6304613
Description
Flashcards by Michelle Evans, updated more than 1 year ago
|
|
Created by Michelle Evans
over 8 years ago
|
|
| Question | Answer |
| What tube do you use for a serum chemistry panel? | A red top tube |
| Does a red top tube contain anticoagulant? | No; want the blood to clot so that you can separate the serum and run a biochemistry panel |
| What is the purpose of a tiger-top (red/grey) tube? | Also for serum biochemistry; separates the blood and the serum within the same tube (same tests as red top tube) |
| Which tube contains the anticoagulant EDTA with potassium salt? What is the purpose of EDTA? | Lavender top tubes Used to collect blood for CBC, fluids EDTA chelates Ca2+ and prevents coagulation in the tube (preserves cell morphology) |
| Which tube is used for coagulation testing? | Blue top tube |
| What additives does the blue top tube contain? What is their purpose? | Contains anticoagulatnt sodium citrate Weakly chelates Ca2+ Then add calcium back to see how clotting precedes |
| What is a common mistake when filling a blue top tube? | Not using the precise volume of blood; need a 9:1 ratio of blood to citrate Under fill tube, get too much anticoagulant Will use up all the Ca2+ and invalidate the test |
| Which tube is used for glucose collection, if the sample is going to ship and can't be spun? | Grey top tube |
| What additives are in the grey top tube? What are their purpose? | Sodium fluoride Inhibits glucose metabolism in cells so that you can determine the glucose concentration in the cells |
| What is the purpose a green top tube? | Use in large animal, avian, and reptile serum biochemistry Other specific tests like lead concentration, blood gas panels |
| What additives are in the green top tube? What are their purposes? | Contains the anticoagulant heparin Prevents thrombin from promoting fibrin formation |
| Why shouldn't you refrigerate a blood film or freeze a blood sample? | Will get cell lysis Artificially low PCV, high Hgb |
| You see a sample with very swollen red blood cells and degraded leukocytes. What error was made to leave to these changes? | Left the sample sitting at room temperature for 24 hours or more |
| If you under fill a lavender top tube, what changes in CBC results? | Will have decreased PCV and MCV due to erythrocyte shrinkage |
| You have a sample that is taking an extremely long time to clot. Assuming the animal does not have a clotting disorder, what could explain these results? | Too little blood was added to the blue top tube, and the sodium citrate ate the Ca2+ that was added back into the tube to initiate coagulation |
| What is packed cell volume (PCV)? | The percentage of whole blood that is composed of erythrocytes Measured after centrifugation to maximally pack RBC |
| What is the purpose of plasma protein refractometry? | Estimates the protein concentration in plasma (assuming that other solutes are present in their normal concentration) |
| What factors can alter the results of protein concentration estimate? | Lipemia and severe hemolysis |
| What does an increase in blood albumin indicate? | Dehydration; not due to increased production in albumin |
| Increased PCV and increased TP indicate: | Dehydration |
| Decreased PCV and decreased TP indicate: | Blood loss |
| PCV is WNL, TP is decreased: | Decreased protein production, increased protein loss |
| PCV is WNL, TP is increased: | Increased globulin production, dehydration in an anemic patient |
| PCV decreased, TP is WNL: | Anemia of chronic disease or hemolysis |
| PCV increased, TP is WNL | Dehydration in an animal with low TP or polycythemia (increased cell production) |
| Which is more useful: the percentage of nucleated cells that belong to each cell type, or the absolute concentration of each cell type? | The absolute concentration The percentage can be WNL, but if we have lost all the cells the percentage isn't useful to us (won't reflect this loss) |
| What is the best technique for blood film preparation? | "Push" technique Use two slides; increase angle if animal is anemic; push quickly to get a thin film across the slide |
| Which area of the blood film do you examine to find large items, such as microfilariae and aggregated platelets? | The feathered edge Large objects will be pushed here as the slide is prepared |
