12931939
AQA A Level psychology - Paper
3 Schizophrenia
- Classification of schizophrenia
- Affects 1% of pop. at some point in life.
- Diagnosis manual > DSM-V (US) =
classification & description of >200 mental
disorders, grouped on common features.
ICD-11(Europe)(= recent update).
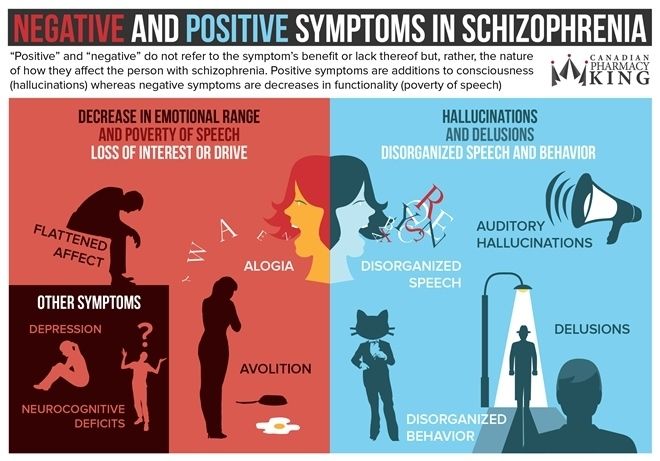
- Positive symptoms = reflect excess or distortion of normal functioning.
- Hallucinations
- Bizarre, unreal perceptions of environment> auditory
(hearing voices), visual (seeing lights/ objects) , olfactory
(smelling things) or tactile (feelings of being touched) = all
things that others do not experience.
- Bizarre, unreal perceptions of environment> auditory
(hearing voices), visual (seeing lights/ objects) , olfactory
(smelling things) or tactile (feelings of being touched) = all
things that others do not experience.
- Delusions
- Bizarre , unreal beliefs > paranoia (being followed
or spied on), delusions of grandeur (inflated
beliefs on own power/importance) or delusions
of reference (events in environment appear
directly related to them).
- Bizarre , unreal beliefs > paranoia (being followed
or spied on), delusions of grandeur (inflated
beliefs on own power/importance) or delusions
of reference (events in environment appear
directly related to them).
- Disorganised speech
- Abnormal thought processes = can't
organising thoughts = derailment (slip from one topic
to another) & incoherent speech= gibberish > 'word
salad'
- Abnormal thought processes = can't
organising thoughts = derailment (slip from one topic
to another) & incoherent speech= gibberish > 'word
salad'
- Grossly disorganised
- Inability or motivation to do/complete task> day-to-day
difficulties = low interest in personal hygiene/ dress or
act bizarrely
- E.g. heavy clothes in summer
- E.g. heavy clothes in summer
- Inability or motivation to do/complete task> day-to-day
difficulties = low interest in personal hygiene/ dress or
act bizarrely
- catatonic behaviour
- Reduced reaction to immediate
environment, rigid posture, aimless
motor activity (movements)
- Reduced reaction to immediate
environment, rigid posture, aimless
motor activity (movements)
- Hallucinations
- Negative symptoms = reflect reduced or loss of normal functioning.
- Speech poverty
(alogia)
- Lessened speech fluency & productivity (reflects
blocked thoughts) = fewer words/ difficulty of
spontaneous speech/ less complex syntax. >
associated with long & earlier onset of illness.
- Lessened speech fluency & productivity (reflects
blocked thoughts) = fewer words/ difficulty of
spontaneous speech/ less complex syntax. >
associated with long & earlier onset of illness.
- Avolition
- Reduced self-initiated involvement in available
activities (e.g. can sit and do nothing for hours)
- Reduced self-initiated involvement in available
activities (e.g. can sit and do nothing for hours)
- Affective flattening
- Poor communication = Reduced range & intensity of
emotional expression + deficit in paralinguistic features.
- Poor communication = Reduced range & intensity of
emotional expression + deficit in paralinguistic features.
- Anhedonia
- Loss of interest in normally
pleasurable stimuli = physical (no pleasure from food,
bodily contact..), social (no pleasure from interacting
with others).
- Sarkar et al. > physical anhedonia = more reliable
symptom of schizophrenia [as social anhedonia overlaps
with other disorders (e.g. depression).
- Loss of interest in normally
pleasurable stimuli = physical (no pleasure from food,
bodily contact..), social (no pleasure from interacting
with others).
- Speech poverty
(alogia)
- Schiz. = Psychosis - severe mental disorder >
impaired thoughts & emotion = loss of contact
with external reality
- Diagnosed between ages 15-35 >
men & women affected equally.
- Affects 1% of pop. at some point in life.
- Reliability & validity in diagnosis and classification
- Reliability
- Diagnostic reliability = repeatability > test-retest reliability
(clinicians reach same conclusions at different points in time) /
inter-rater reliability (different clinicians reach same conclusions).
