11048952
Description
Mind Map by SaraandEmily SnyderandBarnett, updated more than 1 year ago
|
|
Created by SaraandEmily SnyderandBarnett
about 8 years ago
|
|
Disseminated Intravascular Coagulation (DIC)
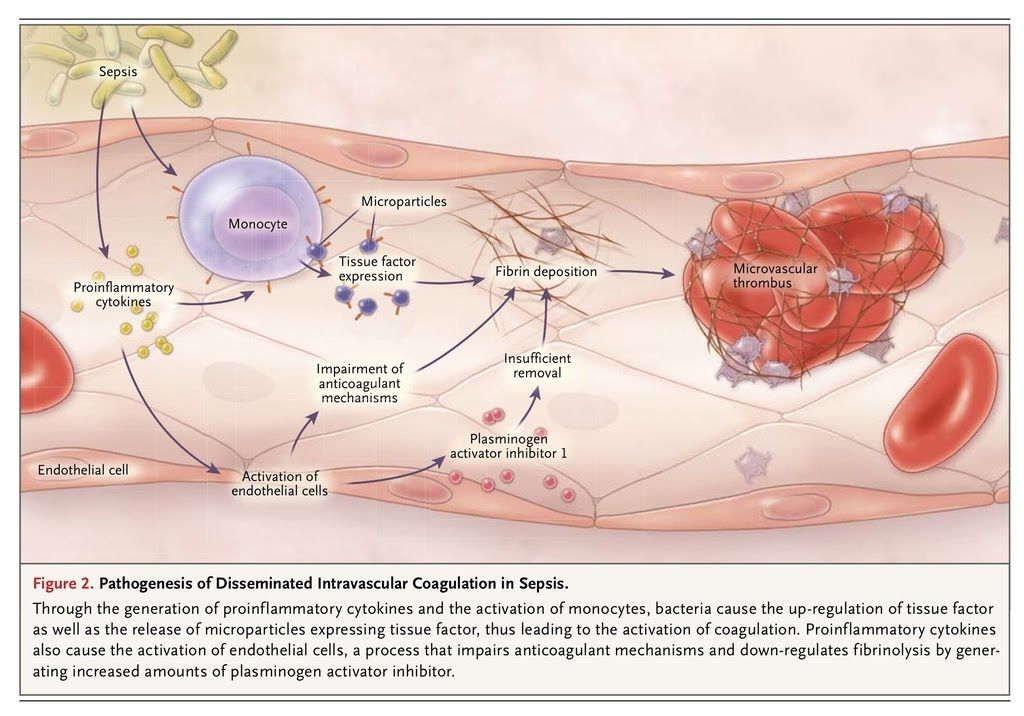
- Pathogenesis (Rome &
Lord, 2014; Stewart,
2001; Backhouse, 2004;
Kelly, 1998).
- A hematological disorder, NOT a disease: DIC
involves abnormal activation of the clotting
cascade secondary to a condition or disease
- Clinical Management and Treatment of DIC
(Frazier, 2012; Rome & Lord, 2014).
- Basic Treatment
- Vital Sign Monitoring
- Lab work monitoring,
especially anticoagulant
values
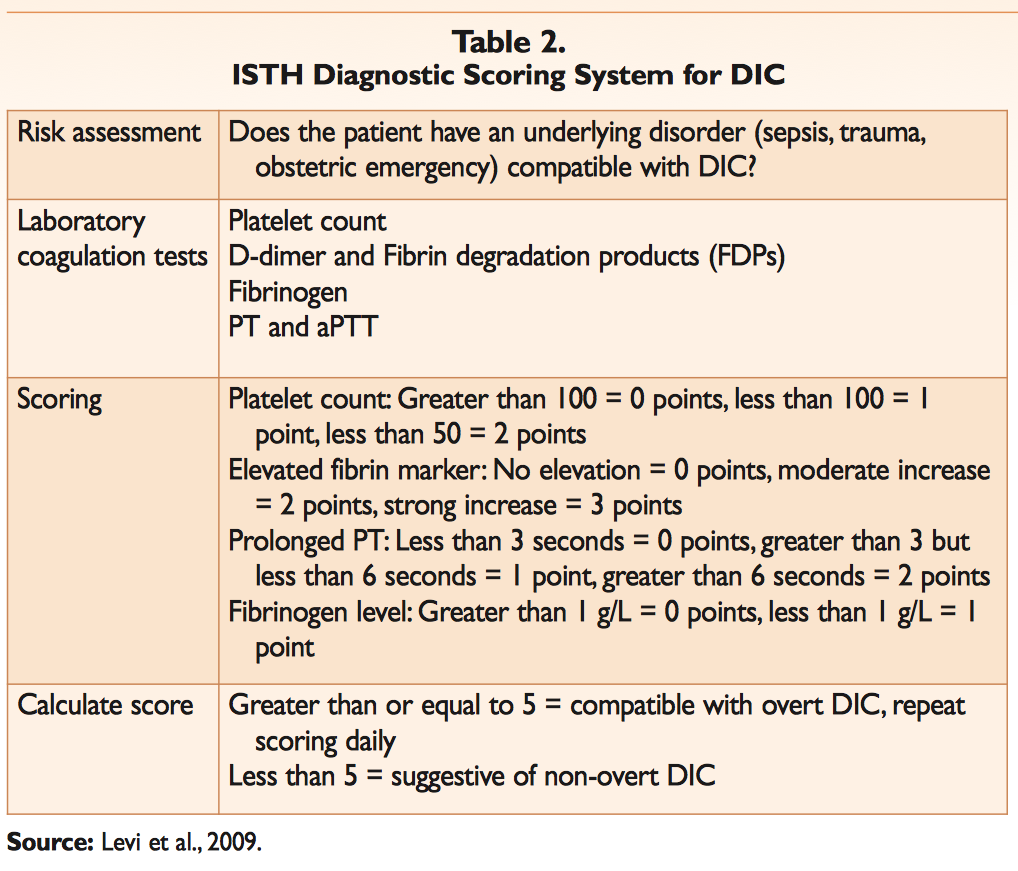
- Determine the patient specific risk factors,
and DIC score based on the International
Society for Thrombosis and Hemostasis
- Assess patient for the formation of
clots and evidence of bleeding
- If hypovolemia is
present, ensure
this is corrected
- Antibiotics to
treat sepsis
and infection
- Primary
Factor
Identification
- Vital Sign Monitoring
- Advanced Treatment
- Unfractionated
heparin
administration
(based on
patient's weight)
- Low molecular weight
heparin administration
(i.e. Lovenox/Enoxaparin)
- Administer fresh
frozen plasma
- If prolonged PT
or aPTT
- If prolonged PT
or aPTT
- Transfusion
of platelets
- For active
bleeding and
platelet count
below 50,000,
or before an
invasive
procedure
- For active
bleeding and
platelet count
below 50,000,
or before an
invasive
procedure
- Recombinant
activated
human
protein C
- Lysine
Analogues
- For severe
bleeding
- For severe
bleeding
- Primary disorder
treatment
- Unfractionated
heparin
administration
(based on
patient's weight)
- Basic Treatment
- Often a complication of septic shock and other
shock states
- DIC can also be a complication of:
Septecemia, transfusion reactions,
and obstetric complications
