13861128
Description
Flashcards by Aizza Memon, updated more than 1 year ago
|
|
Created by Aizza Memon
over 6 years ago
|
|
| Question | Answer |
| What is an allergy? | 2 parts: 1) initial exposure 2) subsequent exposure allergen is anything than cause a response eyes are prone to allergy- (exposed to environment, conjunctiva is highly vascular, conjunctiva large SA) |
| Types of hypersensitivity reactions | type 1- immediate/ anaphylactic 95% of hypersensitivity reactions are type 1 type 2- cytotoxic ( autoimmune) type 3- immune complex type 4- cell mediated ( delayed) |
| Type 1 hypersensitivity reaction examples | Vernal Conjuctivitis Seasonal allergic Conjuctivis - hayfever Perrenial allergic Conjuctivis - anytime of year dust etc Atopic Keratoconjuctivitis |
| Allergic Conjunctivitis SAC PAC | Seasonal allergic conjuctivitis during season eg hayfever Perrennial allergic conjuctivitis occurs all year round dust mites etc Symptoms: itching, redness, oedema IRO usually bilateral |
| Vernal Keratoconjuctivitis VKC | usually in males, late 20s, more common in warmer climates Symptoms: -tranta dots -THICK MUCOID DISCHARGE -severe itching -papillae on upper eye lid -photophobia -punctate keratitis |
| Atopic Keratoconjuctivitis AKC | usually present in people who have eczema perennial disorder Symptoms: -severe itching - CLEAR THIN WATERY DISCHARGE -photophobia -papillae on upper eyelid -punctate keratitis - SHIELD SHAPED CATARACT DEEP CORNEAL NEOVASC |
| TYPE 1 reaction 2 stages: 1) initial sensitisation 2) subsequent exposure | 1) initial sensitisation- the allergen binds to allergen presenting cell ( APC) and causes it to attract T helper cells. Lipotryins causes B cells to produce antibodies( IgE) and circulates them into the blood stream and the area of the lympathic vessel. Mast cell is in the conjuctiva 2) the allergen binds to the receptor on the mast cells which causes the mast cells to degranulate and release antihistamines and other chemical mediators. causes VASODILATION AND ENDOTHELIAL GAPING AND FLUID LEAKAGE- oedema GOBLET CELLS MUCOUS SECRETION ACTS ON NERVES- ITCHING |
| Histamine receptors | H1 - H4 H1 and H4 most important in allergy H1 causes contration vasodilation SMOOTH MUSCLE BLOOD VESSELS H4 can be present on mast cells degranulated |
| Type 2 and type 3 hypersensitivity | Type 2 antibodies, antigen is cell surface, minutes to hrs, cell lysis Type 3 antibodies, SOLUBLE, 3-8hrs, Stephen Johnson Syndrome, Rhuematoid artheritis |
| Type 4 hypersensitivity | Cell mediated- t cells, nuerophils, macrophages chemical mediators such as cytokines, interleukins, prostaglandins produce inflammatory response DELAYED TAKES 48-72 HRS for the inflammatory cells to build up Giant papillary conjuctivitis, uveitis, herpes simplex |
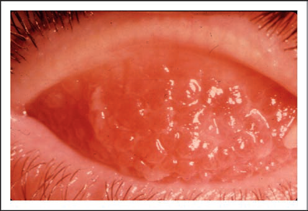
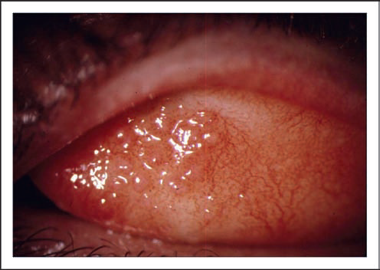
| Giant Papillary Conjuctivitis |
Usually due to CL wear
can be due to friction/ trauma
more commonly due to allergic reaction to protein deposits on CL surface
bumps on conjuctiva
TYPE 4- inflammatory response
Image:
Gpc (binary/octet-stream)
|
| Astringent eye washes and drops | provide temporary relief in very mild irritation effectively wash the allergen out does it doesnt cause an allergic response 0.9% saline solution Optrex eye drops: benzalkonium chloride GSL witch hazel |
| Ocular decongestants | vasoconstrictor slows down the release of chemical mediators to the conjunctiva from the bloodstream. Decreases the access of chemical mediators in the eye. the blood vessels constricting, counteracts the vasodilation, redness, oedema caused by histamine and other chemical mediators. NO DIRECT RESPONSE TO ALLERGN CAN BE USED WITH ANTIHISTAMINES AND OTHER OCULAR DRUGS SYMPATHOMIMETIC Alpha 1 adrenreceptor adrenaline used to be one not anymore |
| Ocular decongestants examples and problems | NaphAZOLINE OxymetAZOLINE - longer duration phenylephrine - NOT ALLOWED adrenaline used to be P DRUG- bought over counter transient stinging , blurred vision, dilation, rebound congestion( when you stop using them then symptoms come back worse prolonged used) NO HBP MEDS as HBP could occur |
| Antihistamines | H1 receptor antagonists, block histamine binding to receptor and therefore triggering response (reduced redness, swelling and pain) NOT COMPLETE RELIEF AND OTHER H RECEPTORS INVOLVED AND OTHER CHEMICAL MEDIATORS |
| Antihistamines how do they work? examples | allergen binds to IgE antibody receptor. there is a release of histamine however it does not bind to blood vessels ( block receptors) ANTAZOLINE- weakest one short max duration combined with decongestant shouldnt use for long periods of time KETOIFEN OLAPATADINE- dual action antihistamine + mast cell stabiliser |
| Examples of dual action antihistamine and mast cell stabilser | Olapatadine Ketoifen prevents histamine and other chemical mediators being released. Prevents FCR1 from being activated immediate relief SAC NOT TO BE USED FOR UNDER 3 |
| antihistamine problems | transient stinging- pH of the drop contains preservatives- aggravate symptoms mydriasis and blurred vision if it causes irritation it can cause histamine to be released |
| Mast cell stabiliser | stabilise mast cells --> inhibits the influx of Ca 2+ ions across the membrane --> prevents degranulation of mast cell --> stop histamine release --> stops the release of other chemical mediators NEEDS TO BE USED CONTINUOUSLY TO MAKE SURE ALLERGIC RESPONSE DOESNT occur. aint treating the root cause ygm takes days before effects are evident, take it before symptoms arise |
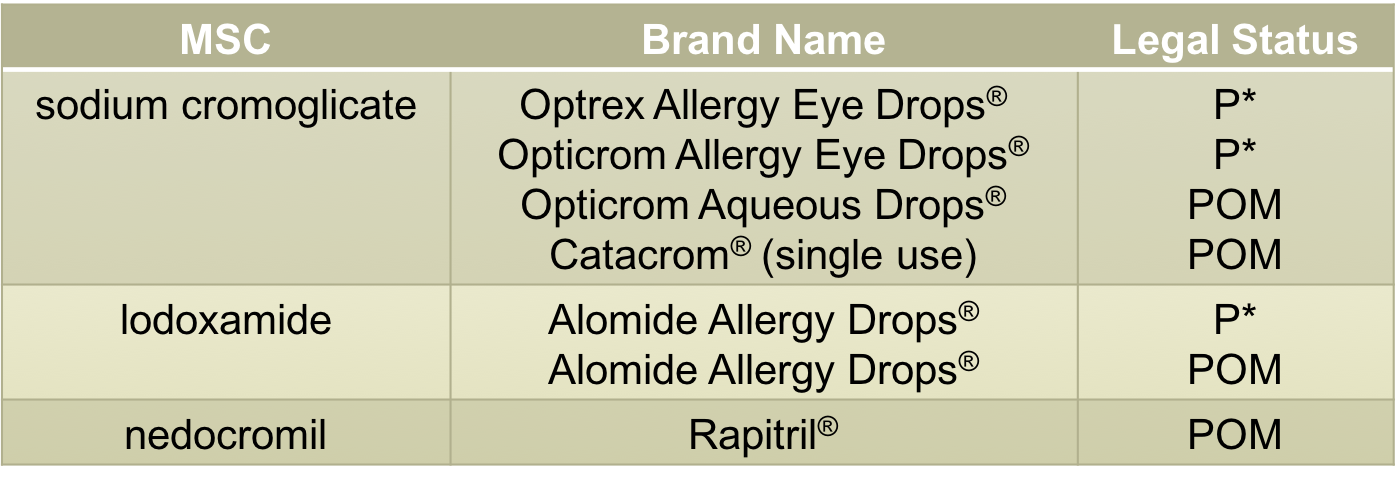
| Mast cell stabiliser examples | SODIUM CROMAGLICATE- cheaper P* SAC and PAC lodoxamide, nedocromil faster onset minimum age 4yrs |
| Mast cell stabiliser indications problems | GSL/P -SAC/PAC POM- VKC or AKC MCS more for severe ocular symptoms not to be used for children under 3 99 problems mast cells aint one transient burning - pH contains preservatives- aggrevate symptoms well tolerated -heart problems dont give them this |
| oral antihistamines | main indication are when symptoms are predominantly non ocular chlorphenaMINE- sedating loratadINE - can cause dry eye cardiac arrythmias ( terfenadINE taken off market, fexofenaDINE) grape fruit |
| what is inflammation? | -normal physiological response to defend body from attack - inflammation in the eye can result in permanent loss of vision ( scar formation and damage) born with it baby DONT REQUIRE IMMUNOLOGIC MEMORY, QUICK ONSET,automatic response first youre in contact trauma eg corneal abrasion ( physical damage) immunogenic inflammation eg bacterial conjuctivitis neurogenic inflammation- toxic substances release neuropeptides eg onions |
| stages of inflammation | Acute inflammation acute vascular response- provides cells with access to the site acute cellular response- sends signals to other white blood cells and other chemical mediators to come to the area chronic cellular response- appearance of mononuclear cells ( macrophages, lympthcytes) tissue will start to repair sometimes you get an exeggerated response and scarring can occur. Sometimes it goes wrong and the cycle continues CHRONIC INFLAMMATION |
| components of inflammatory response | H C C humoural- series of proteins that work together chemical- chemical mediators that amplify up the inflammatory response eg prostanoids, leukotrienes cellular- Wbc's help release other chemical mediators engulf pathogen |
