12799926
Description
Mind Map by kim bodick, updated more than 1 year ago
|
|
Created by kim bodick
almost 7 years ago
|
|
Heart Failure 101
- Heart Failure
Classifications
- The heart is a four
chambered, 2-sided pump.
Heart failure can happen as
a result of damage or
weakening of heart muscle
or valves (Heart and Stroke
Foundation of Canada, 2018)
- Abnormalitites in heart function can
cause blood to back up in peripheral
circulation causing edema. Failure or
inadequate pumping can also cause
congestion in lungs manifesting as
pulmonary edema. Inadequate pumping
of the heart also leads to perfusion and
oxygenation difficulties (Heart and
Stroke Foundation of Canada, 2018)
- New York Heart Association
Functional Classification of
People with Cardiac Disease
(NYHA, 2018)
- Class I: No limitation of physical activity. Ordinary physical
activity does not cause undue fatigue, dyspnea,
palpitations, or anginal pain.
- Class II: Slight limitations of physical activity. No
symptoms at rest. Ordinary physical activity results in
fatigue, palpitations, dyspnea, or anginal pain
- Class III: Marked limitation of physical activity. Usually
comfortable at rest. Ordinary physical activity causes
fatigue, dyspnea, palpitations, or anginal pain
- Class IV: Unable to carry on any physical activity
without discomfort. Symptoms of heart failure at
rest. If any physical activity is undertaken
discomfort increases.
- Class I: No limitation of physical activity. Ordinary physical
activity does not cause undue fatigue, dyspnea,
palpitations, or anginal pain.
- New York Heart Association
Functional Classification of
People with Cardiac Disease
(NYHA, 2018)
- Abnormalitites in heart function can
cause blood to back up in peripheral
circulation causing edema. Failure or
inadequate pumping can also cause
congestion in lungs manifesting as
pulmonary edema. Inadequate pumping
of the heart also leads to perfusion and
oxygenation difficulties (Heart and
Stroke Foundation of Canada, 2018)
- The heart is a four
chambered, 2-sided pump.
Heart failure can happen as
a result of damage or
weakening of heart muscle
or valves (Heart and Stroke
Foundation of Canada, 2018)
- Main Causes (Heart and Stroke
Foundation of Canada, 2018).
- Hypertension
Annotations:
- Hypertension and ethnicity: In Canada people who are Black or of South Asian descent are three times more likely to develop HTN than White individuals or East Asian Canadians. Black Canadians have a higher mortality rate related to HTN than White individuals. Female Black Canadians have a disproportionately high prevalence of HTN.HTN is more prevalent among First Nations adults than the general population and HTN is more aggressive in Black and Aboriginal populations and results in more severe end-organ damage (Lewis, 2014, pg. 867).
- High pressures within vessels cause
damage and scarring to vessels and valves
- Damaged vessels lose
elasticity, scar and narrow
forcing the heart muscle to
pump harder through narrow
openings
- The heart compensates by
getting larger
(cardiomegaly), to pump
more blood, but efficiency
begins to decline (American
Heart Association, 2018).
- The heart compensates by
getting larger
(cardiomegaly), to pump
more blood, but efficiency
begins to decline (American
Heart Association, 2018).
- Damaged vessels lose
elasticity, scar and narrow
forcing the heart muscle to
pump harder through narrow
openings
- Diabetes
Annotations:
- People diagnosed with Diabetes (Type I and Type II) are at very high risk of heart disease and stroke (Canadian Diabetes Association, 2018). People with Diabetes may develop heart disease 10 to 15 years earlier than individuals without diabetes (Canadian Diabetes Association, 2018). High blood glucose (sugar) is one risk factor for heart attack or stroke, but people with diabetes often have a number of other risk factors. These include being overweight (especially if they have excess fat around the waist), inactive lifestyles, high blood pressure and high cholesterol. People who smoke or have a family history of heart disease or stroke are at even higher risk (Canadian Diabetes Association, 2018).
- Individuals who have been diagnosed with
diabetes, tend to develop hypertension and
atherosclerosis from elevated lipid levels,
both of which are closely linked to heart
disease (American Heart Association, 2018).
- Atherosclerosis and
hypertension increase the risk
for CVD, PVD, and stroke
- Causing damage or
weakness to heart
muscle
- Causing damage or
weakness to heart
muscle
- Atherosclerosis and
hypertension increase the risk
for CVD, PVD, and stroke
- Coronary
Artery
Disease
- CAD is a disease process that involves the blood vessels
of the heart itself. It affects the arteries supplying blood
to the heart muscle and is associated with serious
conditions including myocardial infarction,
stable/unstable angina, and reduced oxygen and
nutrient flow to tissues (Lewis, 2014).
- CAD is caused by atherosclerosis, which causes narrowing
and blockages of coronary arteries and by cardiac disease
processes. This condition is exacerbated by a poor diet,
sedentary lifestyle, smoking, high cholesterol,
long-standing hypertension, drug and alcohol abuse and
increased body weight particularly of the abdominal girdle
(Heart and Stroke Foundation of Canada, 2018).
- CAD is caused by atherosclerosis, which causes narrowing
and blockages of coronary arteries and by cardiac disease
processes. This condition is exacerbated by a poor diet,
sedentary lifestyle, smoking, high cholesterol,
long-standing hypertension, drug and alcohol abuse and
increased body weight particularly of the abdominal girdle
(Heart and Stroke Foundation of Canada, 2018).
- CAD is a disease process that involves the blood vessels
of the heart itself. It affects the arteries supplying blood
to the heart muscle and is associated with serious
conditions including myocardial infarction,
stable/unstable angina, and reduced oxygen and
nutrient flow to tissues (Lewis, 2014).
- Other Causes:
(Heart and
Stroke
Foundation of
Canada, 2018)
- Alcohol and
Drug Abuse
- Heavy binge drinking is associated with increased
risk for hypertension. It can also be problematic
when interacting with medications (Heart & Stroke,
2018). Drugs such as amphetamines, cannabis
(marihuana), cocaine, ecstasy, heroin, opiates, LSD
and PCP all increase your risk of having a stroke or
developing heart disease (Heart & Stroke, 2018).