- Inter-rater reliability > measured by statistic = kappa score. 1 =
perfect inter-rater agreement (same conclusions on diagnonsis) . 0 =
no agreement (different conclusions). Kappa score ≥ 0.7 = good score.
- Regier at al. (2013) > DSM-V field trials -
diagnosis of schizophrenia kappa score = 0.46.
- Regier at al. (2013) > DSM-V field trials -
diagnosis of schizophrenia kappa score = 0.46.
- Inter-rater reliability > measured by statistic = kappa score. 1 =
perfect inter-rater agreement (same conclusions on diagnonsis) . 0 =
no agreement (different conclusions). Kappa score ≥ 0.7 = good score.
- Cultural differences in diagnosis
- Research suggests> significant variation between countries when
diagnosing schizophrenia = culture influences diagnostic process.
- Copeland (1971) > 134 US & 194 British
psychiatrists given description of
patient. 67% - US & 2% British
psychiatrists diagnosed schizophrenia.
- Copeland (1971) > 134 US & 194 British
psychiatrists given description of
patient. 67% - US & 2% British
psychiatrists diagnosed schizophrenia.
- Research suggests> significant variation between countries when
diagnosing schizophrenia = culture influences diagnostic process.
- = Consistency of
measurements
- Diagnostic reliability = repeatability > test-retest reliability
(clinicians reach same conclusions at different points in time) /
inter-rater reliability (different clinicians reach same conclusions).
- Validity
- Gender bias in diagnosis
- Diagnosis accuracy = gender dependant
- Bias in diagnostic categories
- Boverman et al. (1970) US clinicians equated healthy 'adult'
behaviour= healthy 'male' behaviour = androcentrism. =
tendency for women to be seen as less mentally healthy.
- Boverman et al. (1970) US clinicians equated healthy 'adult'
behaviour= healthy 'male' behaviour = androcentrism. =
tendency for women to be seen as less mentally healthy.
- Diagnosis accuracy = gender dependant
- = Whether observed effect is
genuine
- Symptom overlap
- Many pos./ neg. symptoms found in other
disorders, eg. depression/ bipolar.
- Ellason & Ross (1995) > People with Dissociative
identity disorder (DID) - have more schizophrenic
symptoms than people diagnosed with schizoprenia
- Ellason & Ross (1995) > People with Dissociative
identity disorder (DID) - have more schizophrenic
symptoms than people diagnosed with schizoprenia
- Many pos./ neg. symptoms found in other
disorders, eg. depression/ bipolar.
- Co-morbidity
- ≥ 2 conditions/disease co-occur in
schizophrenic patient (substance
abuse, anxiety, depression symptoms)
- Buckley et al. (2009) > 1/2 schizophrenic patients 50% =
co-morbid depression & 47% = co-morbid substance abuse.
- Buckley et al. (2009) > 1/2 schizophrenic patients 50% =
co-morbid depression & 47% = co-morbid substance abuse.
- ≥ 2 conditions/disease co-occur in
schizophrenic patient (substance
abuse, anxiety, depression symptoms)
- Gender bias in diagnosis
- Evaluation of valitidty
- Gender bias support from research > Loring & Powell (1988) > randomly selected 290 male
& female psychiastrists - given 2 case descriptions of patients' beh. Asked for judgement
using standard diagnostic criteria. 'male'/ 'no gender descriptions' patient = 56%
psychiatrists diagnosed schizophrenia. 'female' patient = 20% psychiatrists diagnosed
schizophrenia. = diagnosis dependant on patients gender = gender bias = low internal
validity.
- = some behavior seen as psychotic in males
was not seen as psychotic in females.
- = some behavior seen as psychotic in males
was not seen as psychotic in females.
- Problems with the validity = unsuitable
treatment may be administered, sometimes on
an involuntary basis = practical and ethical
issues when selecting different types of
treatment.
- Differences in prognosis (outcome forecast) - 20% recover
from previous level of functioning, 10% achieve sig./lasting
improvement, 30% some improvement + irregular relapses.
= low predicitve validity of schiz. diagnosis.
- Gender bias support from research > Loring & Powell (1988) > randomly selected 290 male
& female psychiastrists - given 2 case descriptions of patients' beh. Asked for judgement
using standard diagnostic criteria. 'male'/ 'no gender descriptions' patient = 56%
psychiatrists diagnosed schizophrenia. 'female' patient = 20% psychiatrists diagnosed
schizophrenia. = diagnosis dependant on patients gender = gender bias = low internal
validity.
- Evaluation of reliability
- Inter-rater reliability issues when diagnosing schiz. > Rosenhan (1973)
ON BEING SANE IN INSANE PLACES - PSEUDOPATIENTS (=fake
patients) 'normal' ppl presented themselves to psychiatric hospitals in
US - claimed hearing voice in head (pos. symptom) saying 'empty',
'hollow' & 'thud'. All diagnosed with schiz. & admitted into hospital.
Throughout stay, no staff recognised ppl actually normal.
