7386448
Description
Flashcards by Andrew Street, updated more than 1 year ago
|
|
Created by Andrew Street
almost 8 years ago
|
|
| Question | Answer |
| Laryngeal & tracheal infxn's cause mucosal inflammation & swelling. This can rapidly cause life-threatening obstruction of the airway in young children. Several conditions can cause acute upper airways obstruction - what are they? | Common causes: * Viral laryngotracheobronchitis (‘croup’ – very common) Rare causes: * Epiglottitis * Bacterial tracheitis * Inhalation of smoke & hot air in fires * Trauma to throat * Retropharyngeal abscess * Laryngeal foreign body * Allergic laryngeal angioedema (seen in anaphylaxis & recurrent croup) * Hypocalcaemia due to poor vitamin D intake * Infectious mononucleosis causing severe lymph node swelling * Measles * Diphtheria ITOP p280. |
| Laryngeal & tracheal infxn's are characterised by what signs? | * Stridor * Hoarseness due to inflammation of the vocal cords * A barking cough like a sea lion * A variable degree of dyspnoea ITOP p280. |
| How is upper airway obstruction assessed for severity? | **Do NOT examine the throat!** Take a careful assessment of severity including: * Degree of stridor & subcostal recession (none, only on crying, at rest or biphasic (stridor only)) * RR * HR * LOC, tiredness, & exhaustion * Pulse oximetry OHOP |
| With laryngotracheobronchitis (croup), there is mucosal inflammation & ^secretions affecting the airway, but it is oedema of subglottic area that is potentially dangerous in young children as it may result in critical narrowing of trachea. What are the common causes of croup & when is the peak incidence? | Viral croup accounts for >95% of laryngotracheal infections. Parainfluenza viruses are commonest cause. Other causes - human metapneumovirus, RSV & influenza - can produce a similar picture. Occurs from 6/12-6 YO but peak incidence is in second year of life. ITOP p280. |
| What are typical features of croup? | * Barking cough * Harsh stridor & hoarseness * Usually preceded by fever & coryza * Sx often start, & are worse, at night ITOP p280. |
| Mx of croup. | Mild illness - Mx at home. Advise parents that if recession & stridor at rest then return to hospital. Infants <12mths may need closer attention. Rx includes the following: * Moist or humidified air - widely used but unproven * Steroids - oral prednisolone (2mg/kg for 3 days) or oral dexamethasone (0.15mg/kg stat dose) or nebulized budesonide (2mg stat dose) reduces severity & duration of croup. Also likely to reduce need for ET intubation. OHOP • Nebulized adrenaline (epinephrine): can provide transient relief of symptoms. In cases that require endotracheal intubation steroids should be given and, if there is evidence of secondary bacterial infection or bacterial tracheitis, antibiotics should be added. |
| Acute epiglottitis is a life-threatening emergency. Caused by H. influenzae type b. In UK introduction of universal Hib immunisation has led to a >99% reduction in incidence of epiglottitis. There is intense swelling of the epiglottis & surrounding tissues associated with septicaemia. What is the peak age of incidence & key signs & Sx? | Most common in 1–6 YO's but affects all age groups. The onset of epiglottitis is often very acute with: * High fever in an ill, toxic-looking child * Intensely P'ful throat that prevents child from speaking or swallowing * Saliva drools down chin * Soft inspiratory stridor & rapidly ^respiratory difficulty over hours * Child sits immobile, upright, with an open mouth to optimise airway * In contrast to croup, cough is minimal/absent ITOP p281. |
| Mx of acute epiglottitis. | Mx in ITU after ET intubation. Once intubated take BD cultures & start IV ABx. * 2nd or 3rd generation cephalosporin (eg cefuroxime, ceftriaxome, or cefotaxime) IV for 7–10/7 * Rifampicin prophylaxis to close contacts OHOP |
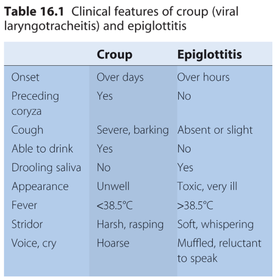
| Outline differences in clinical features between croup & acute epiglottitis. Box from ITOP p281. |
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.