7491350
Description
Flashcards by Andrew Street, updated more than 1 year ago
|
|
Created by Andrew Street
almost 8 years ago
|
|
| Question | Answer |
| What is developmental dysplasia of the hip (DDH)? | Disorder of hip joint development resulting in hip instability/subluxation/dislocation leading to acetabular dysplasia. OHOP |
| Incidence: 2:1000 (but up to 20:1000 newborn hips are unstable; 90% spontaneously stabilize by 9/52). What are the risk factors? | * FHx (1:5) * Female > male (5:1) * L > R (1.5:1) * Racial predilection * Breech presentation OHOP |
| DS progression = Capsular laxity + shallow acetabulum → instability/subluxation/dislocation → muscle contracture → progressive acetabular dysplasia with a fibrofatty substance filling the acetabulum; femoral head becomes hypoplastic. What is the typical Hx? | * Usually uneventful pregnancy * Parents may notice delayed walking * P'less limp * Prone to falls * DDH may be incidental finding OHOP |
| All newborn infants are screened for DDH before discharge. Describe how you would perform Ortolani's & Barlow's test. | * Is hip dislocated? If so, is it reducible? Ortolani’s test (O for out). Gently elevate (anteriorly) & abduct the dislocated hip to reduce it (clunk of reduction). * If not dislocated, can I dislocate it (ie dislocatable)? Barlow’s test. Gently adduct & depress (posteriorly) femur, vulnerable hip dislocates. These 2 provocation manoeuvres become unreliable after age 6–8/52. OHOP |
| Ix of DDH pre & post 6/12. | * <6/12 - hip US (before ossification, operator-dependent) * >6/12 - AP pelvis radiograph. A shallow acetabulum with ^acetabular index & hypoplastic femoral head in superolateral position is demonstrated OHOP |
| Rx of DDH. | * <6/12: > Pavlik harness (maintain hip in flexed position with some hip abduction) * Age 6–18/12: > Manipulation & closed reduction (+/− adductor tenotomy) + hip spica plaster cast > Open reduction + hip spica plaster cast * 18–24/12: > Trial of closed reduction > Open reduction +/− pelvic osteotomy + hip spica plaster cast * 2–6yrs: > Open reduction +/− femoral shortening +/− pelvic osteotomy + hip spica plaster cast OHOP |
| What is postional talipes & how is it corrected? | * Caused by intrauterine compression - is common * Foot is of normal size * Deformity is mild * Can be corrected to neutral position with passive manipulation * If positional deformity is marked parents can be shown passive exercises by physiotherapist ITOP p453. |
| What is talipes equinovarus? | * Entire foot is inverted & supinated, forefoot adducted & heel is rotated inwards & in plantar flexion * Affected foot is shorter * Calf muscles thinner than normal * Position of foot is fixed, cannot be corrected completely & often bilateral * Birth prevalence is 1:1000 live births, affects predominantly males (2:1), can be familial & usually idiopathic See pics on following cards. OHOP |
| Rx of talipes equinovarus. | Rx is started promptly with plaster casting & bracing, may be required for many months. Usually successful unless condition is very severe, when corrective SX is required. ITOP p453. |
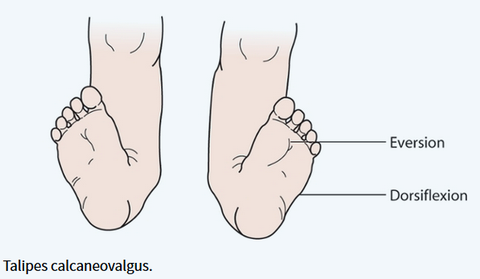
| What is talipes calcaneovalgus? | Foot is dorsiflexed & everted. Usually results from intrauterine moulding & self-corrects. Passive foot exercises are sometimes advised. ITOP p453. |
| Poo I'm soo bored. |
{kind=link}
{kind=link}
{kind=link}
Want to create your own Flashcards for free with GoConqr? Learn more.