| signs of inflammation | pain loss of function oedema redness |
| How are chemical mediators synthesised? | inflammatory response --> activates phospholipase which breaks down Arachidonic acid into LIPoxygenases --> luekotrienes and CYCLOoxygenases --> prostaglandins |
| Prostaglandins | synthesised by cyclooxygenases PGs - MAIN IS PGE2 & PG F2 not just for inflammation but you get an influx when inflammation occurs. - produces mucus - prevention of thrombosis |
| COX enzymes | cox 1- most prominent and responsible for physiological roles ( chronic pain) cox 2- they needed to be produced more for certain functions, present in low levels in normal( INFLAMMATION important) |
| NSAIDS- inhibit the PG synthesis | inhibits the enzyme prevents the arachidonic acid being broken into prostaglandins. NSAIDS inhibit COX1 but also COX2 - still get leukotrienes, cellular mediators stimulated upstream inhibit the PG= reduce inflammatory response! PG- causes redness, oedema, PAIN |
| example of topical NSAIDS | DiclofeNAC Voltarol trade name severe SAC intra/post operative surgery -POM - level 2 optometrist./IP |
| Systemic NSAIDs | ONLY AVAILABLE ORAL -same mechanism of action, wont cross in the eye enough - COX1 AND COX2 inhibition - extraocular muscles or around the eyes can use systemic NSAIDS e.g. aspirin, ibuprofen, diclofenac problems: GI bleeding./ ulcer thrombosis - increased bleeding bronchoconstriction- AA diverted to increase luekotriene synthesis NO ASTHMATICS majority of NSAIDS inhibit cox 1 and cox 2 if we just inhibit cox 2 more specific response with less side effects however have cardiovascular events, skin reactions eg CELECOXIB, ETORCOXIB helps with reducing pain analgesic fever antipyretic |
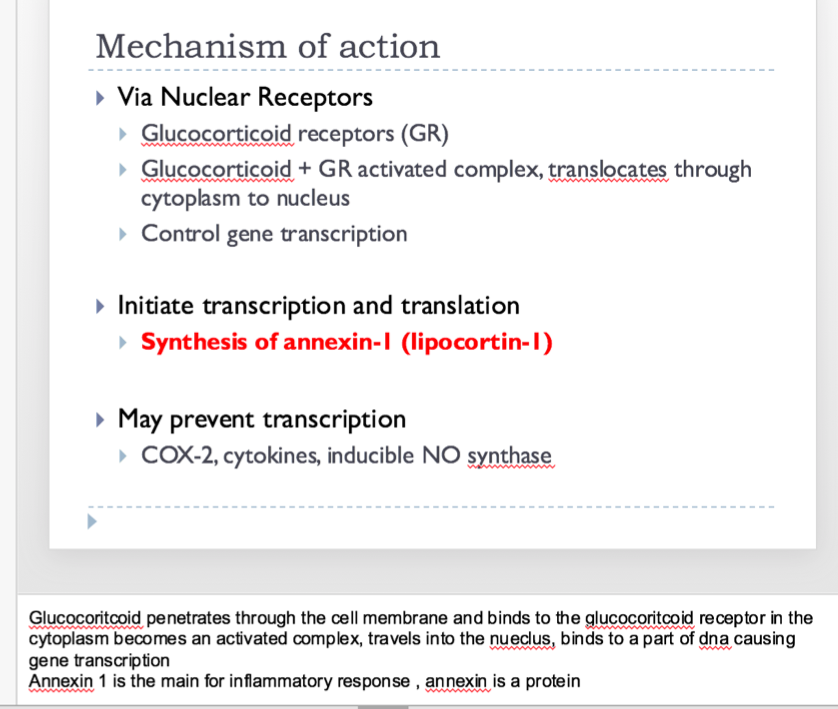
| anti inflammatory action of corticosteroids SAIDS |
inflammatory stimulus--> corticosteroids SAIDS inhibits the phosopholipase a2 being produced basically stops nothing else being produced ( prostaglandins and leukotrienes)
- stops it earlier in the pathway than NSAIDS
-decrease permeability of blood vessels so less wbcs into the area
- prevents T and B cells
tends to be used when NSAIDS not helping
for more SEVERE THINGs
Image:
Saids (binary/octet-stream)
|
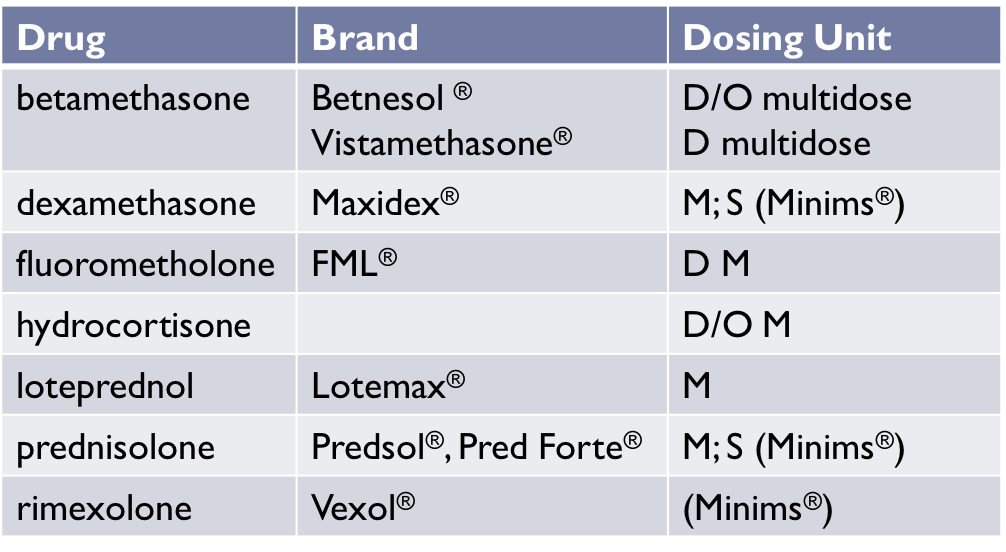
| TOPICAL SAIDs | topical steroids vary in ability to pentrate the cornea ACETATE ( suspensions) ALCOHOL PHOSPHATE SALT HYDROCHLORIDE ( solutions) low lipophilicity immediate treatment- has to be administered very frequently at first then lower it. Continue use for a few days after to make sure we have got rid of chemical mediators long term- side effects Topical steroid Inflammation of the eyelid, conjunctiva, cornea, iris, ciliary body Topical + periocular injection / systemic steroid- Severe anterior uveitis (unresponsive to topical alone) Systemic steroid- Inflammation of the optic nerve, posterior segment or orbit |
| topical SAIDS examples | POM hydrocortisone, prednisolone ONE problems- stimulating the trabecular meshwork clogs up the TB decreased outflow --> increase in IOP ( more than a week) cataract formation-higher dose SYSTEMICALLY prevents wound healing- orally for about 10 days withdrawal can interfere with natural corticosterioid production REBOUND INFLAMMATION systemic higer risk of side effects |
| other inflammation measured | MYDRIATICS in uveitis relieves pain by immobilising the iris, prevents adhesion of the iris to the cornea antimuscarinics phenylephrine |
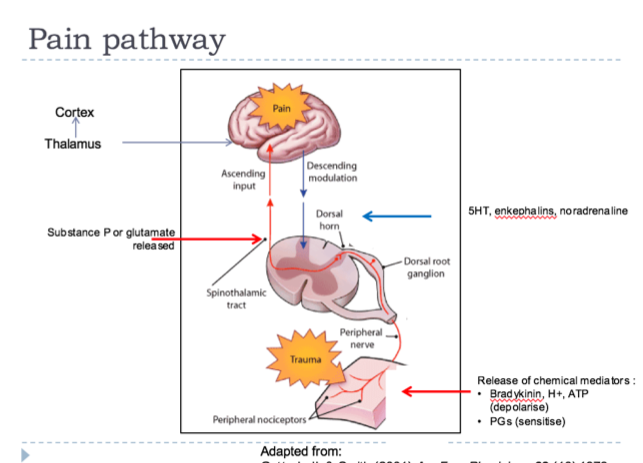
| pain pathway |
trauma to any tissue or organ travels via peripheral nerve to the dorsal ganglion -- >synapes with other nerves to higher areas of the brain --> thalmus --> cortex
asscending pathway that comes back down to stop it so we feel less pain
NSAIDS- good at reducing pain at the local level
Opoids-not as good at local level more at the level of the brain
Image:
Pain (binary/octet-stream)
|
| ocular pain pathway | trigeminal nerve --> trigeminal nucleus( brain stem) --> thalmus --> somatosensory cortex corneal representation can get pain from skin innervated by similar nerves |
| Pyresis | interleukin are released from leukocytes --> can cause increase in prostaglandin synthesis --> PGE2 raises temp in thermoregulatory centre in HYPOTHALMUS --> core temp is senses as too low --> increased heat gain |
| Pyresis V hyperthermia | hyperthermia core themostat not increased heat producted greater than heat loss feel hot the thalmus hasnt been affected hot hot hot pryresis core thermstat increased by prostaglandins ( CONSERVING HEAT) heat production and heat loss balanced feel cold |
| paracetamol v NSAIDS | paracetamol analgesic anti pyretic NOT GOOD IF YOU HAVE PAIN THAT IS DUE TO INFLAMMATION inhibit COX 2 AND COX 3( form of cox 1 only found in the brain) reversible non competitive inhibition NSAIDS analgesic anti pyretic anti inflammatory inhibit COX 1 AND COX 2 |
| Cox enzyme inhibition Aspirin ibuprofen paracetol | aspirin- irreversible inhibition of COX, binds permanently to the enzyme = prostaglandins not produced ibuprofen- reversible , competitive paracetamol- reversible non competitive |
| drugs and Analgesic activity | decrease prostaglandin synthesis prevent PG induced sensitisation of nocioreceptors on nerve endings paracetamol cox 3 in brain dampens down the pain pathway |
| painkillers drug safety | aspirin NSAIDS toxic at high doses, accidental death bronchoconstriction ASPIRIN ovedose Reyes syndrome if they recovering from viral illness paracetamol toxic at high doses risk of liver damage having it regularly difficult to treat overdose |
| Opioid analgesics | cant prescribe this Agonists – morphine, diamorphine HEROIN, methadone, codeine ( small amounts can be GSL) Antagonists – naloxone, naltrexone Mixed action compounds – buprenorphine, pentazocine |
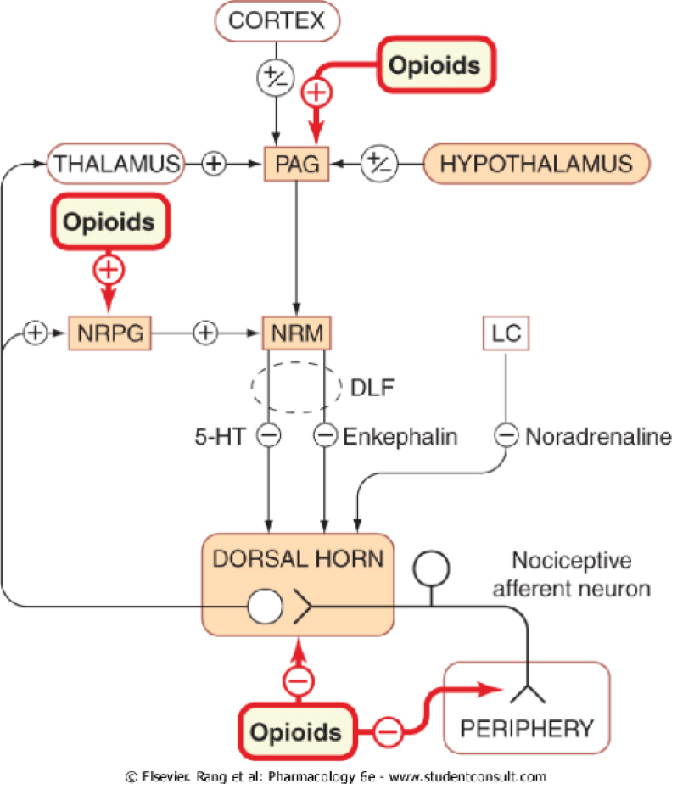
| Opioids and pain pathway | opiods can have an affect at the level of the brain to dampen down the pain signal. thalmus, at the spinal cord to prevent the pain signal to be sent opioids receptor present all across the pain pathway |
| Codeine | one of the least potent opioid analgesics reduced analgesia available as P medicine combined with paracetamol co - cocadamol normally POM |
| dihydrocodeine | slightly more potent than codeine available as P medicine combined with paracetamol Paramol normally POM |
| OPIOID ANTAGONISTS | reverse effects of agonists- emergency situations only used to treat respiratory depression in neonate ( If they are absorbed the featus during child birth then they can be used) in overdose |
| mixed action compounds | agonist/partial agonist at opioid receptor increase analgesic effect DOESNT WORK BASICALLY |
| general ocular response | pathogen--> innate immune response --> pronounced vasodilation BVs becoming more leaky --> emigration of WBCs and other inflammatory factors --> WBCs accumulation / mucus/ DISCHARGE |
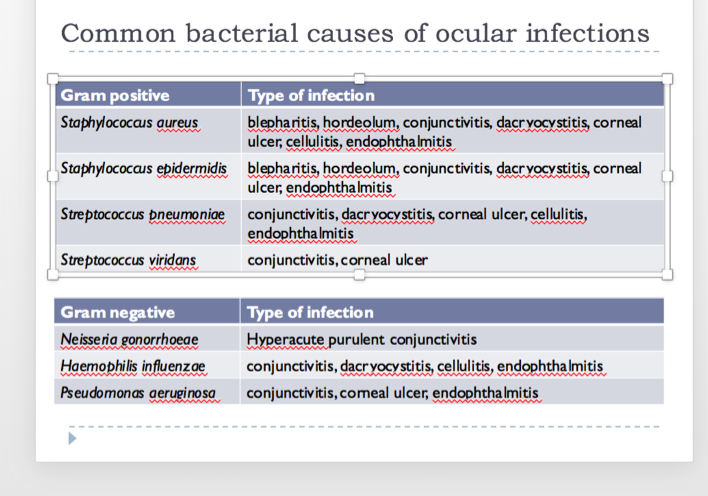
| sites of ocular infecction | Membrane of the inner eyelid – conjunctivits Eyelid – blepharitis Cornea – keratitis Iris – iritis Nasolacrimal sac – dacryocystitis Gland of Zeiss (eyelash) – hordeolum (stye) Intraocular cavity (lining or liquid) – endophthalmitis / vitritis Retina and blood vessels supplying it – chorioretinitis Optic nerve – neuroretinitis Conjunctivitis in newborn (up to 28days old) - ophthalmia neonatorum sometimes from STD |
