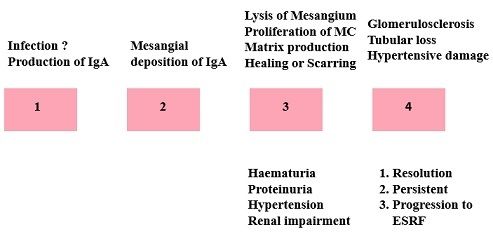
| pathophysiology of IgA nephropathy |
Image:
Iga (binary/octet-stream)
|
| IgA nephropathy - epidemiology - secondary to? | The most common primary glomerular disease. Up to 1% of the “normal” population. Precipitated by infection? Synpharyngitic May be 2° to HSP, cirrhosis, coeliac disease. |
| IgA nephropathy - pathology - clinical features | Abnormal/ over-production of IgA1, IgA I/C. Mesangial IgA, C3 deposition. Mesangial proliferation. Tubular atrophy/interstitial fibrosis Haematuria. Hypertension. Proteinuria (varies with prognosis) |
| IgA nephropathy - progression - predictors of progression - therapy | About 1/3 progress to ESRF. 10% at 10 years, 20% at 20 years …….. Predictors of ESRF- uPCR, sCr at diagnosis, BP. No specific therapy. Antihypertensive Rx, ACE inhibitors. |
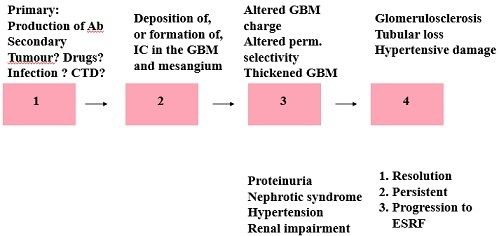
| Pathophysiology of membranous GN |
Image:
Gn (binary/octet-stream)
|
| Epidemiology and aetiology of membranous GN | A disease of adults. Presents with the nephrotic syndrome – commonest primary cause. 10% secondary to malignancy, CTD, drugs |
| Pathology and progression of membranous GN | Anti-phospholipase A2 receptor antibody in 70% Immune Complexes in basement membrane/ sub-epithelial space. IC deposited (preformed) or formed in situ. Variable natural history. A third spontaneously remit. A third progress to ESRF over 1-2 years. A third persistent proteinuria, maintain GFR. |
| How to treat membranous nephropathy? | 1. Treat underlying disease if secondary 2. Supportive non-immunological – ACEi, statin, diuretics, salt restriction 3. Specific immunotherapy - Steroids - Alkylating agents (cyclophosphamide) - Cyclosporin - Alternatives– rituximab, anti-CD20 MAb Outcomes – Complete remission, partial remission, ESRD, relapse, death. |
| Minimal Change Disease - who - causes what - pathogenesis - cause | The commonest form of GN in children. (90% of GN < 10 years, 20% of adults of all ages.) Causes the nephrotic syndrome. EM - foot process fusion. Pathogenesis - T cell, cytokine mediated. Target glom. epithelial cell, GBM charge Idiopathic but may be 2° to malignancy |
| Minimal change disease - presentation - GFR - outcome | Acute presentation - may follow URTI. GFR - normal, or reduced due to intravascular depletion. Very rarely causes renal failure. Relapsing course (50% will relapse). |
| Treatment of minimal change disease | 1. High dose steroids. Prednisolone 1mg/Kg for up to 8 weeks. Failure to respond, consider FSGS 2. Cyclophosphamide / calcineurin inhibitor |
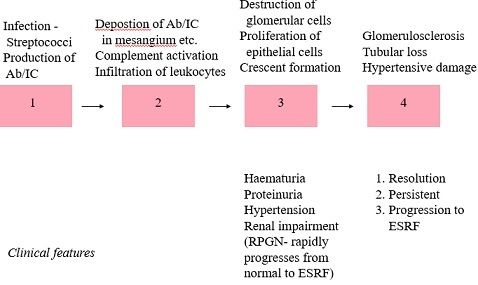
| Pathophysiology of post-infectious GN |
Image:
Pign (binary/octet-stream)
|
| post-infectious GN - cause - pathology | Usually post-streptococcal type 12, gp A strep. Production of Ab (cross-reactive) and I/C. Sub-epithelial I/C deposition. Complement consumption and hypocomplementaemia. Days after URTI (10-21) – latent period Oliguric ARF. Haematuria, variable proteinuria, oedema. Hypertension. Urinary red cell casts. |
| outcome of post-infectious GN | Proliferation of all glomerular cells, crescents. Infiltrating cells. Resolves over weeks in most cases. May require dialysis. Antibiotics? no other specific therapy. The prognosis is usually, but not always, benign. |
|
Image:
Cresc (binary/octet-stream)
|
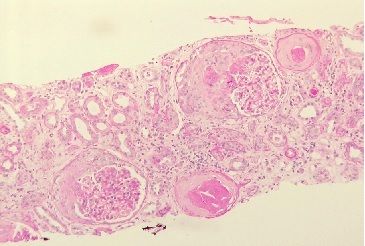
crescentic disease |
| Crescentic GN/RPGN - histology - progression | A group of conditions linked by natural history/ histology. Crescents on biopsy. Progression to ESRF over a few weeks, untreated high mortality. |
| common causes of crescentic GN/RPGN | - Goodpastures syndrome – Anti-GBM antibody. - Pauci-immune: Microscopic polyangiits – MPO antibody (positive pANCA) Granulomatosis with polyangiitis (GPA) – PR3 antibody (positive cANCA) - Post infectious/ bacterial endocarditis. - Lupus. - Idiopathic. - Rarely others e.g. IgA nephropathy. |
| Tests in renal disease (and associated diseases) | HbA1c/random glucose (diabetic nephropathy) ANCA/anti-GBM (vasculitis) ANA/PLA2R/virology (membranous) complement/ANA/dsDNA (lupus) complement/virology (hep BC, HIV)/Igs/RF (MPGN, FSGS) SEP/BJP/SFLC (amyloid/light chain deposition (myeloma) |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.