- Heavy binge drinking is associated with increased
risk for hypertension. It can also be problematic
when interacting with medications (Heart & Stroke,
2018). Drugs such as amphetamines, cannabis
(marihuana), cocaine, ecstasy, heroin, opiates, LSD
and PCP all increase your risk of having a stroke or
developing heart disease (Heart & Stroke, 2018).
- Unhealthy Body Weight
- Increased
triglyceride
(LDL) levels
- Increased risk
of Type II
Diabetes
- Hypertension
- Sleep Apnea
- Increased
risk of MI
- Increased
risk of
CAD
- Body Mass Index
(Canadian Diabetes
Association, 2018;
American Heart
Association, 2018;
Heart and Stroke
Foundation of
Canada, 2018)
Annotations:
- Printable BMI Chart. (n.d.). [JPEG] Retrieved from https://www.vertex42.com/ExcelTemplates/bmi-chart.html
- Normal:
18.5 -24.5
- Overweight:
25-29.9
- Obese:
30 +
- Increased
triglyceride
(LDL) levels
- Valvular disorders and
cardiomyopathy
- Conditions of heart valves that involve
stenosis (narrowing) of the great vessels or
regurgitation of blood back ward into atria
or peripheral circulation. Cardiomyopathy
refers to a group of disease that directly
affect the structural or functional ability of
the myocardium. May be primary
(idiopathic) or secondary (attributed to
another disease process) (Lewis, 2014).
- Conditions of heart valves that involve
stenosis (narrowing) of the great vessels or
regurgitation of blood back ward into atria
or peripheral circulation. Cardiomyopathy
refers to a group of disease that directly
affect the structural or functional ability of
the myocardium. May be primary
(idiopathic) or secondary (attributed to
another disease process) (Lewis, 2014).
- High Cholesterol
- LDL (low density lipoprotein) and HDL (high density
lipoprotein) levels can be checked with a simple blood
test. Adults 20 years of age and older should have their
cholesterol and other cardiac risk factors checked every
four to six years (American Heart Association, 2018).
- LDL (low density lipoprotein) and HDL (high density
lipoprotein) levels can be checked with a simple blood
test. Adults 20 years of age and older should have their
cholesterol and other cardiac risk factors checked every
four to six years (American Heart Association, 2018).
- Infections: Specifically,
infections involving
inflammation of the heart
muscle or lining of the heart.
Individuals with pre-existing
heart valve abnormalities or
heart conditions are at
particularly increased risk.
- Oral Health and Periodontal
Disease. Several studies by
the Canadian Dental Health
Association (Lavigne, 2004)
and in The Journal of Dental
Hygiene (Mosely et al., 2014;
Jones, 2015) have shown a
link between poor oral
health and periodontal
disease, and poor
cardiovascular health. Some
acute infections in
individuals with heart
conditions or weakened
heart valves may develop
more severe complications
- Myocarditis
- A condition of focal or diffuse
inflammation of the myocardium. Most
commonly caused by viral infections,
parasites, fungi, radiation therapy,
chemical or pharmacological
interventions and autoimmune
diseases. Myocarditis is frequently
associated with acute pericarditis.
- A condition of focal or diffuse
inflammation of the myocardium. Most
commonly caused by viral infections,
parasites, fungi, radiation therapy,
chemical or pharmacological
interventions and autoimmune
diseases. Myocarditis is frequently
associated with acute pericarditis.
- Bacterial
endocarditis
- Caused by bacteria circulating within the blood
stream. Bacterial colonies reach heart muscle and
valves and manifest inflammation and infection
processes. Endocarditis is uncommon in healthy
hearts.
Annotations:
- University of Cambridge. (2018). This Vibrant Bacteria Could Be Used to “Grow” Paint. [JPEG] Accessed on 16 March 2018. Retrieved from https://www.smithsonianmag.com/tag/bacteria/
- Caused by bacteria circulating within the blood
stream. Bacterial colonies reach heart muscle and
valves and manifest inflammation and infection
processes. Endocarditis is uncommon in healthy
hearts.
- Myocarditis
- Oral Health and Periodontal
Disease. Several studies by
the Canadian Dental Health
Association (Lavigne, 2004)
and in The Journal of Dental
Hygiene (Mosely et al., 2014;
Jones, 2015) have shown a
link between poor oral
health and periodontal
disease, and poor
cardiovascular health. Some
acute infections in
individuals with heart
conditions or weakened
heart valves may develop
more severe complications
- Hypervolemia
- An important reason that nurses must meticulously evaluate
clients who are receiving IV therapy and fluid through
peripherally or centrally inserted lines. Fluid overload can lead
to pulmonary congestion, fluid and electrolyte imbalances,
hypertension, edema, shortness of breath and death. Clients
in heart failure can very easily be overloaded - exacerbating
the condition significantly (Lewis, 2014).
- An important reason that nurses must meticulously evaluate
clients who are receiving IV therapy and fluid through
peripherally or centrally inserted lines. Fluid overload can lead
to pulmonary congestion, fluid and electrolyte imbalances,
hypertension, edema, shortness of breath and death. Clients
in heart failure can very easily be overloaded - exacerbating
the condition significantly (Lewis, 2014).
- Alcohol and
Drug Abuse
- Hypertension
- Manifestations
(Lewis, 2014)
- Symptoms
- Right-Sided Symptoms
- Fatigue
- Dependent Edema
- Upper Right
Quadrant Pain
- Anorexia and
GI Bloating
- Nausea
- Fatigue
- Left-Sided Symptoms
- Fatigue
- Dyspnea
- Orthopnea
- Dry Hacking Cough
- Pulmonary Edema
- Nocturia
- Paroxysmal Nocturnal
Dyspnea
- Fatigue
- Right-Sided Symptoms
- Signs
- Signs of
Left-Sided
Failure
- Left Ventricular Heaves
- Cheyne-Stokes
Respiration
- Patients with respiratory pattern
disturbances or altered
respiratory function and
impairment of gas exchange must
be monitored for fluctuations in
blood pH Normal: 7.35 - 7.45
- pCO2 = 34 - 45 mmHg (Lewis, 2014)
- pO2 = 80 - 100 mmHg (Lewis, 2014)
- HCO3 = 22 - 26 mEq/L (Lewis, 2014)
- pCO2 = 34 - 45 mmHg (Lewis, 2014)
- Patients with respiratory pattern
disturbances or altered
respiratory function and
impairment of gas exchange must
be monitored for fluctuations in
blood pH Normal: 7.35 - 7.45
- Pulsus Alternans
- Increased Heart Rate
- Crackles (pulmonary edema)
- S3 S4 Auscultation
- The most common form of initial
heart failure experienced is left-sided
failure. Left-sided failure is caused by
left-sided dysfunction (back-up of
blood), increased pressure on the
pump and great vessels causes
increased pressure and extravasation
of fluid in vessels - which manifests
as pulmonary congestion and edema
(Lewis, 2014).