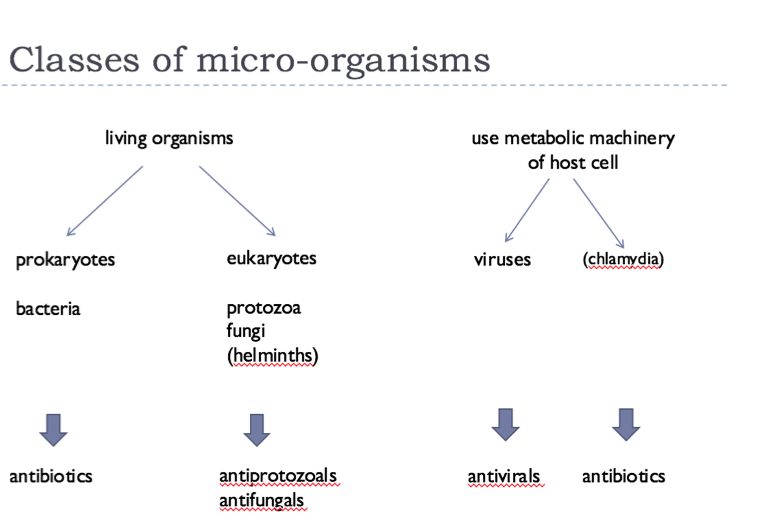
| class of micro- organisms |
Image:
Class (binary/octet-stream)
|
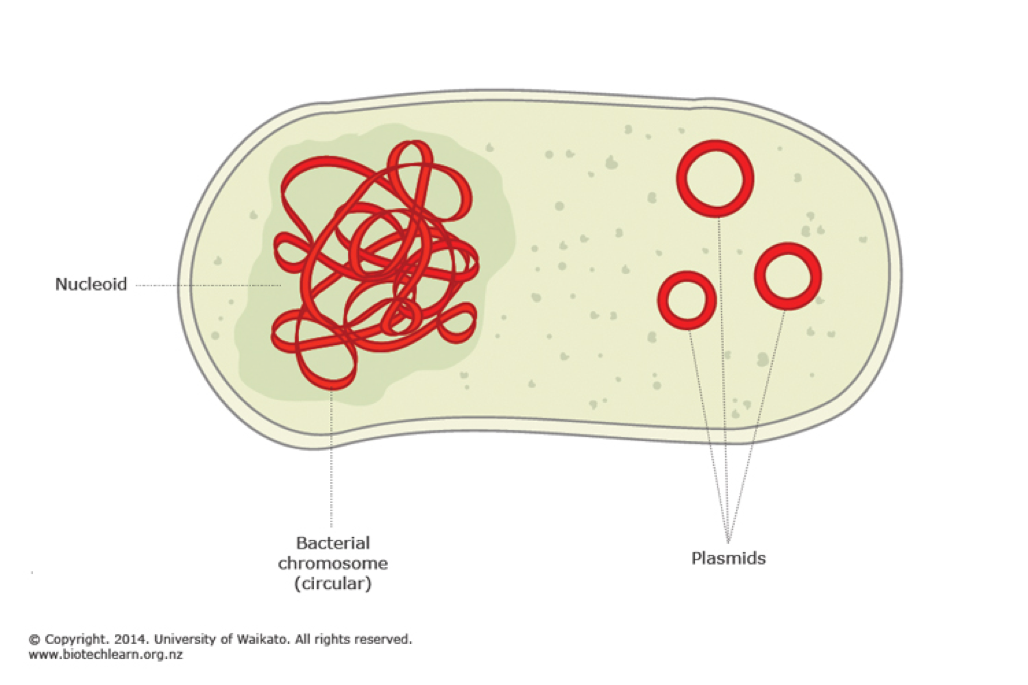
| Bacteria characteristics | living organism single cells no nucleus no membrane bound organelles DNA- single loop additional loop of DNA called plasmid plasmid can cause bacteria resistance! 1) cell elongates and DNA replicates 2) cell wall and plasma begin to divide 3) cross wall forms complete around DNA 4) cell seperates cocci spherical bacilli ( tablet shape) rod spirilla ( spiral) vibrous ( comma sausage) spirochaetes ( corkscew) |
| bacterial resistance | micro organisms can adapt itself so is no longer effective against it alter the target site for the drug so it is no longer binds MRSA- hospitals clostridium difficile- severe nausea/ diareohea |
| Differentiation of bacteria | gram - doesnt stain it gram + does stain it |
| Common bacterial causes of infection | |
| Mechanism of action ( bacteria) | cell wall structure - PENICILLINS,CEPHALOSPORINS , BACITRACIN, VANOMYCIN cell membrane permeability - POLYMIXINS protein synthesis- AMINOGLYCOSIDES, CHLORAMPHENICOL, FUSIDIC ACID, DIAMIDINES dna replication- FLUROQUINOLONE |
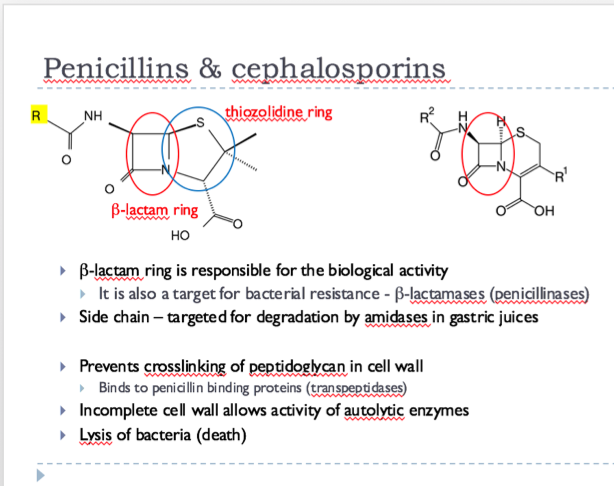
| penicillions and cepholosporins | |
| Mechanism of action - pencillion | the bacteria cell wall consists of strands of peptidogylcan the pencillin binding protein binds the peptide side chains by forming a cross- link the PBP dissociates from the wall once the cross link has been formed pencillin can enter the active site of the PBP and reacts with it to inhibits its enzymatic activity involved in cross linking the Beta- lactam ring og pencillin is irreversibly opened during the reaction with the PBP. pencillin remains convalently linked to the PBP and permenantly blocks the active site |
| Pencillin use | systemic only high incidence of allergic reactions very commonly used broad spectrum - active against gram +, gram - naturally occurring Pencillin G and Pencillin V synthetic pencillins Flucloaxcilin amoxicilin Type 1-type IV sensitivity reactions with penicillins and 1st generation cephalosporins Type 1 / IV most common uticaria, angiodema contact dermititis, Steven-Johnson syndrome Cross reaction between penicillins and 1st generation cephalosporins can occur Most common side effects Nausea, diarrhoea (upsets normal gut bacteria) Cephalosporins Vitamin K deficiency – destroys bacteria that synthesis vit K Bleeding (C/I haemophilia) Nephrotoxicity Cefaclor – metabolite causes Type III reaction (skin / joints) |
| Bacitracin | Mechanism of action Prevents movement of a precurser to petidoglycan from cytoplasm through cell membrane to cell wall Therefore, inhibits synthesis of cell wall Resistance – low Active against gram positive but NOT gram negative (except N. gonhorreae) Topical use only as causes renal necrosis Used to be available as eye ointment with polymixin B or neomycin but discontinued in 2005 |
| Vanomycin | Mechanism of action Prevents synthesis of peptidoglycan by binding to mucopeptide precurser Therefore, inhibits synthesis of cell wall Resistance – low Active against gram positive especially those resistant to most other antibiotics Use usually reserved for these resistant infections Can be ototoxic and cause permanent deafness when used in conjunction or subsequent to other ototoxic antibiotics |
| drugs affecting cell membrane permeability | gramicidin Mixture of gramicidins Mechanism of action Acts as a detergent – disrupts phospholipid component Makes cell leaky, killing it Active against gram positive (except baccilli) and gram negative Causes haemolysis: TOPICAL use only Only available as a combination product with steroid Sofradex® - dexamethasone 0.05%, framecytin 0.5% & gramicidin 0.005% Can be used prohylactically when conjunctiva or cornea are compromised TOPICAL ONLY polymixin B TOPICAL ONLY Mechanism of action Acts as a detergent – disrupts phospholipid component Makes cell leaky, killing it Effective against gram negative, including P. aeruginosa Neuro- and nephrotoxic: TOPICAL use only Only available as a combination product with steroid Maxitrol® - dexamethasone 0.1%, neomycin 0.35% & polymixin B 6000units / ml Can be used prohylactically when conjunctiva or cornea are compromised |
| drugs affecting protein synthesis | aminogylocosides,tetracyclines, macrolides, chloramphenicol |
| Aminogylcosides | Mechanism of action Binds irreversibly to 30S subunit of ribosome Resistance Mutations in the ribosomal binding site Decreased uptake into the cell Enzymatic modification of the antibiotic Activity against gram positive and gram negative bacteria Includes against P. aeruginosa (except for neomycin) Not active against MRSA Can cause ototoxicity and nephrotoxicity Not normally seen with topical administration Hypersensitivity reactions common SOME OCULAR SOME SYSTEMIC binds irreversibly to Mrna so it changes the shape so the tRNA cannot bind to the mrnA Gentamicin Gentacin® - gentamicin 0.3% (multidose + BKC) Tobramycin Tobravisc® - tobramycin 0.3% (multidose + benzododecimum bromide) Neomycin Maxitrol® - dexamethasone 0.1%, neomycin 0.35% & polymixin B 6000units / ml |
| tetracyclines | Mechanism of action Prevents tRNA binding to the 30S subunit of ribosome-mRNA complex Resistance (high) Decreased penetration through cell wall Active efflux out of the cell Protection of the 30S subunit Activity against gram positive and gram negative bacteria Includes against spirochaetes and chalamydiae Not active against P. aeurginosa or Proteus Chelate calcium Affect teeth and bone growth Rare with topical use tRNa cannot bind used for acne, careful during pregnancy |
| chloramphenicol | Mechanism of action Prevents elongation of protein by binding to 50S subunit of ribosome Resistance Plasmid encoded chloramphenicol transferase Chromosomal mutations causing altered outer membrane Activity against gram positive and gram negative bacteria Includes against spirochaetes, rickettsaie and chlamydiae Not active against P. aeurginosa Can cause aplastic anemia leading to agranulocytosis Avoid if family history of blood dyscrasias Very rare with topical use P medicine TOPICAL ONLY binds to 50s portion and inhibits formation of peptide cant bind to tRNA |
| macrolides | Mechanism of action Prevents elongation of protein by binding reversibly to 50S subunit of ribosome Resistance Methylation of 23S ribosomal unit Enzymatic cleavage (esterase) Active efflux Activity against gram positive and some gram negative bacteria Each macrolide has different spectrum of activity Azithromycin (Azyter ® - single use drops) binds to 50s portion prevents movement along mRNA |
| Fusidic ACID | Mechanism of action Prevents translocation of elongation factor G (EF-G) from the ribosome thereby interfering with protein synthesis Resistance Alterations in EF-G gene Activity against gram positive and some gram negative bacteria Fucithalmic ® - 1% viscous drops (BKC + EDTA) P drug dont get the protein change |
| inhibition of nucleic acid synthesis | quionolones fluoroquinolones metronidazole rifampicin |