| What determines if an anemia is regenerative? | The presence of reticulocytes (young, immature erythrocytes that still contain some RNA from organelles); visualized with methylene blue stain |
| Which species never release reticulocytes in response to anemia? | Horses Anemia may be regenerative, but will not see reticulocytes in the peripheral blood |
| In cats, which form of reticulocytes are important for determining if regeneration is ongoing? | The aggregate form Aggregate forms mature in about 12 hrs, then the punctate take weeks to mature; only aggregate reticulocytes indicate an ongoing regeneration |
| What is the buffy coat? | The white band on a centrifuged sample between the serum and the RBC Contains leukocytes, nucleated erythrocytes, platelets |
| What does yellow pigmented serum indicate? | This serum is icteric Indicated that there is increased bilirubin (icterus) or may just be carotene in large animals (pigment from food) |
| What does white opaque plasma indicate? | This plasma is lipemic; there are increased chylomicrons in the plasma Can be due to a postprandial collection, or due to diseases with abnormalities in lipid metabolism |
| What does red plasma indicate? | Hemolysis Can be in vitro or in vivo If PCV not decreased, probably in vitro (consider it an artifact) If in vivo = hemolytic anemia |
| What are the components of a CBC? | Leukogram, Eyrthrogram, Thrombogram, Total Protein |
| What parameters are included in the erythrogram? | RBC count, PCV, [Hgb], RBC parameters (MCV, MCHC, RDW), RBC morphology +/- reticulocyte count |
| Which parameters are directly measured? | Nucleated cell count, RBC count, Hgb, MCV, Platelet count, MPV, plasma protein, fibrinogen |
| Which parameters are determined via microscope examination? | Differential nucleated cell count; morphology of RBC, WBC, platelets; reticulocyte enumeration |
| What parameters in a CBC are calculated? | Absolute [WBC], hematocrit, RDW |
| A decrease in which parameters indicates anemia? | RCB, Hct, PCV, Hgb |
| What does an increased in mean cell volume (MCV) indicate? | Macrocytosis Can be due to a regenerative response to anemia (polychromatophils are larger than mature RBC) |
| In a cat with macrocytosis (increased MCV) and a non-regenerative anemia, what disease do you consider as a top differential diagnosis? | FeLV |
| What does a decreased MCV indicate? | Microcytosis Iron deficiency or portosystemic shunt Can be seen in a chronic inflammatory response when macrophages sequester iron |
| What is the MCHC? | The mean cell hemoglobin concentration , or the average amount of hemoglobin in a RBC |
| What does an increased MCHC indicate? | Hemolysis (more Hgb in the blood, get an increased calculation) Never hyperchromic Cannot get increased Hgb in a RBC |
| What does a decreased MCHC indicate? | Decreased MCHC = hypochromia Indicates cell swelling Dilutes the Hgb as the volume increases, [Hgb] remains the same |
| What is the RDW? What does an increase in this parameter indicate? | Red cell distribution width; tells you the variation in size of red blood cells Increased RDW indicates a high degree of anisocytosis; variable RBC size |
| What information does the reticulocyte count give you? | Tells you whether or not an anemia is regenerative |
| What does an increase in the reticulocyte count indicate? | A regenerative anemia The bone marrow is producing many new RBC to try and make up for the deficit |
| What does a decreased reticulocyte count, or a reticulocyte count that is not increased in an anemic animal, indicate? | That red blood cells are not regenerating A non-regenerative anemia can be due to issues in the bone marrow |
| What is a hypochromic RBC? | A red blood cell with decreased [Hgb], appears to have less color and a larger central pallor |
| What CBC parameter confirms whether an anemia is hypochromic or normocrhomic? | MCHC The color of the RBC is determined by the [Hgb] |
| What is anisocytosis? | Variation in cell size |
| What CBC parameter determines the degree of anisocytosis? | RDW |
| What is poikilocytosis? | Variation in cell shape |
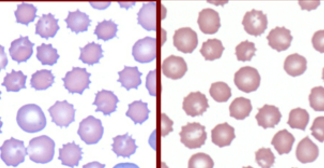
| What are these cells? | Echinocytes |