- Left Ventricular Heaves
- Signs of
Right-Sided
Failure
- Right Ventricular
Heaves
- Murmurs
- Peripheral
Edema (Lewis, 2014)
- 1+ Slight pitting, no visible
change in shape of the
extremity; depth of indentation
<6mm; disappears rapidly
- 2+ No marked change in
shape of the extremity;
depth indentation 6-12mm;
disappears 10-15 sec
- 3+ Noticeably deep pitting; swollen
extremities; depth of pitting 1
-2.5cm; duration 1-2 minutes
- 4+ Very swollen; distorted
extremity; depth of pitting >2.5
cm; duration 2-5 minutes
- 1+ Slight pitting, no visible
change in shape of the
extremity; depth of indentation
<6mm; disappears rapidly
- Weight Gain
- Patients must be weighed
daily, in conjunction with a
closely monitored fluid
intake restriction (1.5 - 2.0 L
per day Lewis, 2014).
- Sudden weight gain
of 2kg in 2 days is
often indicative of
exacerbated heart
failure (Lewis, 2014)
- Sudden weight gain
of 2kg in 2 days is
often indicative of
exacerbated heart
failure (Lewis, 2014)
- Patients must be weighed
daily, in conjunction with a
closely monitored fluid
intake restriction (1.5 - 2.0 L
per day Lewis, 2014).
- Increased Heart Rate
- Ascites
- Jugular Vein Distention
- Hepatomegaly
- Causes: Right-sided failure causes backup of
blood into the right atrium and into venous
circulation. This manifests as peripheral
edema in dependent areas of the body (feet,
ankles, wrists). The primary cause of
right-sided failure is left-sided failure. In this
case left-sided failure results in pulmonary
congestion and increased pressure on blood
vessels of the lung (pulmonary
hypertension). Cor pulmonale results (right
ventricular dilation and hypertrophy caused
by pulmonary pathology) as a result of
right-sided failure (Lewis, 2014).
- Right Ventricular
Heaves
- Signs of
Left-Sided
Failure
- Symptoms
- Diagnostic Testing
(Heart and Stroke
Foundation of
Canada, 2018)
- Chest X-Ray
- A radiographic
picture of the
heart, lungs and
bones of the
chest
- Used to diagnose a large or
unusually shaped heart.
Used to diagnose the
presence of valvular
dysfunction and evaluate
how serious the condition
may be (Heart and Stroke
Foundation, 2018). Can also
be useful in the differential
diagnosis of pericarditis
and endocarditis
- Used to diagnose a large or
unusually shaped heart.
Used to diagnose the
presence of valvular
dysfunction and evaluate
how serious the condition
may be (Heart and Stroke
Foundation, 2018). Can also
be useful in the differential
diagnosis of pericarditis
and endocarditis
- A radiographic
picture of the
heart, lungs and
bones of the
chest
- Echocardiogram
- An echocardiogram uses sound
waves to create a picture of the
heart. It is the most widely used
test to determine a heart's ejection
fraction. (Normal: 50-70%)
- This diagnostic test is used to observe the valvular
movement and swell as the shape and texture of the heart
changes as it beats. It also looks at the heart chambers and
the degree of mechanical heart function. Useful for
diagnosing heart murmurs, myocardial infarction and
infection of the heart. Echoes can be used to evaluate
ejection fraction of the ventricles (Heart and Stroke
Foundation, 2018; Lewis, 2014; Jiayun et al, 2015).
- Heart Failure with
Preserved Ejection
Fraction (formerly
called DIASTOLIC
Heart Failure)
- Heart muscle
contracts normally
but the ventricles
do not relax as
they should during
ventricular filling
(American Heart
Associaton, 2018)
- Heart muscle
contracts normally
but the ventricles
do not relax as
they should during
ventricular filling
(American Heart
Associaton, 2018)
- Heart Failure with
Reduced Ejection
Fraction (formerly
called SYSTOLIC
Heart Failure)
- The heart muscle
does not contract
effectively and less
oxygen rich blood is
pumped out to the
rest of the body
(American Heart
Association, 2018)
- The heart muscle
does not contract
effectively and less
oxygen rich blood is
pumped out to the
rest of the body
(American Heart
Association, 2018)
- Heart Failure with
Preserved Ejection
Fraction (formerly
called DIASTOLIC
Heart Failure)
- This diagnostic test is used to observe the valvular
movement and swell as the shape and texture of the heart
changes as it beats. It also looks at the heart chambers and
the degree of mechanical heart function. Useful for
diagnosing heart murmurs, myocardial infarction and
infection of the heart. Echoes can be used to evaluate
ejection fraction of the ventricles (Heart and Stroke
Foundation, 2018; Lewis, 2014; Jiayun et al, 2015).
- An echocardiogram uses sound
waves to create a picture of the
heart. It is the most widely used
test to determine a heart's ejection
fraction. (Normal: 50-70%)
- Electrocardiogram
(ECG 12 Lead)
- A tool to measure
the electrical
activity of the
heart.
- Useful in detecting abnormal
electrical conduction in the
hearts conduction system. this
includes past, recent or ongoing
heart attacks. All of which can
result in heart muscle damage,
coronary artery blockage,
enlarged heart muscle, and
inflammation of the pericardial
sac. Can detect electrical
disturbances and pathology due
to lung diseases (Heart and
Stroke Foundation, 2018).
- STEMI
- ST-Elevation
Myocardial
Infarction.
Identified when
the ST segment
of the cardiac
cycle is elevated
by 2 mm or
more above the
isoelectric line,
in two or more
anatomically
contiguous leads
- STEMIs indicate
necrosis of cardiac
muscle. Reversal of
necrosis is not likely,
but some hypoxic
tissue damage may still
be salvaged and some
ischemia reversed.
- STEMIs cause damage to the heart muscle itself and
can lead to future heart failure or dysfunction.