| quinolones/ fluoroquinolones | Mechanism of action Bind to alpha subunit of DNA gyrases or topoisomerases therefore preventing supercoiling of DNA Resistance Altered alpha subunit of DNA gyrase Decreased uptake by alteration of porins Activity against gram positive and some gram negative bacteria Systemic side effects Local side effects Well tolerated, rare hypersensitivity, comfortable to use Ciprofloxacin – white corneal deposits – can damage the cornea prevents DNA from being translated MMa cannot be formed most side effects systemic Levofloxacin Oftaquix ® - 0.5% single dose and multi dose (+BKC) Moxifloxacin Moxivig ® - 0.5% multidose + BKC Ofloxacin Exocin ® - 0.3% multidose + BKC Ciprofloxacin Ciloxin ® - 0.3% drops (multidose + BKC); ointment |
| interference with uptake of DNA, rna precursers | diamidines |
| propamidine and dibromopropamidine | Mechanism of action Block permease transport system in the cell membrane Inhibits uptake of purine nucleotides Prevents synthesis of DNA, RNA and proteins Resistance Alteration of the transport system? Activity against gram positive and some gram negative bacteria Local side effects Well tolerated, rare hypersensitivity, comfortable to use Available OTC and so to all Optoms (level 1 and 2) Brolene® eye drop and ointment P medicine prevents nucleotides being taken up by the medicine |
| antibiotics with antimetabolitee activity | sulphonamides trimethoprim |
| Sulpohamides | Mechanism of action Compete with PABA preventing synthesis of folic acid Resistance Cell wall / membrane permeability Activity against gram positive and some gram negative bacteria Systemic side effects Hypersensitivity; Stephen-Johnson syndrome Local side effects bacteria synthesise their own folic acid not very common |
| trimethorpim | Mechanism of action Inhibits dihydrofolate reductase preventing synthesis of folic acid Resistance Altered affinity to dihydrofolate reductase Intrinsic resistance Activity against gram positive and some gram negative bacteria Systemic side effects Local side effects not ocular used for uti as it accumulates in urinal tract |
| optometrist and bacteria management | Lid scrubs Propamide / dibromopropamide Chloramphenicol Fusidic acid Bacitracin / polymixinB? Aminoglycosides (gentamicin, neomycin) Fluoroquinolones (ofloxacin, levofloxacin, ciprofloxacin) Infection more than 7- 14 days think about antibotics Bacterial keratitis- immediately use antibiotics Conjuctival –usually resolves itself Affecting the cornea need to treat as vision can be compromised Depends on what level you are Lid scrubs- get rid of the bacteria on the surface Aminoglycosides / fluroquinolones – prescribing person 1st line chloramphenicol 2nd line Fusidic acid 3rd line (GP; SP, IP) Ofloxacin; ciprofloxacin; gentomicin 4th line (Ophthamologist only) Cefuroxime ophthalmic solution (fridge required) general hygiene- dont share towels etc |
| Acanthamoeba keratitis | Multiple Acanthamoeba species are known Free-living, protozoan (amoeba) which is parasitic Usually picked up by: swimming in infected water with contact lenses in; washing contact lenses in infected water or making up solutions in infected water Contact lens wearers more prone due to Lack of oxygen reaching cornea Build up of bacteria on lens Corneal abrasions Symptoms foreign body sensation, photophobia, decreased visual acuity, tearing, pain and redness of the eye Ring infiltrate round cornea characteristic Can be mixed up with herpes simples virus keratitis “Ground glass” epitheliopathy Hard to treat It exists in cyst form ( dormant) got a thick cell wall so hard for drugs to penetrate but they do have mucus plugs at the occasianal part of the cell wall Can exist in active form trophzoite Cyst form is hard to treat Need to get rid of the cysts as they can become active Need to take a swab to have a diagnosis use confocal microscope to see the cysts cant see them with naked eye |
| treatment of acanthameoba keratitis | Mixture of antibacterials used: biguanides & diamines Chlorhexidine 0.02% PHMB (polyhexamethylene biguanide 0.02%) Propamidine isoetrionate Cystocidal Chlorhexidine 0.02% PHMB (polyhexamethylene biguanide 0.02%) They are cationic detergents. The positive biguanide groups bind to cell wall / membrane and cause pores to form causing leakage of cell contents and death. Also compromise the mucopolysaccharide plug that seals the cyst. Very intense treatment Hourly administration for 2-3days, reducing in frequency Treatment for minimum 2 weeks – commonly 6-12months Neomycin may be used but toxicity an issue Topical cycloplegics, topical NSAIDs or oral analgesics may also be used Topical steroids should NOT be used – worsen condition 3 drugs in combo to be cystisidal 2 weeks for epithelium Deep eg stroma than 6 -12 months Neomycin can be used but not that effective really need a high dose Cylplegics nsaids can be used to reduce the inflammation due to the acanthameba Prognosis less likelihood of recovery than any other ocular infection But can still have outcome of normal vision |
| viruses | RNA or DNA surrounded in a protein coat (capsid) Unable to divide on their own invade a host cell to replicate How do they do this? They bind to normal cell constituents to gain access Cytokine, neurotransmitter, hormone receptors Ion channels Integral membrane glycoproteins |
| viral replication | viruse enters the host the virus uncoats itself to allow DNA to come out the virus the DNA enters the nucleus of host cell -causes replication of viral DNA - transcription of viral DNA and viral mRNA viral proteins proteins enter the nucleus and reassemble they go into the cytoplasm and exit to infect somewhere else |
| virus transcription and translation | viral genome exists as a double strand similar to human DNA RNA polymerase copies DNA strand ( +) to viral mRNA DNA polymerase is used to copy a strand of DNA + and - strand to form dsDNA |
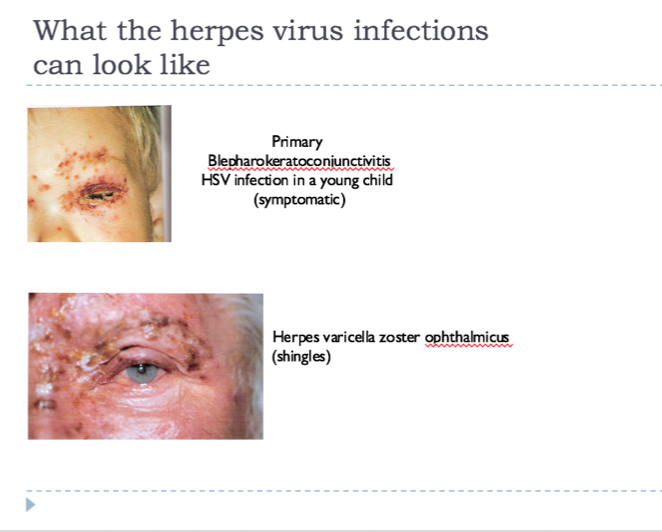
| viral infections | DNA viruses Herpes simplex virus (HSV-1) most common Cytomegalovirus (HHV-5) Varicella-zoster (chicken pox / shingles) Adenoviruses - more common in developing countries RNA viruses Rubeola (measles) Rubella (German measles) Variola (small pox) -redness -itching -watery eye -photophobia -blisters on ocular surface./ skin - often unilateral |
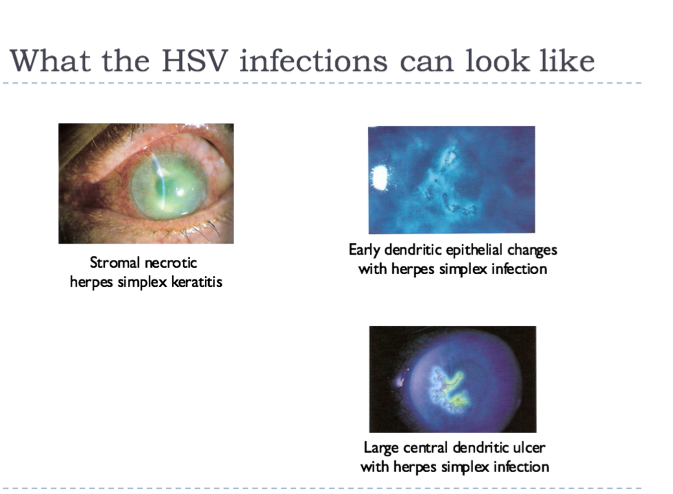
| Herpesvirus infections | primary infection may be asymptomatic or mild BUT virus transports itself down nerve ending to cell body, virus then lies dormant ( doesnt divide) in the sensory ganglia. trigger causes viral replication- recurring infections SITES OF INFECTION lids belpharitis conjuctiva conjuctivitis cornea keratitis uvea uveitis retina retinitis |
| virus and infection | infection has an inflammatory stage --> virus codes proteins very similar to human ones ( immune system attacks virus and normal human proteins) --> virus coat has protein UL6 similar to proteins in cornea , chemokines and cytokines released. inflammatory cascade -->inflammation and lots of damage |
|
Image:
Hsv (binary/octet-stream)
|
Image:
Hsv 2 (binary/octet-stream)
|
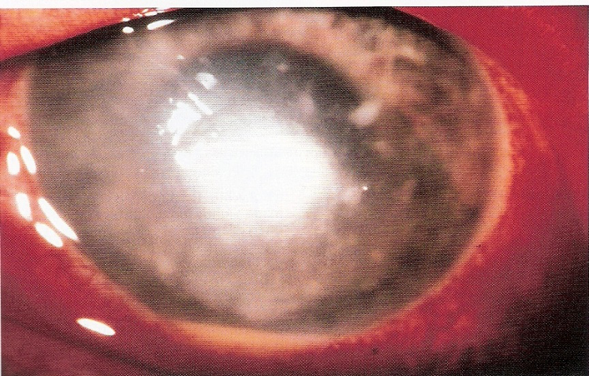
| herpes varicella zoster infections | secondary to original chicken pox infection involves ophthalmic nerve causes hyperesthesia prior to the vesicular rash major risk of corneal scarring and uveitis corneal staining,cataract, glaucoma, macular oedema |