- Implications of this = led to stricter, better defined
diagnosis of those with psychological disorders.
DSM-III used in study> led to update DSM-V.
- Implications of this = led to stricter, better defined
diagnosis of those with psychological disorders.
DSM-III used in study> led to update DSM-V.
- Jakobsen et al. (2005) tested ICD- 10 (classification system
commonly used in Europe) reliability. 100 Danish patients
with psychosis history assessed using operational criteria -
found concordance rate of 98% = high reliability of
diagnosis using updated classification.
- Inter-rater reliability issues when diagnosing schiz. > Rosenhan (1973)
ON BEING SANE IN INSANE PLACES - PSEUDOPATIENTS (=fake
patients) 'normal' ppl presented themselves to psychiatric hospitals in
US - claimed hearing voice in head (pos. symptom) saying 'empty',
'hollow' & 'thud'. All diagnosed with schiz. & admitted into hospital.
Throughout stay, no staff recognised ppl actually normal.
- Reliability
- Psychological explanations for schizophrenia
- Family dysfunction
- Double bind theory
- Gregory Bateson et al. (1956) child recieves frequent contradictory messages
from parent(s) - e.g "Love you" (verbal affection) while squeezing ear
(non-verbal hostility). = conflicting messages on different communicative levels.
- = confusion = prevents development of internally
coherent construction of reality = in long-run forms
schiz. symptoms (e.g. flattened effect/ withdrawal).
- = confusion = prevents development of internally
coherent construction of reality = in long-run forms
schiz. symptoms (e.g. flattened effect/ withdrawal).
- Psychiatrist Laing > argued schiz.
not disease & is reasonable
response to insane world,
- Gregory Bateson et al. (1956) child recieves frequent contradictory messages
from parent(s) - e.g "Love you" (verbal affection) while squeezing ear
(non-verbal hostility). = conflicting messages on different communicative levels.
- Expressed emotion (EE)
- Negative emotional climate/ high degree of
expressed emotions = family variable
associated with schiz.
- EE = communication style - schiz. patient talked about
in hostile manner by family members - indicating
emotional over-involvement/ over-concern.
- Kuipers et al. (1983) found high
EE relatives talk more, listen less.
- Kuipers et al. (1983) found high
EE relatives talk more, listen less.
- High EE level env. = likely influence to relapse rates
(increases symptoms).
- Linszen at al. (1997) patient returning to high EE
family = 4x more likely to relapse (than patient with
low EE family).
- Linszen at al. (1997) patient returning to high EE
family = 4x more likely to relapse (than patient with
low EE family).
- suggests schizophrenics - impaired coping
mechanisms = low tolerance for intensive env.
stimuli > particularly intense emotional
comments/family interactions = arouse schiz.
episode.
- Negative emotional climate/ high degree of
expressed emotions = family variable
associated with schiz.
- = abnormal communication
patterns within families
- Double bind theory
- Cognitive explanations
- = dysfunctional thought processing
- more evident in patients displaying postitive symptoms
(delusions/hallucinations)
- more evident in patients displaying postitive symptoms
(delusions/hallucinations)
- Cognitive explanations of
delusions
- delusions = bizzarre beliefs
- IMPAIRED INSIGHT/ COG. PROCESSING
- unable to recognise cognitive
distortions/ substitute more
realistic explanations for events
- Beck & Rector (2005) Delusions in schiz.
unaffected by 'reality testing' - patients unwilling/
unable to consider they may be wrong.
- Beck & Rector (2005) Delusions in schiz.
unaffected by 'reality testing' - patients unwilling/
unable to consider they may be wrong.
- unable to recognise cognitive
distortions/ substitute more
realistic explanations for events
- FAULTY STIMULUS INTERPRETATION
- Experiences interpreted by inadequate
information processing = formation of delusions
- Critical characteristic of delusional thinking =
degree person perceives themselves as central
component in events (egocentric bias) = jump
to conclusions about external events.
- Relating irrelevant events to themselves
= consequence of false conclusions.
- EXAMPLE - Muffled voices =
critisisms. Flashes of lights = signal
from God.
- EXAMPLE - Muffled voices =
critisisms. Flashes of lights = signal
from God.
- Relating irrelevant events to themselves
= consequence of false conclusions.
- Experiences interpreted by inadequate
information processing = formation of delusions
- delusions = bizzarre beliefs
- Cognitive explanations of
hallucinations
- hallucination = bizzarre perceptions
- Hallucinating ppl focus excessive attention on
auditory stimuli = hyper vigilance > have higher
expectancy for occurrence of voice than normal ppl.
- Aleman (2001) hallucination-prone have difficulty
distinguishing between imagery & sensory-based
perception> imagine sounds = self- generated auditory
- Aleman (2001) hallucination-prone have difficulty
distinguishing between imagery & sensory-based
perception> imagine sounds = self- generated auditory
- Baker & Morrison (198) Hallucinating patients
with schiz. = more likely to misattribute source
of self- generated auditory experience to
external source than non-hallucinating schiz.