| What are echinocytes? | Crenated cells; dehydrated RBC that have the same amount of membrane but decreased volume Most common shape change (usually artifact); can be caused by severe electrolyte imbalances, uremia |
| Rattlesnake envenomation is associated with what shape change in RBC? | Type III Echinocytes Very fine spikes |
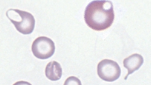
| What is this RBC shape called? | Acanthocyte |
| What disease process is associated with the presence of acanthocytes? | Hemangiosarcoma Any microangiopathic process that creates newly formed vessels for RBC to travel through |
| Keratocytes are indicative of which kinds of processes? | Oxidative Injury Iron deficiency |
| What is the term for these kinds of cells? | Keratocytes Have a vacuole that forms in the RBC; breaks open and creates a horn-like projection |
| What are schistocytes? What are they caused by? | RBC fragments Likely due to shearing in intravascular trauma DIC; microangiopathic disorders; iron deficiency |
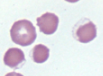
| What are spherocytes pathognomonic for? | Immune-mediated processes such as immune-mediated hemolytic anemia Shape change is caused by membrane damage due to attack by immune system |
| What are these cells? | Spherocytes RBC with membrane damage that ball up; no longer a biconcave disc; no area of central pallor |
| What are these cells? | Eccentrocytes Hgb is eccentrically placed within the cell; it fuses with the erythrocyte membrane |
| What process causes eccentrocytes? | Oxidative damage, either from toxins or endogenous issues |
| What processes can lead to increased nucleated red blood cells (nRBC) in the peripheral blood? | Splenectomy (nucleus can be removed in spleen, no spleen --> no removal) Regeneration (with polychromasia) Lead poisoning Bone marrow injury FeLV, erytholeukemia |
| You see nRBC with no significant polychromasia -- what disease processes are you concerned about? | FeLV or erythroleukemia |
| What is a Howell-Jolly body? | Small nuclear remnant Appears as a small, dark purple spot in a low number of erythrocytes |
| What is cellular feature is often seen in ruminant regenerative responses? | Basophilic stippling |
| If you see basophilic stippling with few other signs of regeneration, or without anemia, what should you worry about? | Lead poisoning |
| How do you distinguish intracellular bacteria, like Anaplasma, from Howell-Jolly bodies? | Bacteria will be present in many more RBC; Howell-Jolly bodies occur only occasionally. |
| Mycoplasma is important in which domestic species? | Cats |
| A large, tear-shaped inclusion in a canine RBC is indicative of which intracellular parasite? | Babesia |
| What are Heinz bodies? | Denatured Hgb due to oxidative injury Form most easily in cats May or may not protrude from the erythrocyte |
| What stain can be used to determine if Heinz bodies are present? | Use a reticulocyte stain, can be easily visualized |
| What causes agglutination? | Cells will arrange in grape-like clusters due to antibody bridging Some kind of immune-mediate process |
| What is anemia? | Decrease in RBC mass Results in decreased tissue oxygenation |
| What parameters are used to assess anemia? | PCV, Hgb, [RBC] Values should all change together since they basically measure the same thing (if not, there is an error in the analysis) |
| What are the three causes of anemia? | RBCs are being lost (hemorrhage) RBCs are being destroyed RBCs aren't being made |
| If regeneration is present, what are the possible causes of the anemia? | Blood loss or destruction of RBC |
| If no regeneration is present, what do you know about the anemia? | Either that the bone marrow is not producing RBC like it should, or that reticulocytes are being destroyed in the marrow before they are released. May also have caught the anemia early, before regeneration starts. |
| If plasma protein is decreased in the presence of anemia, what is the most likely cause of anemia? | Blood loss or hemorrhage Plasma proteins and RBC will be lost in the blood |
| What does macrocytosis indicate in anemia? | May indicate a regenerative response (retiuclocytes and other young RBC are larger than mature RBCs) If no reticulocytes present, may indicate FeLV or another myeloproliferative disorder. |