Recognizing the signs and symptoms of MI and
making the appropriate interventions are vital to
preserve heart tissue during an attack
- Serum cardiac
markers are
measured if a
patient is
suspected of
having an MI.
Cardiac-specific
troponin T (cTnT)
and cardiac
specific troponin
I (cTnI) are highly
specific
indicators of
myocardial
injury
- STEMIs cause damage to the heart muscle itself and
can lead to future heart failure or dysfunction.
Recognizing the signs and symptoms of MI and
making the appropriate interventions are vital to
preserve heart tissue during an attack
- STEMIs indicate
necrosis of cardiac
muscle. Reversal of
necrosis is not likely,
but some hypoxic
tissue damage may still
be salvaged and some
ischemia reversed.
- ST-Elevation
Myocardial
Infarction.
Identified when
the ST segment
of the cardiac
cycle is elevated
by 2 mm or
more above the
isoelectric line,
in two or more
anatomically
contiguous leads
- N-STEMI
- Non- ST
Elevation
Myocardial
Infarction
- NSTEMIs indicate
hypoxia of cardiac
tissues (ischemia)
that may be
reversible. Necrosis
is not readily
apparent but a
myocardial
infarction is still
occurring and may
lead to necrosis if
no interventions are
made.
- NSTEMIs indicate
hypoxia of cardiac
tissues (ischemia)
that may be
reversible. Necrosis
is not readily
apparent but a
myocardial
infarction is still
occurring and may
lead to necrosis if
no interventions are
made.
- Non- ST
Elevation
Myocardial
Infarction
- STEMI
- Useful in detecting abnormal
electrical conduction in the
hearts conduction system. this
includes past, recent or ongoing
heart attacks. All of which can
result in heart muscle damage,
coronary artery blockage,
enlarged heart muscle, and
inflammation of the pericardial
sac. Can detect electrical
disturbances and pathology due
to lung diseases (Heart and
Stroke Foundation, 2018).
- A tool to measure
the electrical
activity of the
heart.
- Brain
Natriuretic
Peptide Test
- A blood test measuring
levels of Brain Natriuretic
Peptide - a hormone
produced by the
myocytes of the heart
when the ventricles of
the heart stretch too far
too often.
- This blood test is used to
determine the levels of brain
natriuretic peptide (BNP)
and if abnormally high levels
are present it indicate heart
failure. Usually used to
determine heart failure also
used when patients are
having trouble breathing or
have edema in the arms or
legs (Heart and Stroke
Foundation, 2018; Lewis,
2014).
- This blood test is used to
determine the levels of brain
natriuretic peptide (BNP)
and if abnormally high levels
are present it indicate heart
failure. Usually used to
determine heart failure also
used when patients are
having trouble breathing or
have edema in the arms or
legs (Heart and Stroke
Foundation, 2018; Lewis,
2014).
- A blood test measuring
levels of Brain Natriuretic
Peptide - a hormone
produced by the
myocytes of the heart
when the ventricles of
the heart stretch too far
too often.
- Coronary
Angiogram
- A radiographic image
of the coronary
vessels feeding the
heart muscle.
Achieved with the
use of radiolucent
dye.
- Used to determine if
coronary arteries feeding
the heart muscle are
partially or completely
obstructed. Treatment
may include angioplasty,
coronary artery bypass
surgery, medical therapy
or lifestyle changes (Heart
and Stroke Foundation,
2018).
- Angioplasty is a procedure
wherein a catheter is inserted
through the wrist or groin
into the heart. The catheter is
used to inflate a balloon, to
relieve obstruction of the
coronary arteries.
- Angioplasty is a procedure
wherein a catheter is inserted
through the wrist or groin
into the heart. The catheter is
used to inflate a balloon, to
relieve obstruction of the
coronary arteries.
- Used to determine if
coronary arteries feeding
the heart muscle are
partially or completely
obstructed. Treatment
may include angioplasty,
coronary artery bypass
surgery, medical therapy
or lifestyle changes (Heart
and Stroke Foundation,
2018).
- A radiographic image
of the coronary
vessels feeding the
heart muscle.
Achieved with the
use of radiolucent
dye.
- Exercise
Cardiogram
(Stress Test)
- An exercise ECG is used to
record the heart response to
electrical impulses. This is done
by recording the heart's
electrical impulses, blood
pressure, and heart rate while
the patient is exercising.
- Used for unexplained chest
pain and or if coronary
artery disease is suspected.
It is also used to determine
the seriousness of coronary
artery disease if diagnosed.
Used to determine how
much exercise a person can
endure after an MI or
surgery. Also recommended
for people with arrhythmias,
tachycardia, and
bradycardia, palpitations and
dizziness or fatigue (Heart
and Stroke Foundation,
2018).
- Used for unexplained chest
pain and or if coronary
artery disease is suspected.
It is also used to determine
the seriousness of coronary
artery disease if diagnosed.
Used to determine how
much exercise a person can
endure after an MI or
surgery. Also recommended
for people with arrhythmias,
tachycardia, and
bradycardia, palpitations and
dizziness or fatigue (Heart
and Stroke Foundation,
2018).
- An exercise ECG is used to
record the heart response to
electrical impulses. This is done
by recording the heart's
electrical impulses, blood
pressure, and heart rate while
the patient is exercising.
- Chest X-Ray
- Treatment and Management
- Medications
- Beta Blockers
- Beta-blockers function to counteract the
negative effects of the failing heart such as
increased HR. Beta-blockers decrease
myocardial contractility, and decrease the
work of the heart an in effect can lower
blood pressure.
- Always assess patient's blood pressure before providing a
medication that affects pressure. Normal reading for
healthy adults is 120/80 mmHg. Some patients may have
readings outside of the norm, in which case use the baseline
to determine whether a pressure reading is normal for a
patient. Assess whether the patient is symptomatic if
readings are outside of norms.
- Example:
Metoprolol
- Example:
Metoprolol
- Always assess patient's blood pressure before providing a
medication that affects pressure. Normal reading for
healthy adults is 120/80 mmHg. Some patients may have
readings outside of the norm, in which case use the baseline
to determine whether a pressure reading is normal for a
patient. Assess whether the patient is symptomatic if
readings are outside of norms.