- DIC can also be a complication of:
Septecemia, transfusion reactions,
and obstetric complications
- Clinical Management and Treatment of DIC
(Frazier, 2012; Rome & Lord, 2014).
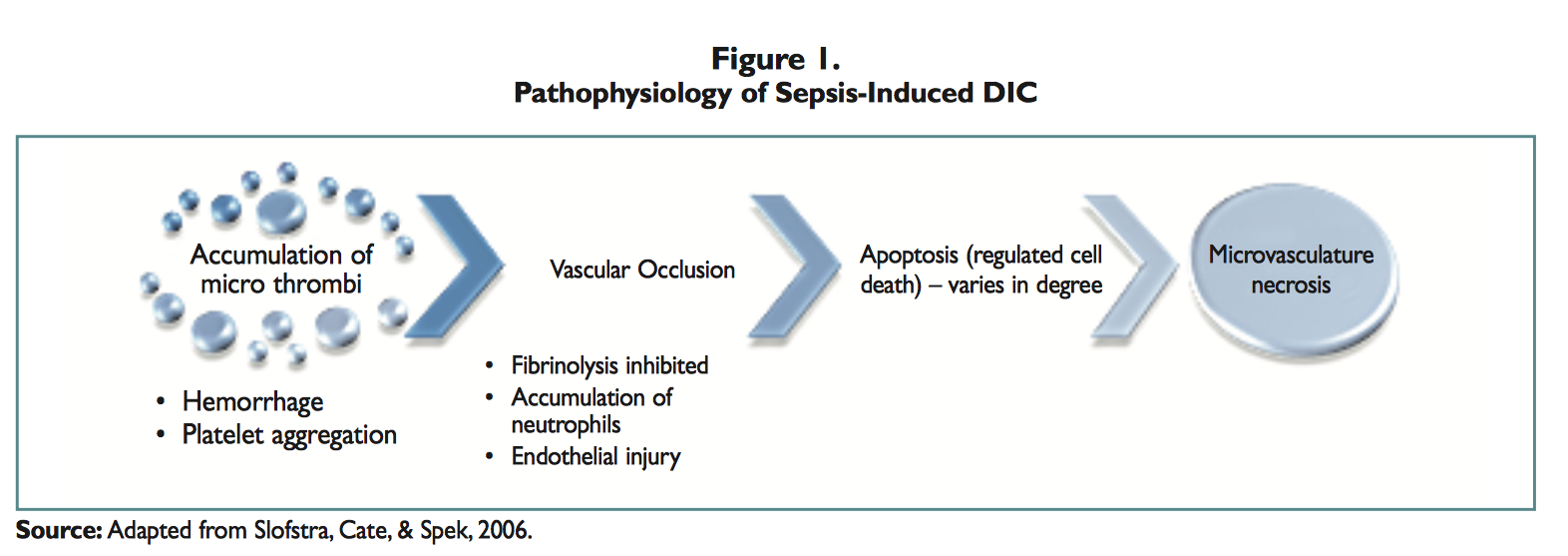
- Two major processes
involves in development of
DIC
- 1.) Activation of clotting cascade in
widespread circulation, as a result of
rapid buildup of Thrombin
- Increased
intravascular
Thrombin enhances
platelet aggregation
by speeding up the
conversion of
Fibrinogen to Fibrin
- Consequent thrombosis or clot
formation as a result of
accumulation of Fibrin and
platelets
- Presence of clots can lead
to reduced tissue perfusion
and subsequent anemia,
hypotension, organ
ischemia, and eventually
necrosis
- Presence of clots can lead
to reduced tissue perfusion
and subsequent anemia,
hypotension, organ
ischemia, and eventually
necrosis
- Consequent thrombosis or clot
formation as a result of
accumulation of Fibrin and
platelets
- Increased
intravascular
Thrombin enhances
platelet aggregation
by speeding up the
conversion of
Fibrinogen to Fibrin
- 2.) Hyperactive fibrinolysis due to
excessive clotting
- Fibrinolysis breaks down the new
clot and releases fibrin split
products [FSPs]
- FSPs have anticoagulant properties that inhibit normal
clotting
- Blood loses its ability to clot or to
clot effectively, this means there
will be no clot formation at sites of
injury and an increased risk for
hemorrhage
- Internal and External
hemorrhage due to
inappropriate
consumption of clotting
factors
- Internal and External
hemorrhage due to
inappropriate
consumption of clotting
factors
- Clinical Manifestations of DIC (Frazier, 2012;
Rome & Lord, 2014).
- Thrombotic Manifestations (from
deposition of fibrin or platelets in
microvasculature)
- Integumentary
- Cyanosis
- Tissue necrosis
from ischemia
- Hemorrhagic
necrosis