| cytomegalovirus | infection occurs in immuno-compromised people( HIV + or immunosuppressants) CMV retinitis can cause progressive damage to retina leads to blindness in 4-6 months increased risk of retinal detachment RARE like my steak |
| antiviral drugs | topical acyCLOVIR ganciCLOVIR systemic famciCLOVIR penciCLOVIR |
| mechanism of action - antiviral | inhibits the transcription the viral DNA the phosphorylated forms of the drugs compete with normal phosohorylated purines ( mimic the protein bases that make up the DNA of the virus ) initial phosphorylation of the drug is by the viral thymidine kinase - only present in virus not the human cell -structure of drugs mimics nucleotides and therefore prevents protein chains for forming as it inhibits viral DNA polymerase drug combines with ATP and then thymidine kinase which is only in virus cell causes acyclovir phosphate to be formed --> human enzymes are used to form acyclovir TRIPHOSPHATE --> then uses another viral specific enzyme DNA polymerase to incorporate into viral DNA |
| anti viral side effects drug regime | topical - rare systemic- fever rash diarrhoea high conc and freqency eg 1 drop x 5 for 5 days use systemic if topical doesnt work |
| RNA retroviruses | HIV- human immunodeficiency virus enzyme reverse transriptase makes DNA copy of viral DNA, this DNA then becomes intergrated into host genome. reverse transcriptase inhibitors nucleotide RTIs non nucleotide RTIs- denature the catalytic site of RT protease inhibitors inhibit viral proteases which cleave precurser polyproteins disrupt structural and functional proteins of new virons COMBO OF DRUGS REQUIRED TO PREVENT HIV FROM OCCURING |
| fungi | eukaryotic cell many are parasitic- live off the host and destroy RARE LIKE MY STEAK athletes foot and thrush |
| fungal infections | fungal keratitis fusarium aspergillus candida increase in occurance - topical steroid overuse - immuno compromised individuals -overuse of antibiotics gain access through damaged epithelium FB sensation eye pain sudden blurry vision redness excessive tearing photophobia |
| fungal keratitis |
fine or coarse granular infiltrate
other forms such as orbital cellulitis and dachryocystitis
irregular edged infiltrate
white ring in the cornea
treatment
no commercial preparations available
can be made on request from Moorfields
sometimes polyenes are used
Image:
Fk (binary/octet-stream)
|
| polyenes | Amphoteracin B - broad spectrum binds to ergosterol in cell wall not present in human cell makes transmembrane ion channels disrupts ion balance and leads to death of the fungal cell not absorbed after oral adminstration treats GI TRACT given by injection - side effects chills, fever, vomitting Nystatin- skin ,mucous membrane, GI candidiasis unwanted effects minor |
| azoles | inhibit cytochrome P450 3 A enzyme prevents conversion of lanosterol to ergosterol --> decreased ergosterol alters fluidity of membrane, inhibits replication Clotrimazole fluconazole- orally / iv |
| other antifungals | Flucytosine converted to 5-fluorouracil inhibits thymidylate synthetase interferes with DNA synthesis yeast terbinafine inhibits ergosterol synthesis inhibits squalene lepoxidase prevents squalene being converted to lanosterol |
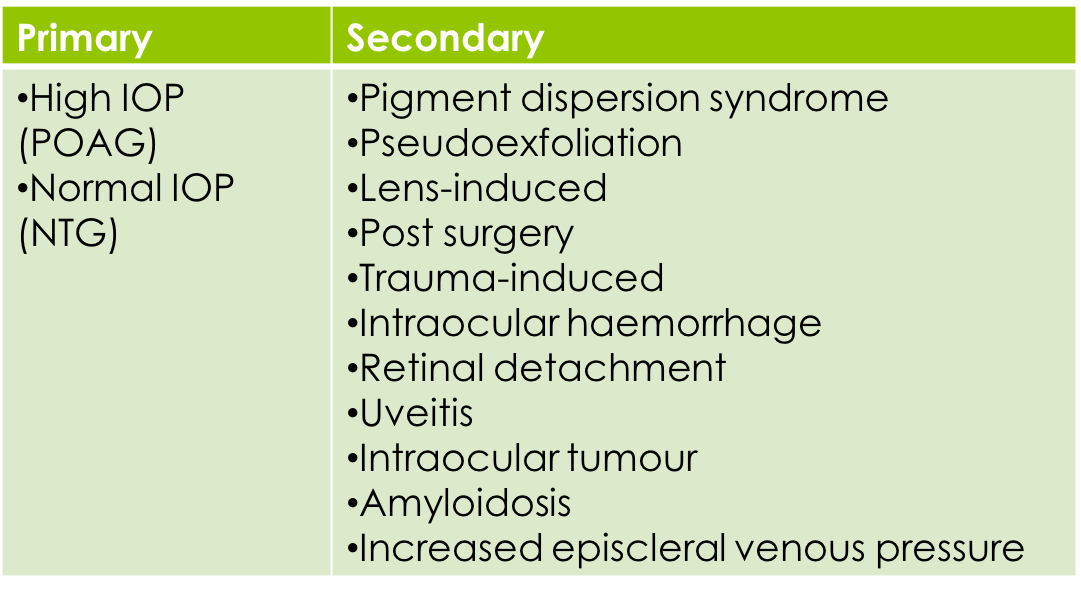
| open angle glaucoma | |
| sites of aqueous humour production and outflow | ciliary muscle and epithelium cells outside of the ciliary body have rich capillary beds. The blood supply comes in from the pressure filtered through the capillary bed goes to the ciliary epithelium , exchange occurs the outer cells secrete to the poster segement aqueous humour. increased secretion of aqueous humour increased IOP --> episcleral vein is what flows out naturally goes from high to low |
| glaucoma | trabecular mesh work is like holes less pressure against the fluid uveoscleral - less common goes through the cell of the ciliary body and sclera through the episcleral vein |
| what do we want for an antiglaucoma treatment | reduce IOP drug to have sufficient duration of action provides preservation of visual field no loss of effect over time compatible with other treatments no topical or systemic side effects |
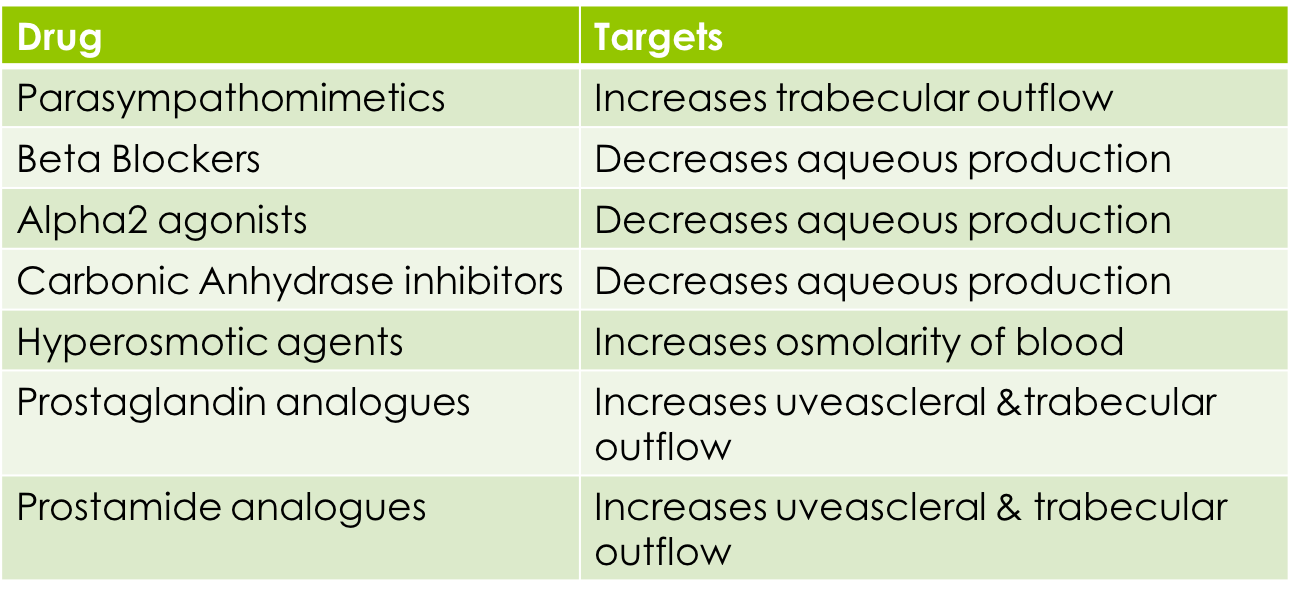
| Drugs and mechanism of action parasympathomimetics? beta blockers? alpha 2 agonists? carbonic anhydrase inhibitors? hyperomsotic agents? prostaglandin analogues? prostamide analogues? POM only |
Image:
Glauc (binary/octet-stream)
|
| management of glaucoma? | Open angle pharmacological - prostaglandin analogues - beta blockers - alpha agonists - carbonic anhydrase inhibitors closed angle emergency- parasympathomimetics systemic carbonic anhydrase inhibitor ( intravenously) surgical |
| NICE GUIDELINES FOR GLAUCOMA | 1st line of treatment prostaglandin/ postroamide analogues - might ADD on beta blockers or if prostaglandins not suitable may start beta blockers - if it doesnt work then carbonic anhydrase inhibitors might be added - alpha agonists - more for acute not for chronic |
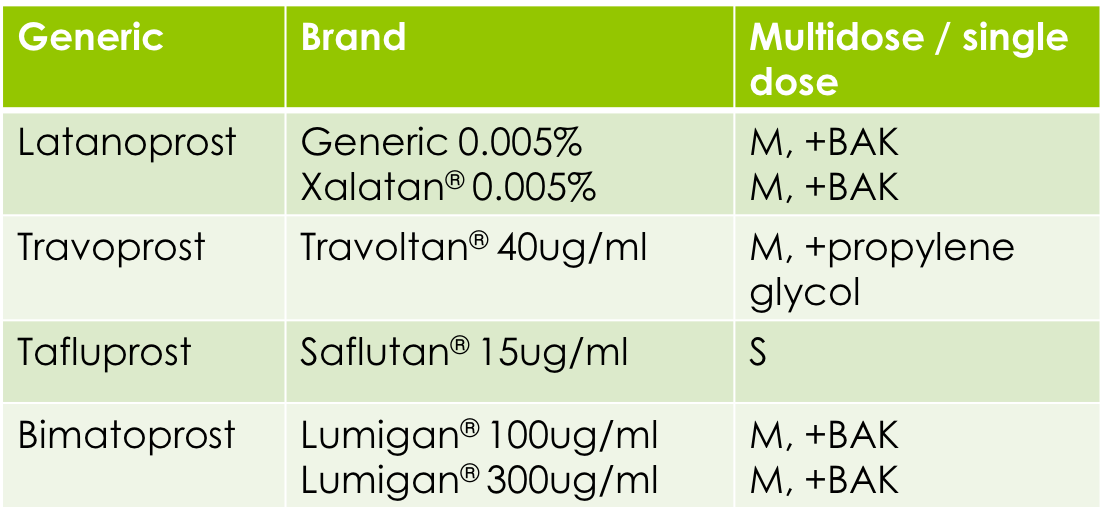
| Prostaglandin analogues | we naturally produce them in most cells. Involved in inflammation and aqueous humour outflow Synthetic drugs that mimic it ( needs to be broken down to acid form to be active) LATANOPROST TRAVOPROST TAFLUPROST act via the FP receptor ( is a G protein coupled receptor). FP receptors are present in eye eg ciliary body, TB increases uveoscleral outflow by breaking down cells eg matrix metalloproteinases, collagen, extracellular matrix. breaking down collagen, breaking down extra cellular matrix so more extra cellular space so no less resistance affect on FP receptor |
| prostglandin analogues examaples | TAFLUPROST LATANOPROST TRAVOPROST prodrugs- ester converted to acid, acid form causes extracellular matrix change long duration of action side effects red eye, increase pigmentation in iris, eye lashes ( monocular makes it a problem), eye lash growth, sensitivity to light CONTRAINDICATIONS IN PREGNANCY |
| prostamide analogue | similar to prostaglandin however not an acid its already active ( not a prodrug) BIMATOPROST analogues of prostaglandin F ethanolamide( prostamide) increases uveoscleral and trabecular outflow |
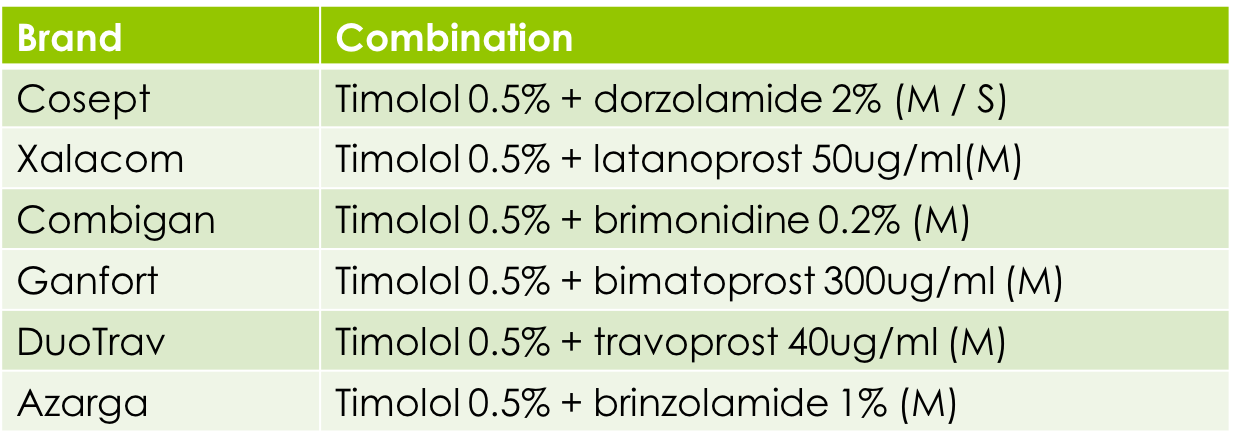
| prostaglandin and prostamide analogues | most common as multi doses commonly combined with other drugs |
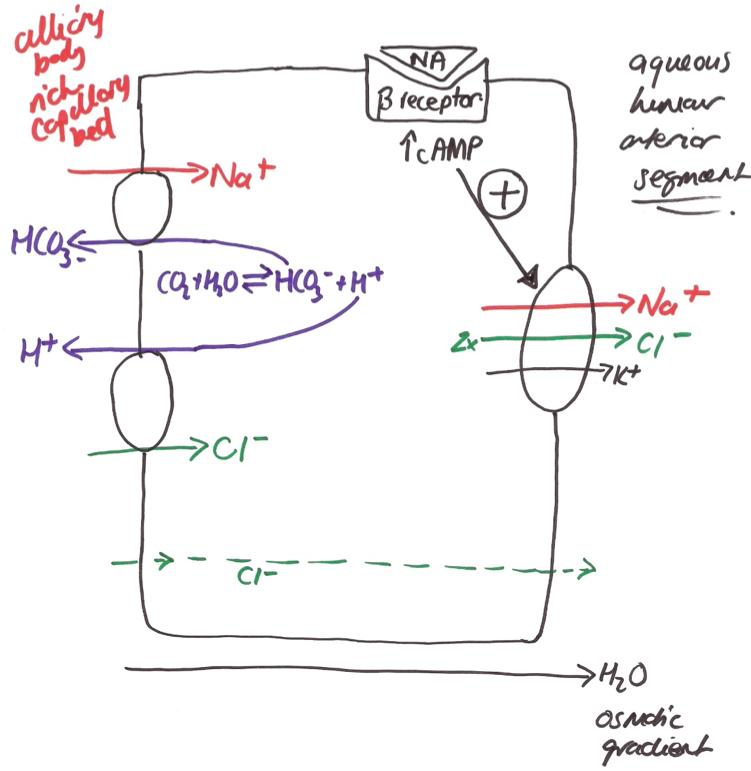
| Beta Blockers -facts | antagonists are B1 and B2 receptors B1 receptors- heart/ kidneys B2 receptors- bronchioles membrane stabilising activity has local anaesthetic activity PROPANOLOL ONLY ( not clinically significant) Beta 2 receptors on blood vessels cause vasodilation. Beta 2 receptors on ciliary epithelial cells stimulation causes aqueous production. SO ANTGONIST CAN CAUSE DECREASE B2 activation stimulates cAMP production cAMP regulates ion transport in the ciliary epithelium --> cAMP activates NA K Cl co transporter --> Cl- efflux in non pigmented epithelial cells stimulation of cl- transport increases aqueous humour production by osmosis. BETA BLOCKERS PREVENT THIS DECREASING AQUEOUS HUMOUR PRODUCTION |