- Beta-blockers function to counteract the
negative effects of the failing heart such as
increased HR. Beta-blockers decrease
myocardial contractility, and decrease the
work of the heart an in effect can lower
blood pressure.
- ACE Inhibitors
- Useful in the treatment of systolic and diastolic HF.
Considered to be first-line therapy for HF. Inhibiting
conversion of Angiotensin I to Angiotensin II
prevents vasoconstrictive effects of the
renin-angiotensin-aldosterone system. (Lewis, 2014).
- Evaluate baseline and
current blood pressure
before administering.
- Example:
Enalapril
- Example:
Enalapril
- Evaluate baseline and
current blood pressure
before administering.
- Useful in the treatment of systolic and diastolic HF.
Considered to be first-line therapy for HF. Inhibiting
conversion of Angiotensin I to Angiotensin II
prevents vasoconstrictive effects of the
renin-angiotensin-aldosterone system. (Lewis, 2014).
- Cardiac Glycosides
- Function as positive inotropes and
decrease the conduction speed within the
myocardium, slowing the heart rate and
decreasing the work of the heart. These
actions lead to improved contractility and
ventricular emptying because of
improved stroke volume (Lewis, 2014).
- Very narrow therapeutic range. >2ng/ml = toxic
range. Blood work must be monitored closely.
K+ levels must be within normal range,
hypokalemia can result in digitalis toxicity.
Patients APICAL pulse rate must be assessed
before administration (must be >60 beats per
minute unless otherwise ordered by a physician)
- Example:
Lanoxin
- ANTIDOTE:
DIGIBIND
- ANTIDOTE:
DIGIBIND
- Example:
Lanoxin
- Very narrow therapeutic range. >2ng/ml = toxic
range. Blood work must be monitored closely.
K+ levels must be within normal range,
hypokalemia can result in digitalis toxicity.
Patients APICAL pulse rate must be assessed
before administration (must be >60 beats per
minute unless otherwise ordered by a physician)
- Function as positive inotropes and
decrease the conduction speed within the
myocardium, slowing the heart rate and
decreasing the work of the heart. These
actions lead to improved contractility and
ventricular emptying because of
improved stroke volume (Lewis, 2014).
- Angiotensin
Receptor Blocker
- Prevent the conversion of Angiotensin II, produces
vasodilation and increases salt and water excretion
(Lewis, 2014), effectively lowering blood pressure and
workload on the heart muscle.
- Example:
Losartan
- Example:
Losartan
- Prevent the conversion of Angiotensin II, produces
vasodilation and increases salt and water excretion
(Lewis, 2014), effectively lowering blood pressure and
workload on the heart muscle.
- Diuretics
Annotations:
- IMPORTANT!! Check patient's K+ levels and monitor closely during diuretic therapy Normal K+ (3.5 - 5.0 mmol) Normal NA (135 - 145 mEq) Normal Cl (96 - 106 mEq)
- Loop
(Non-Potassium
sparing)
- Inhibits NaCl reabsorption in the Loop of Henle.
Increases the excretion of Na+ and Cl-. More
potent diuretic, but has a shorter duration.
Excretes K+ ions. Potassium levels must be closely
monitored (Lewis, 2014). K+ level norm:3.5.5.0
- Patients who are experiencing heart failure, and who
also receive digitalis may be at risk for hypokalemia.
Patients are at risk for digitalis toxicity. Always
review blood work and evaluate heart rate and blood
pressure before administering this drug.
- Example:
Furosemide
- Example:
Furosemide
- Patients who are experiencing heart failure, and who
also receive digitalis may be at risk for hypokalemia.
Patients are at risk for digitalis toxicity. Always
review blood work and evaluate heart rate and blood
pressure before administering this drug.
- Inhibits NaCl reabsorption in the Loop of Henle.
Increases the excretion of Na+ and Cl-. More
potent diuretic, but has a shorter duration.
Excretes K+ ions. Potassium levels must be closely
monitored (Lewis, 2014). K+ level norm:3.5.5.0
- Potassium
Sparing
- Inhibit the Na+ retaining
and K+ excreting effects
of aldosterone in distal
collecting tubules of the
kidneys (Lewis, 2014).
- Patient's blood work must be closely monitored for
hyperkalemia. Hyperkalemia can result in nausea
and vomiting, abdominal cramping, headaches,
cardiac dysrhythmias and cardiac arrest. Potassium
sparing diuretics do not allow for the elimination of
potassium during the filtration process by the
kidneys. Hyperkalemia >5.2 mmol (Lewis, 2014) can
cause severe cardiac side effects.
- Example:
Spironolactone
- Example:
Spironolactone
- Patient's blood work must be closely monitored for
hyperkalemia. Hyperkalemia can result in nausea
and vomiting, abdominal cramping, headaches,
cardiac dysrhythmias and cardiac arrest. Potassium
sparing diuretics do not allow for the elimination of
potassium during the filtration process by the
kidneys. Hyperkalemia >5.2 mmol (Lewis, 2014) can
cause severe cardiac side effects.
- Inhibit the Na+ retaining
and K+ excreting effects
of aldosterone in distal
collecting tubules of the
kidneys (Lewis, 2014).
- Nitrates
- Work to dilate and
expand coronary
vessels and
decrease preload
primarily and
afterload (Lewis,
2014).
- Example:
Nitroglycerine
- Example:
Nitroglycerine
- Work to dilate and
expand coronary
vessels and
decrease preload
primarily and
afterload (Lewis,
2014).
- Antidysrhythmics
- Several major classes.
Function to alter
conduction velocity, and
decrease impulse
conduction, reduce
contractility, and
automaticity of pace
maker cells and/or the
myocardium (Lewis,
2014).
- Inotropic
- Modifies the
contraction of the
heart muscle
- Positive:
Strengthen
the force of
the heart's
contraction
- Example:
Digitalis
- Example:
Digitalis
- Negative:
Lessen the
strength of
the hearts
contraction
- Example:
Metoprolol
- Example:
Metoprolol
- Positive:
Strengthen
the force of
the heart's
contraction
- Modifies the
contraction of the
heart muscle
- Dromotropic
- Modifies
conduction
speed of the
heart's
conduction
system
- Positive:
Increases
conduction
speed
- Example:
Phenytoin
- Example:
Phenytoin
- Negative:
Decreases
conduction
speed
- Example:
Verapamil
- Example:
Verapamil
- Positive:
Increases
conduction
speed
- Modifies
conduction
speed of the
heart's
conduction
system
- Chronotropic
- Modifies the rate
and rhythm of the
hearts conduction
system
- Positive:
Increases
heart rate
- Example:
Epinephrine
- Example:
Epinephrine
- Negative:
Decreases
heart rate
- Example:
Digitalis
- Example:
Digitalis
- Positive:
Increases
heart rate
- Modifies the rate
and rhythm of the
hearts conduction
system
- Inotropic
- Several major classes.