| What does hypochromasia indicate? | Often seen with regenerative anemia, since reticulocytes are still obtaining Hgb Can be seen with iron deficiency (if RBCs are microcytic) |
| What signs found during a physical exam can be indicative of anemia due to blood loss? | Bruising, petechia (can be platelet dysfunction or coagulation disorder) Abdominal distension (internal bleeding) |
| What sign found during a physical exam can be indicative of anemia due to hemolysis? | Icteric mucous membranes |
| If the bone marrow is responding to an anemia and regenerating RBCs, what should the reticulocyte be? | Above average Production needs to increase in order to keep up with the decreased [RBC] |
| A macrocytic, non-regenerative anemia is indicative of which disease processes? | FeLV Myeloproliferative disorders |
| What is pancytopenia? | Aplastic anemia -- lack of any regeneration. Decrease in all cell lines Caused by stem cell injury or suppression. |
| What can cause pancytopenia? | Drugs (chemotherapeutic agents, estrogens) Toxins Infectious agents (FeLV, Erlichia canis, Equine infectious anemia, parvo) |
| In pancytopenia, which cell lines will decrease first? | Neutrophils and platelets (lifespan hours to days); RBC can live for months, won't see a decrease for a bit |
| What is pure red blood cell aplasia? | Severe anemia due to lack of erythroid precursors without decreased neutrophils or platelets Can be immune-mediated destruction of erythroid precursors or FeLV |
| What is RBC hypoplasia? | Decreased RBC production due to external influences -- most common cause of non-regenerative anemia Can be inflammatory disease, renal failure, or endocrine diseases |
| Does chronic inflammatory disease cause regenerative or non-regenerative anemia? | Non-regenerative |
| What is the mechanism of anemia due to inflammatory disease? | Cytokine production causes decreased production of RBC Cytokines cause iron sequestration, leaving less available for erythroid production |
| Why is anemia common in animals with renal failure? | Erythropoietin comes from the kidney and is essential for RBC production; without EPO, will get decreased RBC production |
| How do endocrine diseases cause non-regenerative anemia? | Related to altered metabolism, trophic factors See with hypothyroidism and hyperadrenocorticism |
| Non-regenerative anemia with neutrophilia, left shift, and monocytosis is most likely caused by: | Chronic inflammation |
| What are some causes of pancytopenia? | Stem cell injury Myelophtistic disease (neoplastic cells crowding in the bone marrow) Hemophagocytic syndrome (macrophages eat the precursors) |
| If you have a non-regenerative anemia with azotemia (increased BUN, creatinine), the most likely cause of anemia is: | Renal failure |
| What is the benefit of looking at the bone marrow (via aspirate or core biopsy) during non-regenrative anemia? | Can assess if erythroid precursors are present and if there is evidence of regeneration |
| If a bone marrow aspiration shows dysplatic maturation of RBC, the most likely cause of anemia is: | FeLV Myeloproliferative disease |
| If a bone marrow aspiration shows precursors present in high numbers, but there are no signs of regeneration in the peripheral blood, the anemia is most likely due to: | Immune mediated destruction of precursors in bone marrow |
| In what species can you not use iron stores in the bone marrow to determine if anemia is due to chronic inflammation? | Cats -- don't store iron in bone marrow |
| What is regenerative anemia? | An anemia where the bone marrow is still producing erythroid precursors, trying to combat the anemia by releasing more RBCs |
| What are causes of regenerative anemia? | Blood loss Erythrocyte destruction Recovery fro reversible bone marrow dysfunction or stem cell injury |
| If you see regenerative anemia with low protein concentration, the top differential for the anemia is: | Blood loss |
| In acute blood loss, what signs are seen? | If very acute, PCV and protein may be normal. Later, interstitial fluid moves into vessels to maintain blood volume, get decreased concentrations of erythrocytes and protein. May take awhile to see regeneration |
| Chronic blood loss should lead to: | Strongly regenerative anemia May result in iron deficiency if blood is loss form the body |