- Cyanosis
- Respiratory
- Tachypnea
- Dyspnea
- Acute respiratory
distress syndrome
- Pulmonary
embolism
- Tachypnea
- Cardiovascular
- ECG
changes
- Venous
distension
- ECG
changes
- Gastrointestinal
- Pain in abdomen
- Paralytic ileus
- Pain in abdomen
- Urinary
- Oliguria
- Renal failure
- Oliguria
- Integumentary
- Bleeding Manifestations (from platelet consumption
and depletion, coagulation factors, lysis of clots, an,
FSP formation with anticoagulant properties)
- Integumentary
- Pallor
- Petechiae
- Purpura
- Blood that
is oozing
- Bleeding at
venipuncture
sites
- Hemtomas
- Occult
hemorrhage
- Pallor
- Respiratory
- Orthopnea
- Hemoptysis
- Tachypnea
- Orthopnea
- Cardiovascular
- Tachycardia
- Hypotension
- Tachycardia
- Gastrointestinal (GI)
- Bleeding in
Upper GI
- Bleeding in
Lower GI
- Distended
Abdomen
- Blood in stool
- Bleeding in
Upper GI
- Urinary
- Hematuria
- Hematuria
- Neurological
- Changes in vision
- Dizziness
- Headache
- Mental status changes
- Irritability
- Changes in vision
- Musculoskeletal
- Bone
pain
- Joint
pain
- Bone
pain
- Integumentary
- Thrombotic Manifestations (from
deposition of fibrin or platelets in
microvasculature)
- Blood loses its ability to clot or to
clot effectively, this means there
will be no clot formation at sites of
injury and an increased risk for
hemorrhage
- FSPs have anticoagulant properties that inhibit normal
clotting
- Fibrinolysis breaks down the new
clot and releases fibrin split
products [FSPs]
- 1.) Activation of clotting cascade in
widespread circulation, as a result of
rapid buildup of Thrombin
- A hematological disorder, NOT a disease: DIC
involves abnormal activation of the clotting
cascade secondary to a condition or disease
- Nursing Management (Rome
& Lord, 2014; Stewart, 2001;
Kelly, 1998; Dressler, 1996;
Atassi & Harris, 2001;
Backhouse, 2004).