Function to alter
conduction velocity, and
decrease impulse
conduction, reduce
contractility, and
automaticity of pace
maker cells and/or the
myocardium (Lewis,
2014).
- Anticoagulants
- Most frequently used for patients
with EF <20% or those experiencing
atrial fibrillation to prevent
thrombus formation from turbulent
or stagnant blood flow
- Example: Warfarin
- ANTIDOTE:
VITAMIN K
- ANTIDOTE:
VITAMIN K
- Example: Warfarin
- Most frequently used for patients
with EF <20% or those experiencing
atrial fibrillation to prevent
thrombus formation from turbulent
or stagnant blood flow
- Selective Sinus
Node Inhibitor
- A newer class of medication that targets the Sinoatrial Node. The
desired effect is to lower the cardiac resting rate, decreasing
myocardial oxygen demand and preventing angina, while avoiding
the typical side effects of Beta-blocking agents (psychological
depression, erectile dysfunction, hypotension, and worsening of
Atrioventricular Node disease (Lewis, 2014; Nguyen et al, 2016).
- Assess patient's heart rate and
blood pressure before
administering any drug that
affects resting heart rate and
subsequently blood pressure.
- Example:
Ivabradine
- Example:
Ivabradine
- Assess patient's heart rate and
blood pressure before
administering any drug that
affects resting heart rate and
subsequently blood pressure.
- A newer class of medication that targets the Sinoatrial Node. The
desired effect is to lower the cardiac resting rate, decreasing
myocardial oxygen demand and preventing angina, while avoiding
the typical side effects of Beta-blocking agents (psychological
depression, erectile dysfunction, hypotension, and worsening of
Atrioventricular Node disease (Lewis, 2014; Nguyen et al, 2016).
- Pain Medication
- Opioid
- PRN as ordered
by physician to
treat chest pain,
or for palliative
care. Carefully
monitor
respiratory rate
and depth.
- Morphine
- ANTIDOTE:
NALOXONE
- ANTIDOTE:
NALOXONE
- Morphine
- PRN as ordered
by physician to
treat chest pain,
or for palliative
care. Carefully
monitor
respiratory rate
and depth.
- Opioid
- Beta Blockers
- Surgical
Intervention
- Heart Valve
Repair/
Replacement
- Surgery to repair or to replace a dysfunctional
valve of the heart. Most commonly performed
on the MITRAL (or bicuspid) valve between the
left ventricle and left atria. This valve
experiences the greatest amount of backward
force during the ejection of blood volume from
the left ventricle out to systemic circulation
- Surgery to repair or to replace a dysfunctional
valve of the heart. Most commonly performed
on the MITRAL (or bicuspid) valve between the
left ventricle and left atria. This valve
experiences the greatest amount of backward
force during the ejection of blood volume from
the left ventricle out to systemic circulation
- Mechanical
Assist
Device
- A man-made pump that helps the
heart to beat more effectively
- Intra-Aortic
Balloon
Pump
- A balloon placed within the
aorta that inflates and
deflates at a specific rate to
assist the heart's left ventricle
after an acute cardiac event
(myocardial infarction, etc).
By inflating with each beat,
the balloon relieves the
workload of the heart by
decreasing resistance through
the aorta (Heart and Stroke
Foundation, 2018).
- A balloon placed within the
aorta that inflates and
deflates at a specific rate to
assist the heart's left ventricle
after an acute cardiac event
(myocardial infarction, etc).
By inflating with each beat,
the balloon relieves the
workload of the heart by
decreasing resistance through
the aorta (Heart and Stroke
Foundation, 2018).
- Total Artificial
Heart
- Research is ongoing to build a
functional totally artificial heart and
only a few trials exist in a small
number of research facilities (Heart
and Stroke Foundation, 2018).
- Research is ongoing to build a
functional totally artificial heart and
only a few trials exist in a small
number of research facilities (Heart
and Stroke Foundation, 2018).
- Implantable
Ventricular Assist
Device
- Called a VAD or VAS, this
mechanical device takes
over the heart's
ventricles by beating
for/assisting the heart.
Patients with VADs have
severely weakened
hearts or are in
end-stage heart failure
(Heart and Stroke
Foundation, 2018)
- Called a VAD or VAS, this
mechanical device takes
over the heart's
ventricles by beating
for/assisting the heart.
Patients with VADs have
severely weakened
hearts or are in
end-stage heart failure
(Heart and Stroke
Foundation, 2018)
- Intra-Aortic
Balloon
Pump
- A man-made pump that helps the
heart to beat more effectively
- Implantable
Pace Maker
- Surgeons implant a
device designed to
regulate an abnormal
heart rhythm
(particularly if it is
unresponsive to
medication)
- Sternotomy: Similar to a
thoracotomy, wherein
the patient's chest wall
is opened and leads are
advanced into the heart
(Heart and Stroke
Foundation, 2018)
- Thoracotomy: Open Chest
surgery. Small oval shaped
pads are sewn onto the
epicardium and the chest is
closed (Heart and Stroke
Foundation, 2018).
- Transvenous Approach: Leads
are manipulated onto the
endocardium through a
venous access port by a
surgeon (Heart and Stroke
Foundation, 2018)
- Subxiphoid Approach:
Similar to a thoracotomy,
except that the incision is
made to the left of the
breast bone (Heart and
Stroke Foundation, 2018).
- Internal Cardioverter
Defibrillator (ICD)
may or may not be
required in
management of
lethal dysrhythmias
- Sternotomy: Similar to a
thoracotomy, wherein
the patient's chest wall
is opened and leads are
advanced into the heart
(Heart and Stroke
Foundation, 2018)
- Surgeons implant a
device designed to
regulate an abnormal
heart rhythm
(particularly if it is
unresponsive to
medication)
- Coronary
Bypass
Surgery
- Surgical procedure designed
to improve coronary
bloodflow to the heart
muscle itself. Also
commonly referred to as
CABG surgery. Required
when coronary arteries are
completely blocked
(atherosclerosis) and a
detour must be built around
the blockage.