- hallucinations also result from poor
'reality testing' of external events
- hallucination = bizzarre perceptions
- = dysfunctional thought processing
- Evaluation of family dysfuntion
- Noll (2009) supportive/ low EE family - can help recovery & reduce
anti-psychotic med. dependency = reduced likelihood of relapse
- Supports EE as factor affecting schizophrenic symptoms = real- world
app. - healthy family setting can be used to aid recovery.
- Supports EE as factor affecting schizophrenic symptoms = real- world
app. - healthy family setting can be used to aid recovery.
- Role of EE evidence in adoption studies > Tienari et al.
(1994) adopted children with schiz. biological parents =
more likely to develop schiz. (than those with non-schiz.
biological parents). ONLY if adopted family disturbed.
- = disorder forms under certain env. conditions (e.g.disturbed
family) = Genetic influence + env. conditions - both required
- = disorder forms under certain env. conditions (e.g.disturbed
family) = Genetic influence + env. conditions - both required
- Double bind theory support > Berger
(1965) found schizophrenics = higher
recall of double bind (contradictory)
statements by mothers (than non-
schizophrenics).
- Reliabililty is questionable - recall
may be affetced by schizophrenia.
- Reliabililty is questionable - recall
may be affetced by schizophrenia.
- Noll (2009) supportive/ low EE family - can help recovery & reduce
anti-psychotic med. dependency = reduced likelihood of relapse
- Evaluation of cognitive explanations
- NICE (2014) review of CBTp (involves evaluation of patients
faulty beliefs)= found to be more effective in treating symptom
severity & improving social functioning than anti-psychotic med.
- success shows dysfunctional thought
processing/cognitions = key component of schiz.
- success shows dysfunctional thought
processing/cognitions = key component of schiz.
- Reductionist explanation of schiz. - ignores
other factors, e.g. neurochemical changes.
- Howes & Murray (2014) Intergrated model of schiz. - vulnerability
factors (e.g. genes/birth complications..) + social stressors (e.g. social
adversity) = sensitised dopamine system - increased dopamine release
(combined with cog. processing bias = hallucinations.
- suggests combination of factors
lead to schiz. symptoms
- suggests combination of factors
lead to schiz. symptoms
- Howes & Murray (2014) Intergrated model of schiz. - vulnerability
factors (e.g. genes/birth complications..) + social stressors (e.g. social
adversity) = sensitised dopamine system - increased dopamine release
(combined with cog. processing bias = hallucinations.
- NICE (2014) review of CBTp (involves evaluation of patients
faulty beliefs)= found to be more effective in treating symptom
severity & improving social functioning than anti-psychotic med.
- Family dysfunction
- Drug therapy
- Typical antipsychotics
- = first generation/conventional drugs - e.g. chlorpromazine
- combat positive symptoms = hallucinations & delusions > products of overactive dopamine system.
- combat positive symptoms = hallucinations & delusions > products of overactive dopamine system.
- HIGH AFFINITY FOR D₂ RECEPTORS
- Basic mechanism = reduce dopamine effects
= reduced schiz. symptoms
- Dopamine ANTAGONISTS = bind to D₂ receptors in mesolimbic pathway > block
dopamine actions = reduced stimulation in mesolimbic dopaminergic pathway (in brain)
= eliminate hallucinations/delusions.
- Hallucinations & delusions usually diminish within few
days BUT other symptoms may take several weeks
- Kapur et al. (2000) estimate 60% - 75% of D₂ receptors in mesolimbic
dopamine pathway must be blocked for drugs to be effective = D₂ receptors
in other areas of brain must also be blocked = undesirable side effects
(extrapyramidal effects).
- = first generation/conventional drugs - e.g. chlorpromazine
- Atypical
antipsychotics
- = second generation drugs, e.g. clozapine.
- combat positive symptoms & claimed to have some beneficial effects negative symptoms + cognitive impairments.
- combat positive symptoms & claimed to have some beneficial effects negative symptoms + cognitive impairments.
- HIGHER AFFINITY FOR SEROTONIN RECEPTOR [5-HT₂A] THAN D₂ RECEPTORS
- 3 main differences to typical drugs
- Lower risk of extrapyramidal side
effects
- > due to ‘rapid disassociation’ (temporary
occupation of D₂ receptors = allow normal dopamine
transmission) = no movement problems as found
with typical drugs
- > due to ‘rapid disassociation’ (temporary
occupation of D₂ receptors = allow normal dopamine
transmission) = no movement problems as found
with typical drugs
- Beneficial effect on (positive +)
negative symptoms & cognitive
impairment
- Suitable for treatment-resistant
patients
- Lower risk of extrapyramidal side
effects
- = second generation drugs, e.g. clozapine.
- antipsychotics
- Increase patients subjective wellbeing &
helps them function as well as possible.
- Recommended as initial treatment for schiz. symptoms... after which
clinicians combine meds & psychological therapy to manage disorder.
