10769422
Description
Mind Map by Menna Emam, updated more than 1 year ago
|
|
Created by Menna Emam
about 7 years ago
|
|
Aisha is not feeling well
- later diagnosed with
- congestive heart failure
- occurs when
- The heart is unable to pump
blood at a rate that meets the
metabolic requirements of
the peripheral tissue;
inadequate cardiac output is
usually accompanied by
increased congestion of the
relevant venous circulation.
- The heart is unable to pump
blood at a rate that meets the
metabolic requirements of
the peripheral tissue;
inadequate cardiac output is
usually accompanied by
increased congestion of the
relevant venous circulation.
- Classification
- Left-sided versus right-sided failure
- Left ventricular failure and right ventricular failure
can occur independantly or together as congestive
cardiac failure
- RVH
- LVF
- Pulmonary stenosis
- Lung disease
- Symptoms
- Peripheral edema
- Ascites
- Nausea
- Facial engorgement
- Pulsation in neck and face
- Epistaxis
- Epistaxis
- Pulsation in neck and face
- Facial engorgement
- Nausea
- Ascites
- Peripheral edema
- Symptoms
- Lung disease
- Pulmonary stenosis
- LVF
- LVH
- Dyspnea
- Poor exercise tolerance
- fatigue
- Orthopnea
- PND
- Nocturnal cough
- Wheeze
- Muscle wasting
- Weight loss
- Cold peripheries
- Nocturia
- Nocturia
- Cold peripheries
- Weight loss
- Muscle wasting
- Wheeze
- Nocturnal cough
- PND
- Orthopnea
- fatigue
- Poor exercise tolerance
- Dyspnea
- Left ventricular failure and right ventricular failure
can occur independantly or together as congestive
cardiac failure
- Low-output versus high-output failure
- High-output heart failure
- Output is normal or
increased with increased
needs. Failure occurs when
cardiac output fails to
meet these needs. Occ- urs
with a normal heart but
ear- lier if there is heart
disease.
- Consequence
- Initially features of
RVF, then LVF becomes
evident
- Initially features of
RVF, then LVF becomes
evident
- Causes
- Anemia
- pregnancy
- Hyperthyroidism
- Paget's disease
- Paget's disease
- Hyperthyroidism
- pregnancy
- Anemia
- Consequence
- Output is normal or
increased with increased
needs. Failure occurs when
cardiac output fails to
meet these needs. Occ- urs
with a normal heart but
ear- lier if there is heart
disease.
- Low-output heart failure
- Cardiac output is decreased and fails to
increase normally with exertion.
- Causes
- Pump failure
- Systolic ordistolic
- Heart failure
- decreased HR
- decreased HR
- Heart failure
- Systolic ordistolic
- Excessive overload
- MR
- fluid overload
- fluid overload
- MR
- Chronic excessive after load
- AS
- Hypertension
- Hypertension
- AS
- Pump failure
- Causes
- Cardiac output is decreased and fails to
increase normally with exertion.
- High-output heart failure
- Systolic versus diastolic
failure
- Systolic failure
- Inability of the ventricle to
contract normally, resulting in
decreased cardiac output.
Ejection fraction is <40%.
- Causes
- IHD
- MI
- DCM
- myocarditis
- myocarditis
- DCM
- MI
- IHD
- Causes
- Inability of the ventricle to
contract normally, resulting in
decreased cardiac output.
Ejection fraction is <40%.
- Diastolic Failure
- Inability of the ventricle to
relax and fill normally
causing increased fillinf
pressures. Ejection fraction
> 50%.
- Causes
- Constrictive pericarditiS
- Tamponade
- Restrictive cardiomyopathy
- Hypertension
- Hypertension
- Restrictive cardiomyopathy
- Tamponade
- Constrictive pericarditiS
- Causes
- Inability of the ventricle to
relax and fill normally
causing increased fillinf
pressures. Ejection fraction
> 50%.
- Systolic failure
- Acute versus chronic heart
failure
- Acute heart failure
- Is often used exclusively to mean
new onset acute or
decompensation of chronic heart
failure characterised by
pulmonary and/or peripheral
edema with or without signs of
peripheral hypoperfusion.