- A section of vein or
artery is removed from
one part of the body and
grafted into the heart to
create a new pathway
for coronary blood
supply to reach the heart
muscle. Percutaneous
coronary intervention
may also be used in
place of CABG.
- CABG surgery is not a
curative intervention.
Lifestyle changes must
be part of the patient's
treatment plan
- CABG surgery is not a
curative intervention.
Lifestyle changes must
be part of the patient's
treatment plan
- A section of vein or
artery is removed from
one part of the body and
grafted into the heart to
create a new pathway
for coronary blood
supply to reach the heart
muscle. Percutaneous
coronary intervention
may also be used in
place of CABG.
- Surgical procedure designed
to improve coronary
bloodflow to the heart
muscle itself. Also
commonly referred to as
CABG surgery. Required
when coronary arteries are
completely blocked
(atherosclerosis) and a
detour must be built around
the blockage.
- Cardioversion
- A process of restoring the heart's
normal rhythm by using electric
current - similar to defibrillation but at
much lower energy settings. The
application of energy interrupts
dysrhythmias (ie. atrial fibrillation) and
allows the heart to naturally reset
(Heart and Stroke Foundation, 2018).
- Chemical cardioversion is
performed for the same
purposes but with the use of
medications rather than
electrical current to reset an
abnormal heart rhythm
- Chemical cardioversion is
performed for the same
purposes but with the use of
medications rather than
electrical current to reset an
abnormal heart rhythm
- A process of restoring the heart's
normal rhythm by using electric
current - similar to defibrillation but at
much lower energy settings. The
application of energy interrupts
dysrhythmias (ie. atrial fibrillation) and
allows the heart to naturally reset
(Heart and Stroke Foundation, 2018).
- Atherectomy
- This procedure is similar to angioplasty. A
catheter is threaded through the femoral
artery, the fatty plaque is scraped away from
the inside of the arteries and collected in the
catheter. This procedure restores coronary
circulation. After the procedure, a surgeon
may choose to place a stent additionally
(Heart and Stroke Foundation, 2018).
- This procedure is similar to angioplasty. A
catheter is threaded through the femoral
artery, the fatty plaque is scraped away from
the inside of the arteries and collected in the
catheter. This procedure restores coronary
circulation. After the procedure, a surgeon
may choose to place a stent additionally
(Heart and Stroke Foundation, 2018).
- Heart Valve
Repair/
Replacement
- Medications
- Managing Heart Failure at Home.
Patients will receive education on heart
failure and understand it is a
progressive disease. Treatment and care
plans are based around improving
quality of life (Lewis, 2014)
Annotations:
- Patient education before discharge is very important. Nurses should discuss modifiable risk factors when the patient is ready to learn. Modifiable risk factors include: Smoking, diet, reducing salt intake, reducing fluid intake, increasing exercise within tolerance to strengthen the heart muscle, maintaining a healthy body weight, avoiding foods high in cholesterol, and carefully controlling any endocrine disorders like diabetes or thyroid disorders (Heart and Stroke Foundation of Canada, 2018).
- Smoking
cessation
- Smoking triples the risk of
heart disease for middle
aged men and women in
Canada (Heart and Stroke
Foundation, 2018)
- People diagnosed with heart failure
can use nicotine patches, puffers,
tablets or chewing gum as a
nicotine substitutes while they
decrease their tobacco use.
Physicians will often add these
nicotine supplements onto a
patient's MAR as a method of
ensuring the body is not under
stress with drawl while it recovers.
These interventions may be used in
conjunction with counseling
therapy.
- People diagnosed with heart failure
can use nicotine patches, puffers,
tablets or chewing gum as a
nicotine substitutes while they
decrease their tobacco use.
Physicians will often add these
nicotine supplements onto a
patient's MAR as a method of
ensuring the body is not under
stress with drawl while it recovers.
These interventions may be used in
conjunction with counseling
therapy.
- Smoking triples the risk of
heart disease for middle
aged men and women in
Canada (Heart and Stroke
Foundation, 2018)
- Exercise
- Within tolerance, and
under the direction of a
physician (Canadian
Society of Exercise
Physiology, 2018).
- Mild
- Walking
- Gardening
- Stretching
- Walking
- Moderate
- Brisk Walking
- Biking
- Dancing
- Swimming
- Brisk Walking
- Vigourous
- Basketball
- Jogging
- Fast Swimming
- Hockey
- Aerobics
- Basketball
- Mild
- Within tolerance, and
under the direction of a
physician (Canadian
Society of Exercise
Physiology, 2018).