- Reduce positive symptoms in severely ill
- Help treat psychotic disorders, I,e,
bipolar depression/scizoprenia.
- Developed following discovery of dopamine on
1952 - found to have effect on dopamine
- Antipsychotic action = reduce dopaminergic transmission = reduced action of
dopamine neurotransmitter in areas of brain > associated with with
symptoms of schiz. [DOPAMINE HYPOTHESIS - biological explanation]
- Increase patients subjective wellbeing &
helps them function as well as possible.
- Evaluation
- Support for antipsychotic effectiveness > Leucht et al. (2012) meta-analysis of 65 studies
between 1959 & 2011 – 6000 patients. All pps stabilised on antipsychotics – then some
pps taken off & placed on placebo & remaining pps stayed on regular antipsychotics >
after 12 months - 64% on placebo relapsed & 27% on antipsychotic relapsed.
- Highly effective treatment for schiz. Symptoms = reduced relapse intensity
and frequency/cheap/easy for patient to administer/non-time consuming >
does not require regular visits to clinician for therapy = less dropout rate?
- Typical antipsychotics extrapyramidal side effects (affects 50% of patients)– caused
by blockage of 60-75% dopamine transmission > impact extrapyramidal brain region
= responsible for motor activity = Parkinsonian/tremors/impaired motor activity
- Atypical antipsychotics metabolic side effects > Mareno et al. (2010-12) Study on 90
adolescents on atypical antipsychotics (for various diagnoses) found significant weight gain
= on average 12 pounds in 70% of patients.
- Do not treat real cause & only treats symptoms >
stopping medication will most likely result in relapse.
- Support for antipsychotic effectiveness > Leucht et al. (2012) meta-analysis of 65 studies
between 1959 & 2011 – 6000 patients. All pps stabilised on antipsychotics – then some
pps taken off & placed on placebo & remaining pps stayed on regular antipsychotics >
after 12 months - 64% on placebo relapsed & 27% on antipsychotic relapsed.
- Typical antipsychotics
- Cognitive behavioural therapy for
psychosis (CBTp)
- Developed to treat residual (pos. & neg.) schiz. symptoms (that
persist despite use of antipsychotic med.) + improve patient’s
functioning.
- Evaluation
- Turner et al. (2014) significant effiectiveness in reducing positive
symptoms (when compared with other psychosocial interventions).
- Meta-analysis can result in unreliable conclusions about CBTp effectiveness > as study quality not
taken into account. E.g. some studies fail to randomly allocate pps to either CBTp or control condition.
- Juni et al. (2001) concluded methodologically weak trials
= biased findings on CBTp effectiveness.
- Wykes et al. (2008) found that more rigorous (high quality)
studies had weaker CBTp effects.
- Juni et al. (2001) concluded methodologically weak trials
= biased findings on CBTp effectiveness.
- Stafford et al. (2013) meta-analysis - CBT for those at risk of psychosis [risk ratio 0.54 at 95%
confidence interval] shown to possibly delay/prevent transition to psychosis at 12 months.
- Turner et al. (2014) significant effiectiveness in reducing positive
symptoms (when compared with other psychosocial interventions).
- Basic assumption of CBTp = ppl can have distorted beliefs
= influence inappropriate feelings & behaviours.
- For schiz. these are dysfunctional thought processing
= faulty interpretations of events = delusions
- CBTp used to help patient identify &
correct faulty interpretations.
- CBTp used to help patient identify &
correct faulty interpretations.
- For schiz. these are dysfunctional thought processing
= faulty interpretations of events = delusions
- Aim of CBTp = help ppl establish links between thought, feelings/
actions & symptoms + general level of functioning.
- Monitoring own situation = patient better able to consider
her ways of explaining why they feel/behave the way they
do = reduced distress + improved functioning [ from more
self-awareness & understanding].
- Monitoring own situation = patient better able to consider
her ways of explaining why they feel/behave the way they
do = reduced distress + improved functioning [ from more
self-awareness & understanding].
- Group sessions/ one-to-one.
- NICE (National Institution for Health & Care Excellence)
recommend at least 16 sessions for treating schiz.
- Nature of CBTp
- Patients encouraged to trace symptoms to origins [to get idea of how they
might have developed] + evaluate content of delusions/ hallucinations [to
consider ways they can test validity of faulty beliefs = ‘reality testing’.
- Patient set behavioural assignments e.g.
shower > improve general level of functioning.
- Patient develops own alternatives to previous maladaptive
(inappropriate) beliefs > by looking for other explanations & coping
strategies when assessing cause and effects & distorted thinking
- Patients encouraged to trace symptoms to origins [to get idea of how they
might have developed] + evaluate content of delusions/ hallucinations [to
consider ways they can test validity of faulty beliefs = ‘reality testing’.