| beta blocker mechanism | Transporter 1) is sodium and bicarbonate 2) chloride and H + Na comes in , Cl gets exchanged back out the cell with sodium, chloride and potassium co transporter. 1 na = 2 cl- Agonist ( noradrenaline) binding activation of g protein coupling increase in cAMP, more cAMP promotes more ions out of this chamber = so more fluid goes to posterior then anterior segment CONC GRAD block noradrenaline binding less cAMP = less fluid |
| beta blockers - advantages - disadvantages | advantages well tolerated rapid onset of action efffective in 75% of patients compatible with other drugs disadvantages can observe effects on treated and UNTREATED eye systemic side effects-cardiovascular effects chronic use becomes less effective |
| beta blockers side effects | generally systemic cardiovascular - bradycardia, hypotension CONTRAINDICATED WITH HEART BLOCK/ HEART FAILURE bronchial constricts bronchioles CONTRAINDICATED ASTHMA diabetic- masks hypoglycemia as they lower blood sugar |
| normal tension glaucoma | beta blockers should only be used in morning if used at night causes a dip in blood pressure |
| beta blockers for glaucoma |
TBC Lol
Timolol- timbits ( most common)
betoxalol- detox
carteolol - cartier
levobunolol - harry potter
MOST COME AS MULTIDOSE
timolol = levobunolol > carteolol
timolol gel forming solution prolongs time in conjuctival sac
carteolol is least lipophlic therefore less CNS side effects
leveobunolol formulated in alcohol to increase eye contact time
fixed dose combinations
patient compliance
reduces exposure to preservatives
avoid wash out effect of use of 2nd drop
decreases cost of treatment
Image:
Gluuc (binary/octet-stream)
|
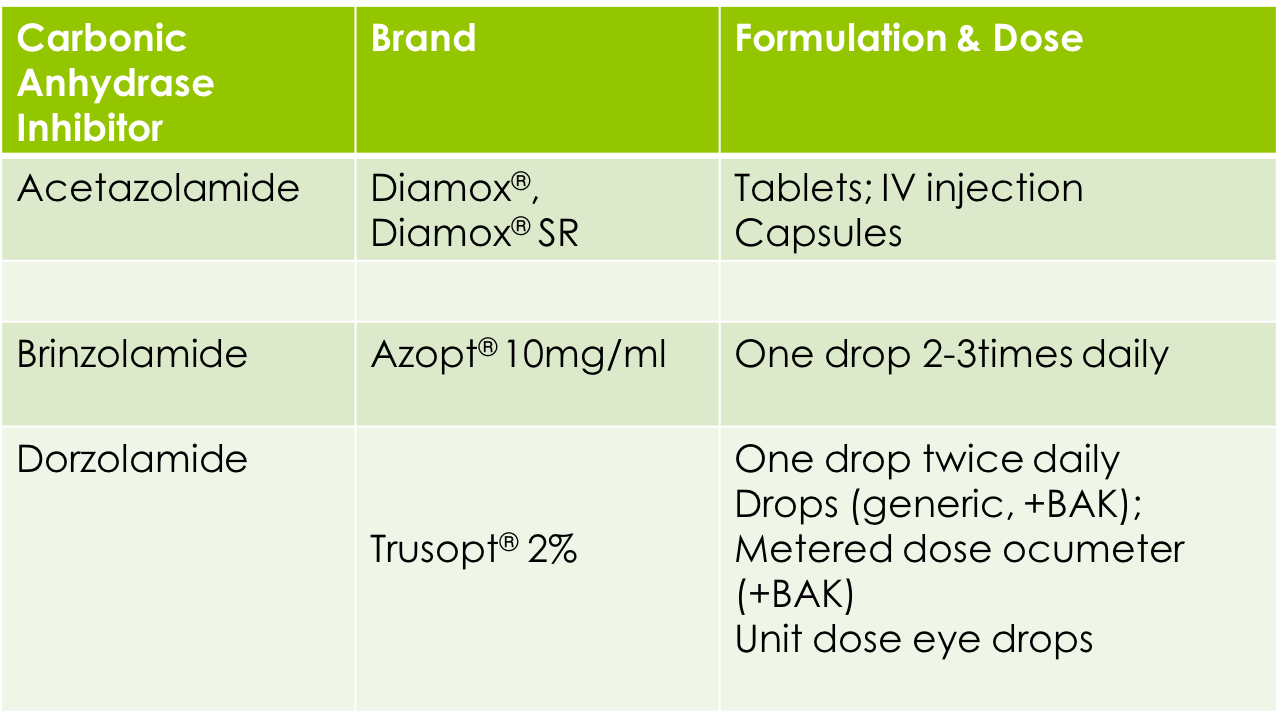
| carbonic anhydrase inhibitors mechanism | systemic ( limited to emergencies) and topical use inhibit carbonic anhydrase ( enzyme) in ciliary epithelium so bicarbonate isnt formed which is needed for aqueous secretion --> reduced aqueous formation = lower IOP dont get build up ions so less transport |
| systemic carbonic anhydrase inhibitor |
Acetazolamide- intravenously
not absorbed topically
used in emergency
carbonic anhydrase enzymes- has effect on many places eg liver
side effects
sulfonamide derivative - increased risk of allergy and blood disorders
enzyme present throughout body:
gastrointestinals problems
diuresis
drowniess/ depression
pins and needles
topical CAIs
ajunct treatment with beta blockers, prostaglandin inhibitors
indicated as sole therapy when patient cannot use beta blockers
transient burning, stinging
blurred vision, conjuctival hyeraemia
TASTE DISTURBANCES, DRY MOUTH
Image:
Cai (binary/octet-stream)
|
| other CAIs | modify acetazolamide to give better lipid solubility to allow corneal absorption decrease likelihood of side effects make more selective - CA-11 enzyme --> dorzolamide --> brinzolamide |
| Sympathomimetics | adrenaline reduces IOP, Dipivefrin (Propine®)was a prodrug for adrenaline (discontinued) More selective drugs marketed ALPHA agonists |
| ALPHA 2 ADRENOCEPTOR | a receptor selective found on ciliary, conjuctival and corneal epithelium advantages no mydriasis no vasoconstriction little effect on the cardiovascular system- no A2 decreases secretion of aqueous - decreases cAMP, ion transport --> aqueous secretion |
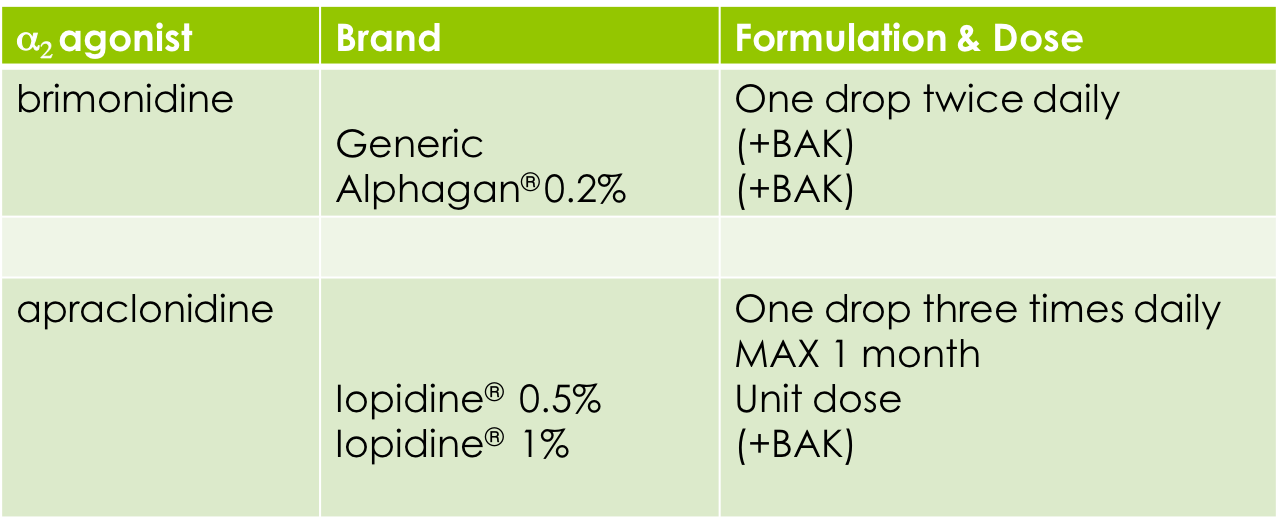
| alpha 2 adrenoreceptor agonists examples | brimonidine selective for a2 receptors rapid onset with peak effect in 2 hrs not used chronically apraclonidine less selective for a2 receptor short term use due to tachyphlaxis( a2 stop responding to the drug) AFTER A MONTH WONT WORK used post surgery to prevent rise in IOP side effects local allergy, stinging, blurred vision, photophobia systemic hypotension, drowsniess, fatigue, dry mouth, taste disturbances |
| parasympathomimetics | pilocarpine contracts ciliary muscle --> pulls scleral spur --> opens tb meshwork --> increase tb outflow --> decreases IOP treatment of closed angle, EMERGENCY USE effects last for 6hrs- need it like x4 a day side effects associated with mechanism of action miosis, loss of light response, ciliary spasm, fluctuating vision NOT THAT EFFECTIVE pilocarpine HCI, pilocarpine nitrate |
| future glaucoma medication | Latonoprostene ROCK- rho kinase inhibitors antibodies against human growth factor |
| how to treat dry eye with no drugs? | if mild avoid AC, smoky places rest eyes gland massage severe punctal plugs - prevents drainage of tear film moisture chamber spectacles contact lens bandage that allows moisture to be retained doesnt look nice though! dietry approaches fish oils omega 3 flax seed oil vitimin E antioxidants |
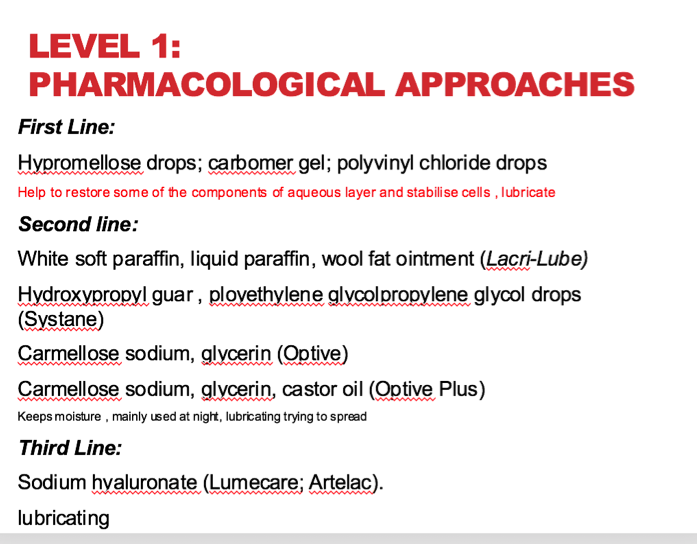
| level 1 pharamcological approaches | |
| tear substitutes artificial tears | artificial tears part of treatment across all severity levels non irritant, good lubricating effect, prolonged presence on the surface of the eye, no disturbance optically ELECTROLYTES - need to replenish keep intergral corneal epithelial barrier, help with mucin secretion HC03 ( helps with mucin secretion) OSMOLARITY normal tears are 300 Osm/L , 305 mOSM pH - need to be near 7 to mimic normal tear film VISCOSITY/ LUBRICANTS, PRESERVATIVES |
| tear substitutes POLYMERS | provides some protection to ocular surface, lubrication of the eye GREATER VISCOUSITY --> increased contact time frequent application as they dont keep the tear film for as long so applied many times Methylcellulose polymers methylcellulose (MC), methyl hydroxy ethyl cellulose (MHEC), hydroxypropyl methyl cellulose (HPMC; Hypromellose), hydroxyethyl cellulose (HEC), hydroxypropyl cellulose (HPC), carboxyl methyl cellulose (CMC) polymers how do they work? help the lipid layer and aqueous layer together. Supplement some of the functions of the mucin. Natural replenish tear film |
| tear film polymers HPMC | hydropropylmethycellulose HPMC neutral polymer - no charge doesnt cause damage less viscous- spreads and lubricates really well very cheap hypromellose isopto plain alkaline tears naturale single use= expensive |
| tear substitutes polymers HMC CMC | hydromethylcellulose less viscous , minims artificial tears SINGLE USE CMC - carboxymethylcellulose high molecular weight and negative charged polymer lubricant and mucoadhesive Optive - multidose - charge helps with attraction with different polar greats helps keep layer together, reacts with the mucins more HIGHER COST celluvisc single use |
| tear substitutes lubricants | PVA polyvinyl alcohol PVA good wetting agent- non ionic surfactant good retention- low viscosity but absorptive Hyotears, Liquifilm tears, Sno tears ( MULTI dose) liquifilm tears ( single use) Povidone mixture of synthetic polymer chains viscoliser and non ionic surfactant Oculotect ( single use) |
| tear substitute gels | Carbomers high molecular weight polymers ( better than hydromels) of acylic acid cross linked with other molecules stablises tear film BETTER THAN HYDROMELS think on blinking, then reforming of gel retained for longer, less frequent application EXPENSIVE gel tears, liquivisc, viscotears |
| tear substitutes ointments | Paraffins white soft paraffin, liquid paraffin melts at eye temperature- becomes thinner so they can spread greasy- longer contact time used at night as it interfers with vision lacrilube, lubri- tears, simple eye ointment Carmellose sythenthic polymer |