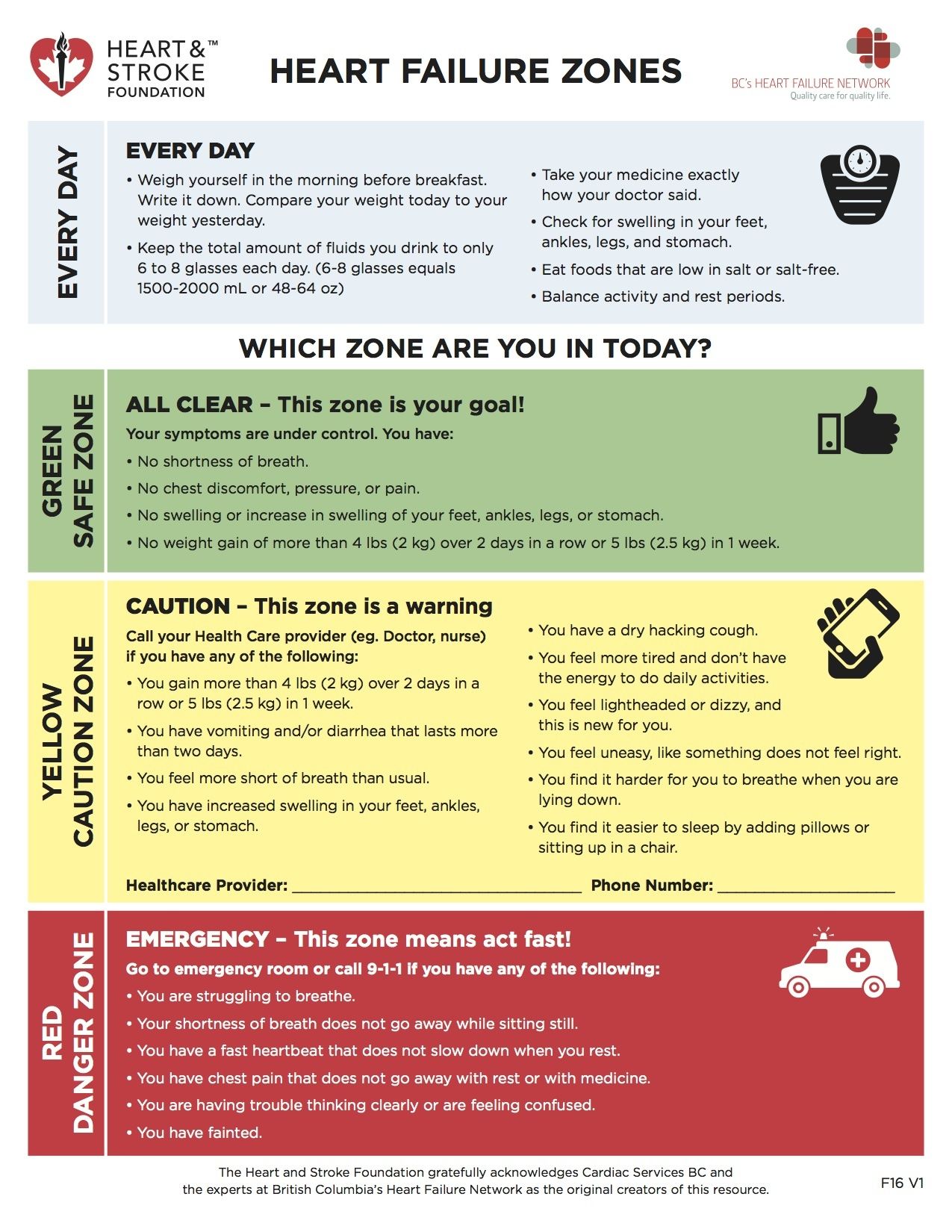
- Heart Failure Zones:The heart
failure zone chart is an excellent
way for patients to visualize the
importance of management of
symptoms and early recognition of
complications or exacerbation of
heart failure. Ensuring that clients
have the knowledge and control
over the management of their
health is integral to avoiding
repeated and longer hospital stays.
Annotations:
- HEART FAILURE ZONES. (n.d.). [JPEG] Accessed on 16 March 2018. Retrieved from http://www.heartandstroke.ca/get-healthy
- GREEN ZONE: All Clear. There is an
absence of symptoms (No chest pain, No
shortness of breath, No weight gain, No
swelling in feet, ankles, legs or
abdomen):
- YELLOW ZONE: Caution - This is a warning zone.
Symptoms start to show again. Some shortness of
breath, weight gain, vomiting/diarrhea that last
more than 2 days, light headedness, dry hacking
cough, difficulty sleeping and low energy
- RED ZONE: EMERGENCY ZONE! You need to act fast!
Shortness of breath that does not subside with
rest, chest pain that does not subside with rest,
confusion, loss of consciousness, racing heart beat
and you struggle to breathe
- Diet
- Foods to
Avoid
- Processed Food
- White
pasta
- White Bread
- Hot Dogs
- Frozen Pizza
- Deli Meat
- White
pasta
- Salty Food
- Potato
Chips
- Canned
Foods
- Potato
Chips
- Sugary Foods
- Cookies
- Cookies
- Saturated and
Trans Fats
- Fried Foods
- Fried Foods
- Foods High in
Cholesterol
- Processed Food
- Canada's Food Guide and Heart
Healthy Foods (Heart and Stroke
Foundation, 2018; Canada's Food
Guide, 2018)
- 7-10 servings
of vegetables
and fruits
- Choose Whole
grain foods
- Wild Rice
- Oats
- Quinoa
- Whole Grain Bread
- Hulled Barley
- Wild Rice
- Protein
- White Fish
(aim for 2
servings per
week)
- Tofu
- Dairy and Milk
Products
- Beans
- Lentils
- White Fish
(aim for 2
servings per
week)
- 7-10 servings
of vegetables
and fruits
- Fluid
Restrictions
- A good technique to teach
patients who are new to
monitoring their fluid intake,
recommend filling a 2L cola
bottle with water to be used
throughout the day. Once the
2L bottle of water is empty,
the patient has reached their
daily limit of fluid intake
- A good technique to teach
patients who are new to
monitoring their fluid intake,
recommend filling a 2L cola
bottle with water to be used
throughout the day. Once the
2L bottle of water is empty,
the patient has reached their
daily limit of fluid intake
- Foods to
Avoid
- Reduce Stress
- Yoga
- Meditation
- Balanced
Diet
- Cut down on stimulants
(caffeine, energy drinks,
chocolate, tea and soft drinks)
- Setting Boundaries
- Get Enough
Sleep
- Yoga
- Support Systems. Patients ideally
should have a support system at
home. Those individuals with
advanced heart failure may
require assistance from CCAC or
home visit nurses. Having
supportive family members also
makes this transition safer and
less stressful for the person
managing heart failure.
- Spouse
- Family Members
- Home Visit
Nursing Care
- Close Friends
- CCAC
- Spouse
- Energy
Conservation
- Recommend pre
planning days when
possible, rest when
fatigued, and set rest
times for the
afternoon hours.
- Patients will benefit from
planning out activities that
require higher amounts of
energy and conserving
energy to optimize
independence in
completion of activities of
daily living (Lewis, 2014)
- Patients will benefit from
planning out activities that
require higher amounts of
energy and conserving
energy to optimize
independence in
completion of activities of
daily living (Lewis, 2014)
- Recommend pre
planning days when
possible, rest when
fatigued, and set rest
times for the
afternoon hours.
- Activity
Therapy
- Collaborate with
physical,
occupational,
psychological
and social
capabilities
- Help patient determine
commitment and provide
obtainable goals
- Help patient determine
commitment and provide
obtainable goals
- Collaborate with
physical,
occupational,
psychological
and social
capabilities
- Oxygen
therapy
Media attachments
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Mind Maps for free with GoConqr? Learn more.