- Phases of CBTp
- Assessment
- Patient expresses thoughts about experiences to therapist + realistic goals
for therapy set (patients current distress used as motivation for change)
- Patient expresses thoughts about experiences to therapist + realistic goals
for therapy set (patients current distress used as motivation for change)
- Engagement
- Therapist empathises with patients distress
- Therapist empathises with patients distress
- ABC model (Ellis)
- Activating events (A) that cause emotional & behavioural (B) consequences (C) to patient are
explained > allows for unhealthy beliefs (e.g. ‘ppl won’t like me if I tell them about my voices’) to
be rationalised, disputed and changed into healthy beliefs (e.g. ‘some may find it interesting’)
- Activating events (A) that cause emotional & behavioural (B) consequences (C) to patient are
explained > allows for unhealthy beliefs (e.g. ‘ppl won’t like me if I tell them about my voices’) to
be rationalised, disputed and changed into healthy beliefs (e.g. ‘some may find it interesting’)
- Normalisation
- 1 in 4 ppl suffer from mental disorders > unusual experiences/delusions/hallucinations =
reduces patients anxiety & isolation/less alienated & stigmatised = hope for their recovery.
- 1 in 4 ppl suffer from mental disorders > unusual experiences/delusions/hallucinations =
reduces patients anxiety & isolation/less alienated & stigmatised = hope for their recovery.
- Critical collaborative analysis –
- Gentle questioning to help patient understand illogical deductions & conclusions – e.g. ‘If the
voices are real, why can’t others here them ?’ (can result in no stress for patient if a
non-judgemental atmosphere of trust and empathy is created between therapist and patient)
- Gentle questioning to help patient understand illogical deductions & conclusions – e.g. ‘If the
voices are real, why can’t others here them ?’ (can result in no stress for patient if a
non-judgemental atmosphere of trust and empathy is created between therapist and patient)
- Developing alternative explanations
- Patient develops other explanations for previously unhealthy assumptions
- Patient develops other explanations for previously unhealthy assumptions
- Assessment
- Developed to treat residual (pos. & neg.) schiz. symptoms (that
persist despite use of antipsychotic med.) + improve patient’s
functioning.
- Family therapy
- KEY STUDY : Pharoah at al. (2010) meta-analysis
- Procedure: Review of 53 published (RCTs = randomised controlled trial = random pps allocation) studies
(2002-2010) conducted in Europe, Asia & North America > family therapy effectiveness
- family therapy outcomes compared to 'standard' care (i.e, antipsychotic medication)
- Findings: MENTAL STATE = some studies reported improvement in family therapy patients compared to standard care patients BUT others did not.
COMPLIANCE WITH MED. = Family therapy increased patient's medication compliance (correct following of medical advice). SOCIAL FUNCTIONING
= Family therapy appeared to improve general functioning BUT did not have much of an effect on social functioning (e.g. living independently).
REDUCED RELAPSE/READMISSION = Family therapy reduced risk of relapse and hospital admission during treatment & 2 yrs after.
- Procedure: Review of 53 published (RCTs = randomised controlled trial = random pps allocation) studies
(2002-2010) conducted in Europe, Asia & North America > family therapy effectiveness
- family therapy outcomes compared to 'standard' care (i.e, antipsychotic medication)
- Range of interventions aimed at schiz.'s family >
schiz. guidance & management = psychoeducation
- Evaluation
- Lobban et al. (2013) analysed studies & found positive impact
on schiz. + family members > 60% of 50 family therapy
studies reported sig. positive impact - e.g. coping/problem
solving skills/relationship quality (including EE)
- HOWEVER poor methodology quality of studies = difficult
to distinguish effective from ineffective interventions
- HOWEVER poor methodology quality of studies = difficult
to distinguish effective from ineffective interventions
- Economic benefits of family therapy - NICE review of family therapy
studies > family therapy associated with sig. cost savings when offered
to schizophrenics alogside standard (antipsychotic drugs) care.
- cost savings from lower hospitalisation/relapse rates
(which fall during intervention + 24 months after)
- cost savings from lower hospitalisation/relapse rates
(which fall during intervention + 24 months after)
- Methodological limitations - Pharoah et al.
meta-analysis > some were chinese studies = Wu et al. >
random allocation of pps stated but not used.
- + lack of double blind = observer bias when
pps allocated > 10 /53 studies reported no
form of blinding + 16/53 did not mention use
- + lack of double blind = observer bias when
pps allocated > 10 /53 studies reported no
form of blinding + 16/53 did not mention use
- Effetiveness of family therapy = increased patient
medication compliance = correctly follow medical
advice/regime = increased benefits from meds
- Lobban et al. (2013) analysed studies & found positive impact
on schiz. + family members > 60% of 50 family therapy
studies reported sig. positive impact - e.g. coping/problem
solving skills/relationship quality (including EE)
- NICE recommend family therapy (=priority when symptoms persist & high relapse
risk) 'to all schizophrenics who are in contact with/live with family members'
- Research shown> higher relapse rate in schiz. when family
had high EE = high hostility & over-involvement
- Nature of family therapy
- 3-12 months -
atleast 10 sessions
- Aims to reduce family EE level = reduced
emotional climate (e.g. less anger/guilt)
- Garety et al. (2008) estimate family therapy
patients have 25% relapse rate & standard care
patients have 50% relapse rate.