| What are the causes of chronic blood loss anemia? | Blood sucking parasites GI ulcers and neoplasms IBD Intermittent bleeding due to thrombocytopenia, inherited coagulopathy, bleeding tumor |
| What is the most common site associated with chronic blood loss? | GI system |
| What are the signs of iron deficiency? | Microcytosis MCV decreased RDW increased MCHC normal or decreased Blood film examination (increased central pallor, keratocytes/schistocytes) Thrombocytosis |
| What are is main causes of blood cell destruction? | Immune system either directly attacking RBC or other immune complexes that attach to RBC Infection, vaccination, neoplasia, drug toxicities, autoimmune disease |
| Destruction of RBC leads to what kind of anemia? | Regenerative |
| What is the mechanism for intravascular hemolysis? | Occurs through complement fixation and the membrane attack complex Hgb leaks from RBC --> ghost cells MCHC increased due to free Hgb in plasma |
| What is the mechanism for extravascular hemolysis? | Macrophages in liver, spleen, bone marrow phagocytize erythrocytes |
| What are signs are pathognomonic for IMHA? | Spherocytes Agglutination |
| What is the mechanism of IMHA? | Antibodies attach to RBC membrane Macrophages recognize this Phagocytize and destroy RBC |
| What is a Coomb's test? | Test for IMHA Create antibodies to the auto-antibodies found in IMHA If a patient has these auto-antibodies, the test will result in agglutination |
| What is neonatal isoerythrolysis? | Immune-mediated destruction of erythrocytes in newborns Maternal antibodies attacking offspring's RBC |
| How do baby's obtain maternal antibodies in neonatal isoerythrolysis? | In colostrum If you prevent the baby from nursing for 24 hrs, or give it colostrum from another mare, can prevent transfer of antibodies |
| Why is neonatal isoerythrolysis common in mule foals? | Donkeys have antigen that horses don't on their RBC; if baby gets mare colostrum, will get RBC lysis |
| How do you diagnose infectious causes of anemia? | PCR Blood film |
| Are Mycoplasma intracellular or extracellular bacteria? | Extracellular Adhere loosely to RBC membrane Can fall of erythrocytes and be seen in plasma |
| What is an infectious cause of acute hemolytic anemia in cats? | Mycoplasma haemofelis |
| Why are splenectomized dogs more likely to get disease from Mycoplasma haemocanis? | Normally the spleen is very effective at removing the bacteria from the RBC; without a spleen, will get many more bacteria in the blood |
| What is an infectious cause of severe hemolytic anemia in cattle? | Anaplasma marginale |
| Is Anaplasma intracellular or extracellular? | Intracellular Lives within the RBC |
| What is the mostly likely cause of a tear-shaped intraerythrocytic organism visualized on a canine blood smear? | Babesia |
| What does Babesia cause in horses? | Piroplasmosis |
| What is a protozoal cause of hemolytic anemia in ruminants? | Theileria |
| What is a protozoal cause of hemolytic anemia in cats? | Cytauxzoon felis |
| A cat presents with hemolytic, nonregenerative anemia, keuopenia, thrombocytopenia, and organisms visible within the RBC and macrophages. What is the most likely cause? | Cytauxzoon felis |
| What is a consequence of macrophages phagocytizing Cytauxzoon felis? | Build up macrophages in bone marrow and blood vessels Get vessel damage and thrombosis |
| What species is most likely to get Heinz body anemia? Why? | Cats Have a hemoglobin structure that is more susceptible to oxidation |
| What is the cause of Heinz body anemia? | Oxidative damage to hemoglobin |
| Why do animals with Heinz body occasionally have elevated MCHC? | Heinz bodies interfere with measurement of hemoglobin |
| How doe water intoxication lead to hemolytic anemia? | After period of severe dehydration, RBC will be hyperosmolar Give unlimited water, water moves into hyperosmolar cells --> swelling, lysis |
| What is polycythemia? | Increase in erythrocyte mass |
| What are relative causes of polycythemia? | Dehydration (Concentrates RBC and protein) Splenic contraction (Common in horses and cats; release of sequestered RBC into circulation for short period of time) |
| What is absolute polycythemia? | Total erythrocyte mass is actually increased |