| problems associated with tear substitures | preservatives BKC damage with frequent exposure( high risk of allergy) Benzalkonium chloride some of them have invisible preservatives eg NAFL they break down the exposure with UV light , you dont get the irritant effect. broken down to ions and free radicals could cause damage transient blurring- could affect daily work frequent application- affect patient compliance P medicine medical device 2 - 6 months not covered by medicine act IF APPLIED FOR MORE THAN 4 X DAY use preservative free may be preferred option phosphate containing drops can produce corneal calcification can be expensive |
| Biofilm | SYSTANE Hp guar gum galactomannan borate( to buffer) keeps it aqueous phase propylene glycol PEG400 lubricants available on NHS thicken mucus layer unique biphasic mechanism of action - first it binds to damaged hydrophobic areas of epithelial cells to add volume to the tear film - then it restructures the tear film by forming a protective gel matrix that provides long lasting proetection bulks up tear film |
| viscoelastic preperations | sodium hyaluronate High molecular mass polymer composed of repeating dimeric units of glucuronic acid and N-acetyl glucosamine which forms the core of complex proteoglycan aggregates found in extracellular matrix. Sodium hyaluronate has water retaining properties and provides a low resistance to blinking. It is highly effective at entrapping water and preventing evaporation; this prolongs any beneficial effects hydrates the eye, traps water molecules Oxyal, Vismed (multidose), Artelac Rebalance; Lumecare Clinitas, Ocusan, Vismed (single dose) LEVEL 3- |
| Lipid spray | CLARYMIST SPRAY Liposomal delivery system for phospholipids Phosphatidylcholine Improves lipid layer Improves tear film stability Spray onto closed lids Avoids blurring of vision, reflex tearing Classed as a medical device Not covered by Medicines Act Not covered by NHS doesnt need to be used as frequently expensive |
| mucolytics | ACETYLCYSTEINE Used in DED with impaired or abnormal mucus production Breaks down the mucus Reduce viscosity Reduce stickiness ILUBE – combined with hypromellose, BKC, EDTA Legal status we can get build up mucin strands, carbs, lipoproteins being discreted horrible smell ewwwww |
| dry eye alternative approach anti inflammatory | Moderate to severe DED Corticosteroids NSAIDs Both associated with causing epithelial defects and so cannot be used long term tackling underlying cause causes damage to corneal epithelial cells |
| dry eye alternative approach ciclosporin A | Topical ciclosporin A Restasis (0.05% ciclosporin); Restasis X (0.1%) Ikervis (0.1% cyclosporin) Inhibits calcineurin-phosphatase pathway Forms a complex with cyclophilin Inhibits transcription of T-cell activating cytokines (IL-2) Increases tear production – couldbe bad Local release of parasympathetic transmitters reduces inflammation PROS Decreased symptoms, use of artificial tears, inflammatory markers & cells on ocular surface CONS Burning sensation; up to 6months for improvement |
| dry eye alternative approach Lifitgrast | Binds to LFA-1 (lymphocyte function antigen-1) Expressed on T cells 275KDa heterodimeric protein of the integrin family Prevents ICAM-1 (intracellular adhesion molecule) binding to LFA-1 Highly expressed on epithelial, endothelial & immune function cells Prevents: T cell activation, adhesion, migration, cytokine release PROS Decreased symptoms, use of artificial tears, inflammatory markers & cells on ocular surface Onset of action <2 weeks Dose response relationship |
| IL-1 inhibitors dry eye alternative approach | Reduce production of cytokines Reduce immune response Reduce pain associated with immune response |
| dry eye alternative approach tetracylcline | Tetracycline, azithromycin Decrease synthesis and activity of matrix metalloproteases Decreases production of IL-1 and TNFa Decreases collagenase activity Decreased B cell activation Increases tear stability and tear production Low dose used for 6-12 weeks Greater dose / duration leads to GI side effects Usually used for meibomian gland dysfunction or rosacea related DED |
| secretagogues | Secretagogues MIM-D3 mimics NGF Ecabet increases mucin secretion and basal tear secretion Rebagen (rebamipride) increases mucin secretion and goblet cell number (Japan only) Serum – part of the blood , lots of proteins human blood product issues with infections etc not conveient increases secretion of tear film ONLY IN JAPAN |
| Commonly prescribed drug | Statins warfarin aspirin thyroxine anti hypertensives anti diabetic anti depressants |
| statin what are they used for? | e.g. Atorvastin (Lipitor ®) Fluvastatin (Lescol ®) Pravastatin (Lipostat ®) Rosuvastatin (Crestor ®) Simvastatin (Zocor ®) reduces LDL cholesterol in the blood by interfering with cholesterol synthesis atheromatous plaque formation CAN LEAD TO CRVO thrombus formation after plaque bursts main side effect muscle pain/ wastage |
| warfarin | oral anticoagulant decreases thrombus formation ( blood cotting, CVA prevention) reduces inactive vit K which activates clotting factors produced in the liver potential risk of bleeding Interaction with -aspirin, -ciprofloxacin, -cephalasporins |
| Aspirin | not just a pain killer also anti platelet drug ( stops platelets sticking ) inhibits prostaglandin production NSAIDS inhibits the enzyme prevents the arachidonic acid being broken into prostaglandins. NSAIDS inhibit COX1 but also COX2 thromboxane a2 - promotes platelet adhesion and aggregation prostacyclin - inhibits platelet adhesion and aggregation platelets ( txa2) needs to be resynthesised, endothelial cells ( PGI2) can synthesis more enzyme continously |
| thyroxine | The thyroid gland produces hormones that are essential in maintaining metabolic process in the body Regulate the rate at which the body burns energy Insulin and glucagon Hypothyroidism affects 2-5% of the population Weight gain Feeling cold Lethargy Mennorrhagia Decreased mental alertness Dry skin, coarse hair Bradycardia Levothyroxine (thyroxine) replacement |
| anti hypertensives | Decrease blood pressure Beta blockers Diuretics ACE Inhibitors Calcium antagonists |
| beta blockers | Act on CNS to decrease effects of sympathetic outflow Decrease cardiac output β1 receptor Decreases renin release Decreases angiotensin I production Propranolol (Inderal®) Acebutalol(Sectral®) *Atenolol (Tenormin®) *Bisoprolol (Cardicor®, Emcor®) Carvediol Celoprolol (Celectol®) Esmolol (Brevibloc®) Labetalol (Trandate®) |
| diuretics | Decrease extracellular fluid volume Increase in salt and water excretion Decrease plasma volume Reduces cardiac output Therefore decrease blood pressure Also used to treat oedema in heart failure Thiazides Act on kidney Blocks chloride pump on apical membrane Increases excretion of SODIUM and CHLORIDE and potassium Also have a direct vasodilator effect Thiazides: *bendroflumethazide cyclopenthiazide (Navidrex®) Related: metolazone (Metenix 5®) chlortalidone (Hygroton®); indapamide (Natrilix®); xipamide (Diurexan®) loop diuretics Acts on Loop of Henle Blocks sodium/potassium/chloride pump Increases excretion of SODIUM CHLORIDE and POTASSIUM – exchange with sodium in collecting duct Furosemide (Lasix®); Bumetanide (Burinex®); Torasemide (Torem®) |
| calcium channel blockers | Block Ca2+ entry into calcium channels Prevents Ca2+ getting into cells upon depolarisation Reduces ability to contract Cardiac muscle Vascular smooth muscle Vasodilator effect reduces arterial pressure Can cause flushing and ankle oedema *Amlodipine (Istin ®) Nifedipine |