- Is often used exclusively to mean
new onset acute or
decompensation of chronic heart
failure characterised by
pulmonary and/or peripheral
edema with or without signs of
peripheral hypoperfusion.
- Chronic Heart failure
- Develops or progresses
slowly, venous congestion
is common but arterial
pressure is well
maintained until very late.
- Develops or progresses
slowly, venous congestion
is common but arterial
pressure is well
maintained until very late.
- Acute heart failure
- Left-sided versus right-sided failure
- prognosis
- Poor with 25 - 50% of patients dying
within 5 years of diagnosis.
- Poor with 25 - 50% of patients dying
within 5 years of diagnosis.
- Diagnosis
- Routine laboratory Test
- biomarkers
- Echocardiography
- ECG
- Recommended test in all heart failure patients.
- CXR
- Cardiomegaly
- Dilated prominent
upper lobe vessels
- pleural
effusion
- Kerley B lines
- Alveolar Edema
- Bat wisngs
- Bat wisngs
- Interstitial edema
- Alveolar Edema
- Kerley B lines
- pleural
effusion
- Dilated prominent
upper lobe vessels
- Cardiomegaly
- ECG in CHF can show abnormalities as
arrhythmias, ischemia, MI, LVH, conduction
abnormalities such as PVCs, LBBB.
- Recommended test in all heart failure patients.
- ECG
- Echocardiography
- biomarkers
- Routine laboratory Test
- Symptoms
- Risk factors
- Tobacco use
- Hyperlipidemia
- Hypercholestremia
- Diabetes
- Diabetes
- Hypercholestremia
- Hyperlipidemia
- Tobacco use
- Management
- Non-pharmacological
- Limiting salt intake for all HF patients
- Limiting fluid intake for those with
hyponatremia, high diuretics intake
and severe HF
- Exercise for those with stable heart
and stable volume levels
- Monitoring all HF patients
- Monitoring all HF patients
- Exercise for those with stable heart
and stable volume levels
- Limiting fluid intake for those with
hyponatremia, high diuretics intake
and severe HF
- Limiting salt intake for all HF patients
- Pharmacological
- Drugs used
- Decreased load on the heart
- Diuretics
- ACE inhibitors
- ARBs
- Vasodilators
- Vasodilators
- ARBs
- ACE inhibitors
- Diuretics
- Increase the function of the heart
- Beta-blockers
- Adrenergics
- Inotropic-cardiotonic drugs
- Digoxin
- Phosphodiestrase inhibitors
- Dobutamine
- Adrenaline
- Adrenaline
- Dobutamine
- Phosphodiestrase inhibitors
- Digoxin
- Inotropic-cardiotonic drugs
- Adrenergics
- Beta-blockers
- Decreased load on the heart
- Drugs used
- Non-pharmacological
- Manifestations upon physical examinatio
- complications
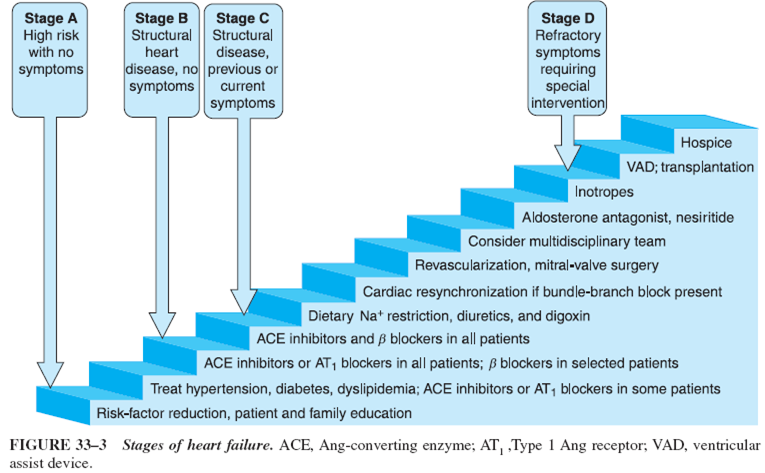
- Stages
- Cardiac cachexia
- Arrhythmia
- Kidney problems
- Anemia, stroke
- Leg venous stasis
- liver problems
- Hyponatremia
- Hyponatremia
- liver problems
- Leg venous stasis
- Anemia, stroke
- Kidney problems
- Arrhythmia
- Stages
- of
- RHF
- JVD
- Hepatosplenomegaly
- Pitting Edema
- Pitting Edema
- Hepatosplenomegaly
- JVD
- LVH
- Pulmonary congestion
- Decreased forward perfusion
- Cardiomegaly
- Tachycardia
- S3
- Ventricular Dilation
- Arrhythmia
- Arrhythmia
- Ventricular Dilation
- S3
- Tachycardia
- Cardiomegaly
- Decreased forward perfusion
- Pulmonary congestion
- RHF
- complications
- occurs when
- congestive heart failure
- presented with
- Orthopnea
- definition
- Difficulty in breathing that occurs when
lying down and is relieved upon
changing to an upright position.