| What is relative polycythemia? | RBC mass is not truly increased; either transient increase in amount in circulation, or just concentrated due to dehydration. |
| What is primary absolute polycythemia? | Uncontrolled production of erythrocytes |
| What myeloproliferative disorder describes a chronic leukemia of erythroctes? | Polycythemia vera |
| What is secondary primary polycythemia? | Bone marrow is increasing production of RBC in response to elevated erythropoietin |
| What is appropriate secondary polycythemia? | Chronic lung or heart disease causes hypoxia that is detected by kidney Kidney released EPO in response to hypoxia to increase RBC in circulation (bring more oxygen to tissues) |
| What is inappropriate polycythemia? | A tumor in the kidney causes an area of local hypoxia, causing a release in EPO Don't actually need more RBC; not a systemic hypoxia. |
| What is MPV? Why can this value be clinically significant? | Mean Platelet Value If increased, probably regenerating platelets (bone marrow releasing larger precursors in response to thrombocytopenia) |
| What is thrombocytopenia? | Platelet count less than reference interval |
| When you see thrombocytopenia without clinical signs, is the most likely cause something pathologic in the animal? | No Look for clots in the tubes, platelet clumps on blood smear |
| Causes of Thrombocytopenia | Platelets being consumed (DIC, vasculitis, hemangiosarcoma) Platelets being destroyed (IMHA, Erhlichia) Platelets aren't being made (Bone marrow toxicity, stem cell injury) |
| An animal presents with severe hemorrhage and bleeding. Do you worry about thrombocytopenia with this patient? | No; blood loss rarely leads to thrombocytopenia If present with blood loss, usually thrombocytopenia first and hemorrhage second |
| What are the indications for bone marrow aspiration? | Unexplained cytopenia (neutropenia, non-regenerative anemia, thrombocytopenia, pancytopenia), abnormal cell mrophologies (WBC blasts, dacrocytosis of RBC), abnormal cell population (excessive nRBCs), diagnosing, staging, and monitoring neoplasia, PE finding (fever unknown origin, lytic bone lesions) |
| What type of anemia is an indication for a bone marrow aspirate? | Non-regenerative Anemia With no signs of inflammation, chronic renal failure, or endocrine disease |
| What is the advantage of a bone marrow aspirate? | Better ID and evaluation of individual cell morphology Faster turn around (no special stain) |
| What are the advantages of core biopsy? | More accurate for determining true cellularity of bone Better at discerning fibrosis, amyloidosis May be more sensitive to detecting infiltrative disorders |
| Why should you stop aspirating as soon as the bone marrow sample starts entering the syringe? | Don't want to get hemodilution of the sample Will just begin getting blood, no more cells; artificially dilutes your sample |
| True or false: Bone marrow aspiration is a useful diagnosis tool without any other tests. | False; need a CBC to understand findings. Everything is relative, interpretation is based on abnormalities in peripheral blood |
| What is the M:E ratio? | The ratio of myeloid and erythroid cells in a bone marrow aspirate or core biopsy |
| What is an increased M:E ratio? | More myeloid cells than erythroid cells Either myeloid cells are being produced excessively, or erythroid cells are not being produced enough |
| What is a decreased M:E ratio? | More erythroid cells than myeloid cells Either more erythroid cells being produced, or not enough erythroid cells being produced |
| If an anemia is due to a lack of production, what would you expect to see in the bone marrow? | You would expect the bone marrow to be hypoplastic, since a lack of production indicates that not enough RBC are being produced |
| If a cytopenia is caused by consumption, what do you expect to see in the bone marrow? | Expect the bone marrow to be hyperplastic, trying to replace the cells that are being consumed |
| If a cytopenia is due to destruction, what do you expect to see in the bone marrow? | Expect the bone marrow to be hyperplastic (replacing the cells that are being destroyed) unless the precursors are being attacked in the bone marrow. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.