- Involves active participation of schizophrenic & family
members = improves relationships as therapist
encourages open discussion of problems & negotiation
of potential solutions together = alliance formation
- Often used alongside drug treatment
for patient + outpatient clinical care
- 3-12 months -
atleast 10 sessions
- KEY STUDY : Pharoah at al. (2010) meta-analysis
- Token economy & the management of schizophrenia
- Token economy = form of behavioural (modification) therapy >
clinican set target (desirable) behaviours (e.g. brushing hair/)
believed to improve patient's engagement in daily activities.
- Evaluation
- Corrigan (1991) Difficult administration of token economy to
outpatients living in community> receive day treatment for few
hrs/day. In psychiatric hospital setting - patients recieve 24 hr care =
better control + monitoring in order to appropriately reward patients.
- positive results produced in outpatients =
difficult to maintain beyond hospital env.
- positive results produced in outpatients =
difficult to maintain beyond hospital env.
- Ethical concerns - to ensure effective reinforcement clinicans
may strictly control primary reinforcers (e.g. food, privacy..) =
basic human needs/ rights (to food, privacy...) violated
through manipulation of token economy programme.
- Atthowe and Krasner (1968) Use of token economy to modify
behaviour of chronic schizophrenics > significant increase in
performed reinforced desirable behaviours + improved
patient initiative, responsibility & social interaction.
- Dickerson et al. (2005) research support for token economy effectiveness in psychiatric
setting > reviewed 13 studies (that use token economy to treat schizophrenia). 11/13
studies reported beneficial effects directly attributed to use of token economy
- Corrigan (1991) Difficult administration of token economy to
outpatients living in community> receive day treatment for few
hrs/day. In psychiatric hospital setting - patients recieve 24 hr care =
better control + monitoring in order to appropriately reward patients.
- Assinging value to tokens
- Neutral token given 'value' through secondary reinforcement = token repeatedly paired
with/immediately before reinforcing stimulus (e.g. watching movie/food/incentives..) = token
acquired same reinforcing properties > can be used to modify behaviour
- classical conditioning
- classical conditioning
- Neutral token given 'value' through secondary reinforcement = token repeatedly paired
with/immediately before reinforcing stimulus (e.g. watching movie/food/incentives..) = token
acquired same reinforcing properties > can be used to modify behaviour
- Reinforcing target behaviours
- Sran & Borrero (2010) Use of 'generalised' reinforcer in session (token can be
exchanged for variety of privileges) = higher rates of target behaviours performed
in sessions [than the use of token that can be excahnged for single privilege]
- Sran & Borrero (2010) Use of 'generalised' reinforcer in session (token can be
exchanged for variety of privileges) = higher rates of target behaviours performed
in sessions [than the use of token that can be excahnged for single privilege]
- The 'trade'
- Kazdin (1977) Effectiveness of token economy decreases
if more time passes between presentation of token &
exchange for backup rewards (chosen by clinician)
- Frequent exchange periods (of tokens for
privilege) = quicker patient reinforcement
+ increased target behaviour frequency
- Kazdin (1977) Effectiveness of token economy decreases
if more time passes between presentation of token &
exchange for backup rewards (chosen by clinician)
- Token awarded when patient engages in target (desirable)
behaviour & can later be exchanged for privileges (e.g.access to tv)
- [Tokens paired with rewarding stimuli (privileges) = secondary reinforcement]
- Ayllon & Azrin (1968) Token economy on female schiz.
patient ward (many hospitalised for many yrs) > given 'one gift' plastic
tokens for target behaviours (e.g. domestic chores). Tokens exchanged
for privileges (e.g. watch movie). Use of token economy = dramatically
increased desirable behaviours performed by patients each day.
- Token economy = form of behavioural (modification) therapy >
clinican set target (desirable) behaviours (e.g. brushing hair/)
believed to improve patient's engagement in daily activities.
- Interactionist approach:
Diathesis-stress model
- Stress = environmental influence
- Evalution
- Treatment implications/real-world app. > Known factors to
interact with genetic vulnerability can be addressed - avoid
additive effect of diathesis (genetics) + stress (env. factors)
- Borglum et al. (2014) Women with gene defect + infected
with cytomegalovirus (type of virus) during pregnancy =
higher risk to have child who develops schiz. (only if both
mother & child have gene defect). Anti-viral medication
during pregnancy = prevent onset of schiz. in offspring.
- Borglum et al. (2014) Women with gene defect + infected
with cytomegalovirus (type of virus) during pregnancy =
higher risk to have child who develops schiz. (only if both
mother & child have gene defect). Anti-viral medication
during pregnancy = prevent onset of schiz. in offspring.