| ACE inhibitors and angiotensin antagonists | ACE converts angiotensin I to angiotensin II (ATII) ATII - VASOCONSTRICTOR Acts at angiotensin I receptors ACE inhibitors Stop formation of angiotensin II; allows vasodilation Decreases total peripheral resistance Decreases blood pressure Angiotensin antagonists Block angiotensin I receptors Captopril (Capoten®) Enalapril (Innovace®) Lisinopril (Zestril®) Ramipril (Tritace®) Side effect: Dry cough Hypotension Kidney impairment Gastrointestinal effects Candesartan (Amias®) Mild side effects (if any) Hypotension (especially if taken with diuretics). |
| anti asthma drugs | Relievers (relieve symptoms) Beta 2 receptor agonists Open up airways Salbutamol (Ventolin ®) Preventers (treat inflammation, prevent symptoms) Corticosteroids Beclometasone Leukotriene receptor antagonists Reduce inflammation and bronchoconstriction Montelukast |
| anti diabetic drugs | Type I diabetes Insulin Type II diabetes Metformin (biguanide, enhances effect of insulin) Increases peripheral glucose utilisation Decreases gluconeogenesis Gliclazide (sulphonylurea, increases insulin release) May cause hypoglycaemia at excessive doses |
| Adverse Reactions muscarinic antagonist | Muscarinic antagonist therapeutic indications ASTHMA GI PROBLEMS , PARKINSONS, TRAVEL SICKNESS - reduced accommodation and blurred vision - mydriasis/ photophobia - CAG in predisposed patients - reduced tear formation due to blockade of muscarinic - DED |
| Adverse reaction Anti-dysrhythmics: Amiodorone | Class III anti-arryhythmic K+ channel block Also NA+ and Beta blocking activity Used for hard to treat arrhythmias Increases action potential duration Increases effective refractory period keeping it simple CARDIAC ARRHYTHMIA --> vortex keratopathy, glare , haloes, |
| Adverse reactions anti dysrhythmics DIGOXIN | - arrhythmias activates K+ACh (vagal tone) blocks AV conduction cardiac heart failure Inhibits Na+/K+/ATPase Increases Na+ in cells, leads to increases Ca2+ , increases force of contraction of heart changes in colour vision, decreased IOP, glare effect, blurred vision |
| Adverse reactions beta blockers | Therapeutic uses Hypertension, angina, arrhythmias Myocardial infarction Anxiety Dry eye Decreased tear lysosome and IgA levels Decreased tear secretion decreased IOP |
| adverse reaction anti-epileptic drugs | eg carbamazepine Diplopia, blurred vision Seen at normal plasma levels (common side effect) lamotrigine Diplopia, blurred vision Nystagmus, conjunctivitis Phenytoin Na+ channel blocker Diplopia, blurred vision, nystagmus, Associated with elevated plasma levels Benzodiazepines Clonazepam, diazepam Positive modulator of GABA Reduced accommodation, mydriasis, diplopia Vigabatrin Inhibits GABA transaminase Nystagmus, double vision, blurred vision Peripheral retinal atrophy Optic neuritis, optic atrophy Visual field defects Defects persist after drug is withdrawn Field testing advised before & during treatment Refer if visual symptoms suspected |
| adverse reaction hormones | Oestrogens & progestogens Contraception Hormone replacement therapy Dry eye Steepening of corneal curvature Decreased aqueous composition in precorneal tear film Corneal oedema, macular oedema due to hypoxia Changes in retinal vasculature Retinal thrombosis Transischaemic attacks Increased risk of stroke Tamoxifen Oestrogen antagonist Used in treatment of breast cancer Corneal changes – structural activity Cataracts Retinopathy Bilateral macula oedema Yellow-white refractile opacities Pigmentary changes, haemorrhages? |
| adverse reactions adrenal steroids | Corticosteroids Inflammatory states (oral) bad asthma Asthma (inhalation and oral) chronicallu Corneal oedema Contact lens problems Raised IOP Posterior subcapsular cataracts |
| adverse reactions NSAIDS | Therapeutic uses Pain Inflammation Corneal deposits (indomethacin) Colour vision changes Blurred vision Refractive changes Dry eye |
| adverse reaction anti malarials | Hydroxychloroquine, chloroquine Anti-malarial (treatment and prophylaxis) Accumulates in lysosomes of plasmodium Forms a toxic complex that kills the parasite Rheumatoid Arthritis Alters activity of lysosomes and endosomes Alters protein degradation and macromolecule assembly Corneal deposits transient and reversible Reversible binding of drugs to intracellular proteins in epithelial cells Toxic macular changes Fine pigmentary mottling with or without foveal reflex loss “Bull’s eye” Progresses – degenerative changes occur in retinal pigmented epithelial cells Optic nerve pallor Ptosis Paracentral scotomas Central red-white visual field defects Colour vision and contrast sensitivity |
| adverse reaction drugs used for erectile dysfunction | Sildenafil & tadafinil Phosphodiesterase type 5 inhibitor (PDE-5) Prevents break down of cGMP in the smooth muscle cells lining the blood vessels supplying the corpus cavernosum Ocular side effect Blue hue Prevents hyperpolarisation of photoreceptors Lasts for about 4hours Pilots – need to see blue runway lights –shouldn’t take within 6 hours before flying! subconjuctival haemorrhages |
| types of adverse reactions | Type A (Augmented) Predictable, acute, related to mechanism of action Stop taking drug the effect goes away, higher dose higher risk Type B (Bizarre) Idiosyncratic, unpredictable acute / sub acute, not related to known mechanism, can happen at any time Extended classification Type C (continuing) Type D (delayed) Type E (end of use) Type F (failure) Type G (genetics / genomics) Type H (hypersensitivity |
| type A adverse reactions | 80% of adverse drug reactions are Type A Predictable, dose-related, mechanistic From primary pharmacology Augmentation of known actions From secondary pharmacology Often involves different organ system but predictable from known pharmacology Low therapeutic ratio of the drug – not much difference between effective level and toxic level so increasing dose can be toxic mild to severe |
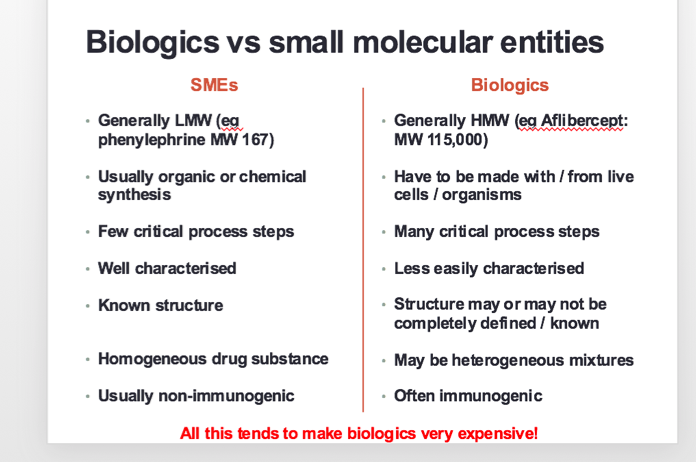
| biologics definition | Section 351 of the Public Health Service (PHS) Act (FDA) defines a biological product as a “virus, therapeutic serum, toxin, antitoxin, vaccine, blood, blood component or derivative, allergenic product, or analogous product, … applicable to the prevention, treatment, or cure of a disease or condition of human beings.” lot of purification is needed |
| SMEs v biologics | |
| why do we use biologics? | exploiting novel targets treatment of disease / disorders that are otherwise untreatable avoid certain side effects |
| antibodies as biologics | Monoclonal antibodies (mAbs): a single type of antibody, highly specific to its target; typically doesn’t bind anything else mAbs for biologics are developed in animals (usually mouse): inject immunogenic material (often needs repeated injections) mouse mounts immune response: B cells produce antibody Remove spleen, extract B cells. immortalise them by fusing with tumour cells (‘hybridomas’) culture individual hybridoma cells: each will be making a slightly different antibody; screen for the most useful Hybridomas can be grown in large scale culture to produce large quantities of mAb (but it must be highly purified before it’s safe to use as a drug) |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.