- Thorough history
- Bleeding disorders
- Medications that increase risk of
bleeding
- Bleeding disorders
- Intravenous Access
- Fluid replacement
- Ermergency infusion of
medications and blood
- Fluid replacement
- Skin Care and Hygiene
- Assess skin for signs
of bleeding such as
petichiae
- Frequent
repositioning
- To avoid ulcers and
skin breakdown
- To avoid blood stasis which could lead to further
thrombus formation
- To avoid ulcers and
skin breakdown
- Temperature every 4 hours and
use of soft swabs to bursh teeth
and electric razors for shaving to
reduce risk of hemorrhage
- Assess skin for signs
of bleeding such as
petichiae
- Cardiac Monitoring
- ECG monitoring for
dysrhythmias and ST
and T-wave changes
due to decreased
perfusion
- Vital signs every 15 minutes
- Systolic above 90 mmHg to ensure adequate
perfusion
- Systolic above 90 mmHg to ensure adequate
perfusion
- Peripheral pulses, capillary refill, skin temperature and color monitored every 2 hours
- To assess for adequate peripheral perfusion
- To assess for adequate peripheral perfusion
- ECG monitoring for
dysrhythmias and ST
and T-wave changes
due to decreased
perfusion
- Respiratory Monitoring
- Pulse oximetry
- Arterial blood gasses
- Respiratory rate, rhythm,
effort
- Assess for cyanosis and
shortness of breath
- Monitor for respiratory failure
caused by pulmonday hemorrhage,
hemothroax, or pulomanry embolus
- Supplemental Oxygen therapy
- Suctioning, deep
breaathing and coughing
- Supplemental Oxygen therapy
- Pulse oximetry
- Thorough history
- Collaborative Care of DIC (Stewart, 2001;
Rome & Lord, 2014; Kelly, 1998;
Backhouse, 2004).
- Physicians
- Diagnosing and treating underlying
condition causing DIC
- Diagnosing and treating underlying
condition causing DIC
- Nurses
- Administer
medications and
blood products as
ordered
- Comfort and pain
control
- Pressure bandages
on bleeding sites
- Assess for signs of active
bleeding or other
complication and intervene
accordingly
- Administer
medications and
blood products as
ordered
- Pharmacy
- Heparin or fresh frozen plasma
- Heparin or fresh frozen plasma
- Client and family
- Must be supported and
communication must be
continuous
- Can assist with history and care
- Can assist with history and care
- Must be supported and
communication must be
continuous
- Respiratory Therapists
- Management of ARDS and artificial ventilation
- Management of ARDS and artificial ventilation
- Specialists such as cardiology
- Physicians
- Classification (Frazier, 2012; Rome
& Lord, 2014).
- Non-Overt
- Condition where body is
able to compensate,
association with blood
dyscrasias
- Continuous or
intermittent
tissue factor
exposure
- Asymptomatic
- Only noticed
from lab values
- Dyscrasias
- Malignancies
- Anemia
- Leukemia
- Malignancies
- Continuous or
intermittent
tissue factor
exposure
- Condition where body is
able to compensate,
association with blood
dyscrasias
- Overt
- Condition with high rate of organ failure
and mortality due to body's inability to
compensate
- Sepsis
- Severe infections
- Hemolyisis
- Liver enzyme increase
- Platelet count decrease
- Liver failure
- Obstetric complications
- Bleeding that is obvious
- Symptomatic patient
- Sepsis
- Condition with high rate of organ failure
and mortality due to body's inability to
compensate
- Non-Overt
- Client-Centered Care (Registered
Nurses Association of Ontario,
2015).
- Therapeutic Communication
- Respect
- Human Dignity
- Timeliness
- Clients are leaders of
their own care
- Goal directed care
- Clients are experts on their
own lives
- Continuity and consistency
of care and caregiver
- Core Processes
- Identify concerns/needs
- Making decisions
- Caring and service
- Evaluating outcomes
- Identify concerns/needs
- Therapeutic Communication
Media attachments
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Mind Maps for free with GoConqr? Learn more.