4289234
| Question | Answer |
| Anti - TB Agents First Line | * INH or isoniazid * Rifampin -Rifabutin Rifapentine * Pyrazinamide * Ethambutol |
| Anti _TB Agents Second Line | * Quinolones (Moxifloxacin, levofloxacin, ciprofloxacin (less active)) * Aminoglycosides (amikacin, capreomycin, streptomycin) * Cycloserine * Ethionamide * P-aminoalicylic acid (PAS) * Linezolid Bedaquiline |
| Isoniazid (INH) | * isoniazid or isonicotinic hydrazide * Prodrug: requires activation by a catalase-peroxidase, KatG * Bacteriocidal against rapidly growing tuberculosis bacilli |
| INH Mechanism of Action | * Blocks the synthesis of cell wall my color acids, the major component of MTB's envelope * 2 enzymes affected by INH -Fatty acid enoyl-acyl carrier protein reductase (InhA) -Complex of a carrier protein (AcmpM) and B-ketoacyl-ACP synthase |
| INH Half Life Dose Metabolism Bioavailability | Half Life: .7-4 hours Dose: 300mg PO daily. Rarely given IM/IV Metabolism: Hepatic Bioavailability: Excellent (90%) |
| INH Toxicity | * Hepatitis: 15% of INH recipients will have minor elevations in AST, True hepatitis .1-.15% * Hepatotoxicity can occur at anytime, most likely 4-8 weeks after start of therapy * Risk of Hepatotoxicity is correlated with age. Uncommon in patients <20. At 50-64 risk is 2%. * Other risk factors: Alcoholic liver disease, pregnancy/post partum state, combination with acetaminophen. * Peripheral neuropathy. Uncommon .2&. Increased risk with DM, HIV, renal failure and alcoholism, pregnant and breast feeding women. Prevention by admin of 25mg vitamin B6 daily. |
| Rifampin Mechanism of Action | * Bacteriocidal against rapidly dividing bacilli * Also active against slowly replicating Intracellular populations of bacilli *Works my inhibiting DNA-dependent RNA polymerase; human RNA polymerase is insensitive. |
| Rifampin Half life Dose Metabolism Bioavailability | Half Life: 1.5 - 5 hours Dose: 600mg PO daily, can be given IV Metabolism: Hepatic. Auto induces its metabolism via the cyp3A4 isoenzyme. Excreted into the bile and undergoes enterohepatic circulation. Bioavailability: Excellent (95%) |
| Rifampin Toxicity | Hepatic. Transient asymptomatic Hyperbilirubinemia .6%. Hepatitis is rare when drug is given alone, but 2.7% when given in combination with INH. Rash Orange-red discoloration of body fluids (tears, saliva, etc.) Flu-like symptoms with thrombocytopenia. (Associated with high dose, intermittent therapy) Significant drug-drug interactions (Due to induction of cyp34A) |
| Pyrazinamide (PZA) Mechanism of Action | Greates activity against populations of dormant or semi-dormant organisms within macrophages or acidic casseus foci. Mechanism of action is unknown; believed to target enzyme involved in fatty acid biosynthesis. |
| PZA Half Life Dose Excretion Bioavailability | Half Life: 12 hours Dose: Weight dependent, oral Excretion: Hepatic and renal Bioavailability: Excellent (100%) |
| PZA Toxicity | Hepatotoxicity 1% Nausea and anorexia common Nongouty polyarthralgia; up t 40% Asymptomatic hyperuricemia Acute gouty arthritis (rare except in patients with Hx of gout) Rash (usually transient) |
| Ethambutol | Bacteriostatic Used to prevent development of resistance in combination regimen. Added to initial treatment regimen if prevalence of INH resistance is >4%. CT INH resistance is 9.1% (2011) |
| Ethambutol Mechanism of Action | Inhibits arabinosyl transferase enzymes which are involved in arbinogalactan nd lipoarbinomannan biosynthesis in the cell wall. |
| Ethambutol Half Life Dose Metabolism Bioavailability | Half Life: 2.5 - 4 hours Dose: Weight based, oral Metabolism: Renal (adjust when GFR <50ml/min) Bioavailability: good (80%) |
| Ethambutol Toxicity | Retrobulbar neuritis -Blurred vision, impaired red-green color vision -Most commonly associated with high dose ethambutol (25mg/kg) -Can lead to blindness via optic neuritis in section of not adjusting dosage in renal insufficiency |
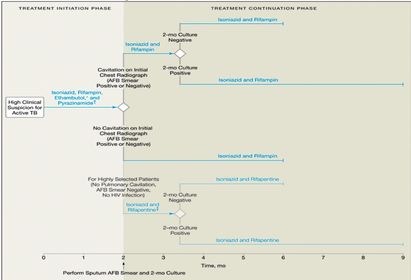