- Causes
- LFH
- Bronchial Asthma
- Mitral stenosis
- MarkedAscites
- Anxiety &
hyperventilation
- Bilateral
diaphragmatic
paralysis
- pericardial diesease
- pericardial diesease
- Bilateral
diaphragmatic
paralysis
- Anxiety &
hyperventilation
- MarkedAscites
- Mitral stenosis
- Bronchial Asthma
- LFH
- Causes
- Difficulty in breathing that occurs when
lying down and is relieved upon
changing to an upright position.
- definition
- Oedema
- definition
- Is the accumelation of
excessive fluid in the
subcutaneous tissue.
- Causes
- Impairment of
lymphatic drainage
- Generalized
- Congenital
deiciency of
lymphatics
- Congenital
deiciency of
lymphatics
- Localized
- Local infection
- Trauma
- Burns
- Animal bites / stings
- Animal bites / stings
- Burns
- Trauma
- Local infection
- Generalized
- Increased plasma
hydrostatic pressure:
- Generalized
- CHF
- Vasodialatory
drugs
- Vasodialatory
drugs
- CHF
- Localized
- Venous
obstruction
- Venous
obstruction
- Generalized
- Decreased plasma
oncotic pressure
- Generalized
- Liver disease
- Renal disease
- Malnutrition/
malabsorption
- Malnutrition/
malabsorption
- Renal disease
- Liver disease
- localized
- Milroy's disease
- Lymphoedema
praecox
- Malignant
infiltration
- Malignant
infiltration
- Lymphoedema
praecox
- Milroy's disease
- Generalized
- Impairment of
lymphatic drainage
- Causes
- Is the accumelation of
excessive fluid in the
subcutaneous tissue.
- definition
- Dyspnea
- definiton
- Is the uncomfortable
awareness of breathing
- Causes
- sudden
- Pneumothorax, Pulmonary embolism,
Aspiration, Anaphylaxis , Anxiety,
Chest trauma
- Acute
- Asthma, Respiratory tract infection,
Lung tumors, Pleural effusion,
Metabolic acidosis
- Chronic
- COPD, Cardiac failure, Fibrosing
alveoli's, Anaemia, Arrhythmia, Vavular
heart disease, Chest wall deformities,
Pulmonary hypertension
- COPD, Cardiac failure, Fibrosing
alveoli's, Anaemia, Arrhythmia, Vavular
heart disease, Chest wall deformities,
Pulmonary hypertension
- Chronic
- Asthma, Respiratory tract infection,
Lung tumors, Pleural effusion,
Metabolic acidosis
- Acute
- Pneumothorax, Pulmonary embolism,
Aspiration, Anaphylaxis , Anxiety,
Chest trauma
- sudden
- Causes
- Is the uncomfortable
awareness of breathing
- definiton
- Fatigue
- definition
- A subjective symptom of malaise and aversion to
activity or to objectively impaired performance.
- A subjective symptom of malaise and aversion to
activity or to objectively impaired performance.
- definition
- Orthopnea
Media attachments
{kind=link}
Want to create your own Mind Maps for free with GoConqr? Learn more.