- Hammen (1992) argues maladaptive methods of
coping with stress in childhood & throughout
development = individual fails to develop effective
coping skills = compromised resilience + higher vulnerability.
- Life = highly stressful & may
trigger mental illness (e.g. schiz.)
[mention psychiatrist Laing]
- = stress may not be key factor in triggering schiz.
BUT may infact be individuals coping skills & how
they react to stressors in env. that trigger schiz.
- Life = highly stressful & may
trigger mental illness (e.g. schiz.)
[mention psychiatrist Laing]
- Tienari et al. key study limitations > OPAS scale assessed
adoptive family ONLY at one given point in time> does not
reflect developmental changes (& how family conditions may
have changed over time to produce/prevent schiz. onset)
- Urban environment not necessarily more stressful > Vassos
et al. suggests living in densely populated urban env. =
significant schiz. stress factor. HOWEVER Romans-Clarkson
et al. found NO urban-rural differences in mental health
[among women in New Zealand]
- Urbanisation as schiz. factor = highly simplistic.
Cultural & gender differences (beta bias)> Women in
New zealand non-representative of other cultures &/
males.
- Urbanisation as schiz. factor = highly simplistic.
Cultural & gender differences (beta bias)> Women in
New zealand non-representative of other cultures &/
males.
- Treatment implications/real-world app. > Known factors to
interact with genetic vulnerability can be addressed - avoid
additive effect of diathesis (genetics) + stress (env. factors)
- KEY STUDY: Tienari et al. (2004)
- PROCEDURE: Hopsital records of 20,000 women [admitted in Finnish
psychiatric hospitals between 1960-79] checked. Sample collected =
145 high risk (with schiz. mother) adopted children & 158 low risk
(non-schiz. mothers) adopted children > all assessed over 21 year
period (longitudinal study)+ adoptive family assessed using OPAS
- FINDINGS: 14 from total 303 (= 145 high risk + 158 low risk)
developed schiz. 11/14 from high risk group & 3/14 from low
risk group. Low OPAS rating = healthy adoptive family > has
protective effect from schiz. dev.. High OPAS rating =
disturbed adoptive family = stressor >trigger schiz.
- Adoptive family stress = predictor of schiz. development
- Adoptive family stress = predictor of schiz. development
- PROCEDURE: Hopsital records of 20,000 women [admitted in Finnish
psychiatric hospitals between 1960-79] checked. Sample collected =
145 high risk (with schiz. mother) adopted children & 158 low risk
(non-schiz. mothers) adopted children > all assessed over 21 year
period (longitudinal study)+ adoptive family assessed using OPAS
- Diathesis = biological infleunce
- Schizophrenia = result of biological & environmental influences
- Family studies > People have varying vulnerability levels (high/low) to schiz.
BUT going on to develop schizophrenia is determined by vulnerability (bio.)
level + level of stress experienced through lifetime (env.)
- Diathesis
- Genetics = determinant of schiz. vulnerability
- Twin studies > identical twin of
schizophrenic = higher risk of developing
schiz. than sibling/non-identical twin.
- Tienari et al. > adoptive relatives do NOT share increased risk as biological relaetives
- Tienari et al. > adoptive relatives do NOT share increased risk as biological relaetives
- 50% of identical twins - where one is diagnosed with schiz.
& other never meets diagnostic criteria for schiz.. This
discordance rate suggests env. plays role (in schiz. dev.)
- Genetics = determinant of schiz. vulnerability
- Stress
- Stressful life events (take many forms - e.g. childhood
trauma/ living in highly urbanised area) = schiz. trigger
- Varese et al. (2012) children experienced severe
trauma (=stressor) before age 16 = 3x more likely
to develop schiz. in later life.
- Vassos et al. (2012) meta-analysis > most
urban environments = 2.37x higher risk to
develop schiz. than most rural environments.
- + Research suggests> higher urbanisation level
associated with higher risk of developing
different psychoses, including schiz.
- Urban env. = poorer/adverse living conditions
- HOWEVER > many ppl live in
urban/densely populated areas BUT only
few develop schiz. = urban env. is
conditional to persons vulnerability level.
- Urban env. = poorer/adverse living conditions
- + Research suggests> higher urbanisation level
associated with higher risk of developing
different psychoses, including schiz.
- Stressful life events (take many forms - e.g. childhood
trauma/ living in highly urbanised area) = schiz. trigger
- Additive nature of diathesis + stress
- Several ways combination of diathesis + stress lead to schiz. onset
- E.g. Highly vulnerable individual + minor stressor = schiz. /
Low vulnerability individual + major stressor = schiz.
- E.g. Highly vulnerable individual + minor stressor = schiz. /
Low vulnerability individual + major stressor = schiz.
- Pre-supposed additivity = diathesis + stress
combine to produce disorder (=schiz.)
- Several ways combination of diathesis + stress lead to schiz. onset
- Stress = environmental influence
- Biological explanations for schizophrenia
Media attachments
{kind=link}
Want to create your own Mind Maps for free with GoConqr? Learn more.