| Anti - TB Chemotherapy Primary Goals | Kill tubercule bacilli rapidly. Prevent the emergence of drug resistance. Eliminate persistant bacilli from the host's tissues to prevent relapse. |
| Anti - TB Chemotherapy Rationale for combination therapy | 3 sub populations of TB in the host -Rapidly growing extracellular bacilli that reside mainly in cavities (largest population) -Due to large size, most likely to harbor sub populations with random mutations which may confer drug resistance -1/1,000,000 for INH and streptomycin -1/100,000,000 for rifampin -For both INH and rifampin resistant bacilli is 1/10^6 X 1/10^8 = 1/10^14 INH and Rifampin work well to prevent emergence of drug resistance. Able to clear live bacilli from sputum in about 80% of patients. The two remaining residual populations grow more slowly a nd are protected by areas of necrosis in an acidic environment, periods of growth spurts interspersed with periods of dormancy. Role for PZA in first two months of therapy. Allowed shortening of duration of therapy from 1 yr to 6 months. |
| Duration of TB Therapy Pulmonary TB | |
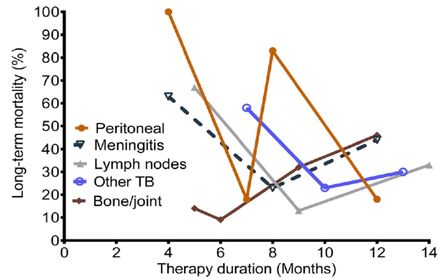
| Duration of TB Therapy Extra pulmonary TB | The relationship between treatment duration and mortality is a "V" shaped curve. For all disease syndromes, mortality decreased with longer treatment duration until a nadir, which was the treatment duration associated with the lowest proportion of patients with adverse long-term outcomes. Thereafter, mortality increased with longer duration of therapy. |
| INH Resistance | Overall US INH resistance rate 8.9% (2012). Areas where INH resistance >4% need to add 4th drug, ethambutol CT INH resistance 13.2% (7 cases, 2012) Due to alterations in the KatG per oxidase-catalase; INH is not activated Less commonly, may be die to altered enzymes -- enoyl-acyl carrier protein reductase (InhA) and acyl carrier protein B-ketoacyl-ACP synthase. Risk factors for resistance: History of prior TB, Asican/Pacific Islander, age >65, foreign born. |
| Rifampin Resistance | Uncommon by itself. Usually associated with multi drug resistance with INH. 1.1% in US (2012) 1 case in CT (2012). Due to point mutations in the polymerase gene (B-subunit rpoB) Risk factors for INH and RIfampin resistance are prior TB history, foreign born. |
| Preventing Multidrug Rresistant - TB | Use of appropriate drug regimen up front. 4 drugs in most of US NEVER ADD ONE DRUG TO A FAILING REGIMEN Most US MDR cases result from inconsistent or incomplete therapy as opposed to patient to patient transmission. Not true in other countries where patient to patient transmission can and does occur. |
| Cross Drug Resistance - TB | Resistance to INH and Rifampin AND Resistance to any Fluoroquinolone AND Resistance to any ont of the second line injectable drugs (amikacin, capreomycin, kanamycin) |
| DOT (Directly observed therapy) Optimizing adherence | DOT should be the default method for medication administration Contact local public health department. May contract out to local VNA services. With enhanced DOT 90.2%. Of patients completed therapy as opposed to only 61.4% completeion rate of unsupervised therapy. |
| TB Discharge Planning Connecticut State Law | Requires pre-discharge collaborative planning with public health officials before a patient with active TB can be discharged from the hospital. The local public health department must approve the discharge plan. TB patient Hospital/Discharge Management Plan must be completed before discharge. |
| Alternative TB Agents Rifabutin | Useful in lieu of rifampin if patient is on ART with a PI. Can only be used with Efavirenz, Raltegravir, Dolutegravir Half Life: 36-45 hours Dose: Oral, must adjust with concomitant PI or NNRTI use Metabolism: Hepatic Bioavailability: Fair (53%) |
| Alternative TB Agents Rifabutin Toxicity | Uveitis: noted with concomitant clarithromycin use in MAI treatment trials of AIDS patients. Fluconazole also implicated. Inhbition of cyp3A4 by Fluconazole or clarithromycin resulting in elevated Rifabutin levels. Rash Orange-red discoloration of body fluids Significant drug-drug interactions due to induction of cyp34A (less than rifampin) |
| Alternative TB Agents Quinolones | Moxifloxacin is the most active of the commercially available Quinolones against MTB and other mycobacteria. Bacteriocidal Effect in MTB similar to that of INH. |
| Alternative TB Agents Quinolones Moxifloxacin | Similar to Rifampin in velocity of killing. EBA similar to that of INH. Additional agent when NDR-TB suspected. Useful when 2st line drugs not tolerated. When strain resistant to INH, rifampin or ethambutol AND fluorquinalone susceptible. CNS disease. |
| Alternative TB Agents Aminoglycosides Streptomycin | Equivalent to ethambutol when used in initial phase of 6 month regimens Resistance in areas of the world where MTB is highly prevalent, limits its utility. |
| Alternative TB Agents Aminoglycosides Streptomycin Dosing | Dose adjusted for age and GFR IV administration Administer daily then reduce to 2-3x/week after 2-4 months of treatment or culture conversion Levels are available by send out chemistry |
| Alternative TB Agents Aminoglycosides Streptomycin Toxicity | Ototoxicity Vestibulotoxicity Neurotoxicity: Circumoral par atheists when infused; increase diffusion duration to 60 minutes. Nephrotoxicity: Less common compared to other aminoglycosides (2%) |
| Alternative TB Agents Cycloserine | Bacteriocidal Inhibits cell wal biosynthesis by inhibiting racemase which converts l-ala to d-ala Dose: oral Metabolism: liver (35%) Excretion: renal (50-70%). Do not use if GFR<50 unless patient on hemodialysis. Half Life: 10-25 hours Bioavailability: 100% |
| Alternative TB Agents Cycloserine Toxicity | CNS: Headache, restless ness to psychosis or seizures. Contraindicated in patient with known seizure disorder. Acts as a partial agonist at the glycine recognition site of NMDA receptor. B6 may help prevent/Treat CNS side effects. Peak serum level should not exceed 20ug/ml |
| Alternative TB Agents Ethionamide | Prodrugs activated by ethA Similar to isoniazid Inhibits my colic acid synthesis Dose: oral Half Life: 1.9 hours Metabolism: Hepatic Bioavailability: 100% |
| Alternative TB Agents Ethionamide Toxicity | GI: Metalic taste, nausea, vomiting (severe), loss of appetite, abdominal pain. Symptoms reduced if taken with food. Better tolerated if titrated dose over a few days. Maybe better tolerated if split dose into w. Hepatotoxicity: similar to INH, up to 2% Neurotoxicity: Peripheral neuropathy, optic neuritis, depression, personality changes. Administer with B6 to reduce risk Endocrine: hypothyroidism, hypoglycemia, gynecomastia Caution wth concomitant admin with cyclosporine - increased risk of seizures |
| Alternative TB Agents P-Aminosalicylic acid (PAS) | Bacteriostatic Inhibits folate metabolism Dose: Oral Half Life: 1.1-1.6 hours Metabolism: Hepatic (acetylation) then excreted into the urine (8-% Bioavailability: 60-65% |
| Alternative TB Agents P-Aminosalicyclic acid (PAS) Toxicity | GI: Intolurance due to N/V, diarrhea Hepatotoxicity: .3% Malabsorption syndrome: Steatorrhea, low serum folate levels Hypothyroidism: Especially in combination with Ethionamide. Coagulopothy: elevated PT |
| Other TB Medications Amikacin Capreomycin | Amikacin: Helpful even in streptomycin resistant isolates Dose: IV Capreomycin: Used during amikacin shortage. Problems of magnesium and potassium wasting |
| Other TB Medications Linezolid | Problems related to dose Safety Cost |
| Other TB Medications Bedaquiline | Diarylquinolone Used for treatment of MDR-TB Inhibits mycobacteria L ATP synthase Half Life: 5.5 months Dose: Oral Metabolism: Hepatic, cyp3A4 Bioavailability: 36-79% (food increases bioavailability 2 fold) |
| Other TB Medications Bedaquiline Risk | Increased risk of death QT prolongation Transaminitis (11%) |
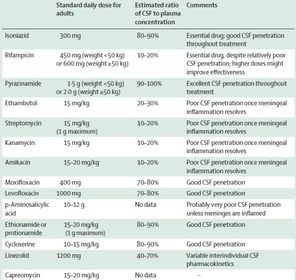
| CNS Penetration of Anti - TB Agents |
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.