13168422
Description
Mind Map by Fatma Shwaylia, updated more than 1 year ago
|
|
Created by Fatma Shwaylia
over 6 years ago
|
|
Urinary Bladder Cancer
- Hematuria
- More than 3 RBCs in centrifuged urine per
high-power field microscopy on properly
collected urine specimen (>3 RBC/HP)
- Classification
- Color
- Microscopic
- Gross
- Microscopic
- Source
- Urologic:
- from peripheral calyces
to external meatus
- from peripheral calyces
to external meatus
- Nephrologic
- glomerular
origin
- glomerular
origin
- Urologic:
- Color
- Etiology
- Urological:
- neoplasm, BPH, urolithiasis, infection,
trauma, iatrogenic, vascular
- neoplasm, BPH, urolithiasis, infection,
trauma, iatrogenic, vascular
- Nephrological
- Post-strep GN, SLE, HUS, Subacute
bacterial endocarditis, necrotizing
papillitis, periarteritis nodosa
- Post-strep GN, SLE, HUS, Subacute
bacterial endocarditis, necrotizing
papillitis, periarteritis nodosa
- Hematological
- Hemophilia, VW diseases, ITP, sickle
cell trait, DIC, anticoagulant therapy
- Hemophilia, VW diseases, ITP, sickle
cell trait, DIC, anticoagulant therapy
- Miscellaneous:
- Exercise hematuria, diseases of adjacent organs like the
appendix, idiopathic
- Exercise hematuria, diseases of adjacent organs like the
appendix, idiopathic
- Urological:
- Classification
- More than 3 RBCs in centrifuged urine per
high-power field microscopy on properly
collected urine specimen (>3 RBC/HP)
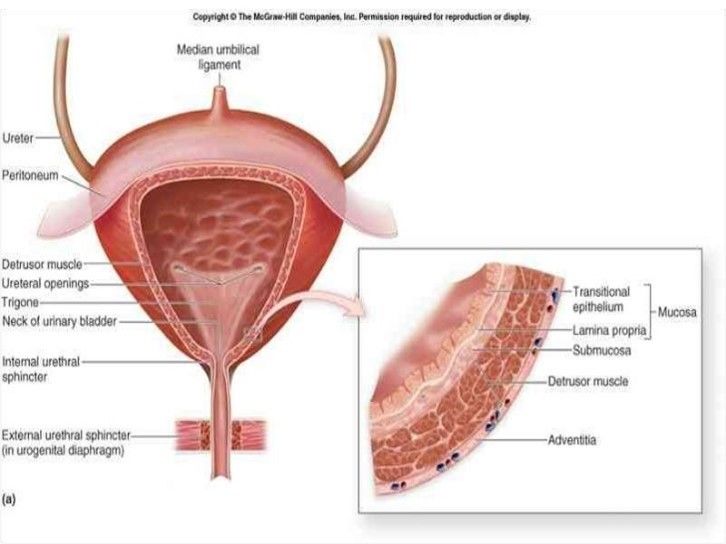
- ANATOMY AND HISTOLOGY OF URINARY BLADDER
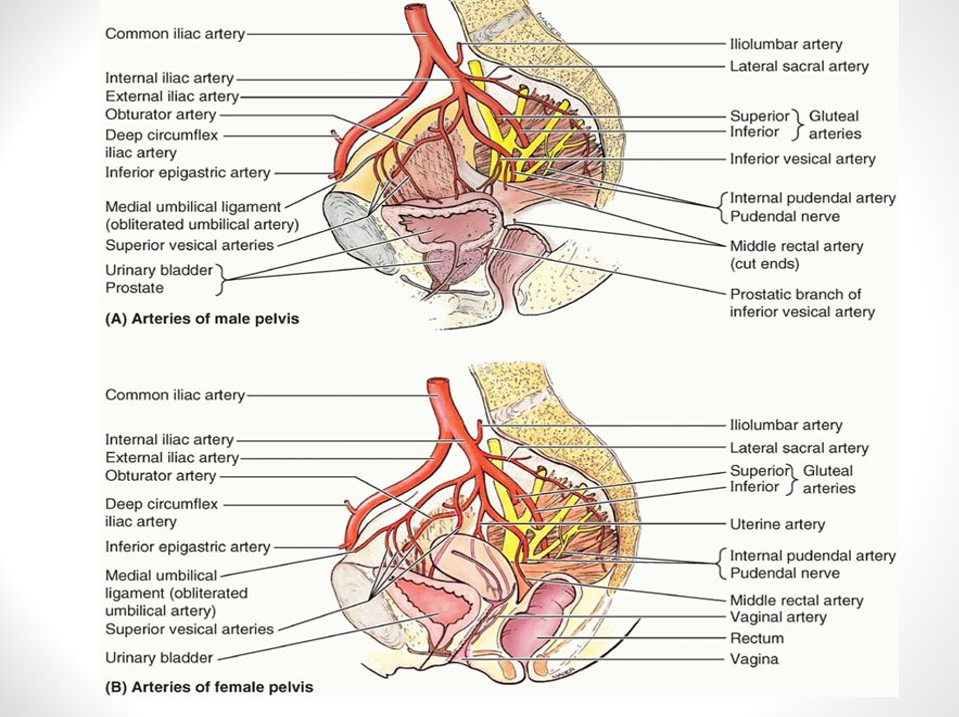
- Blood supply
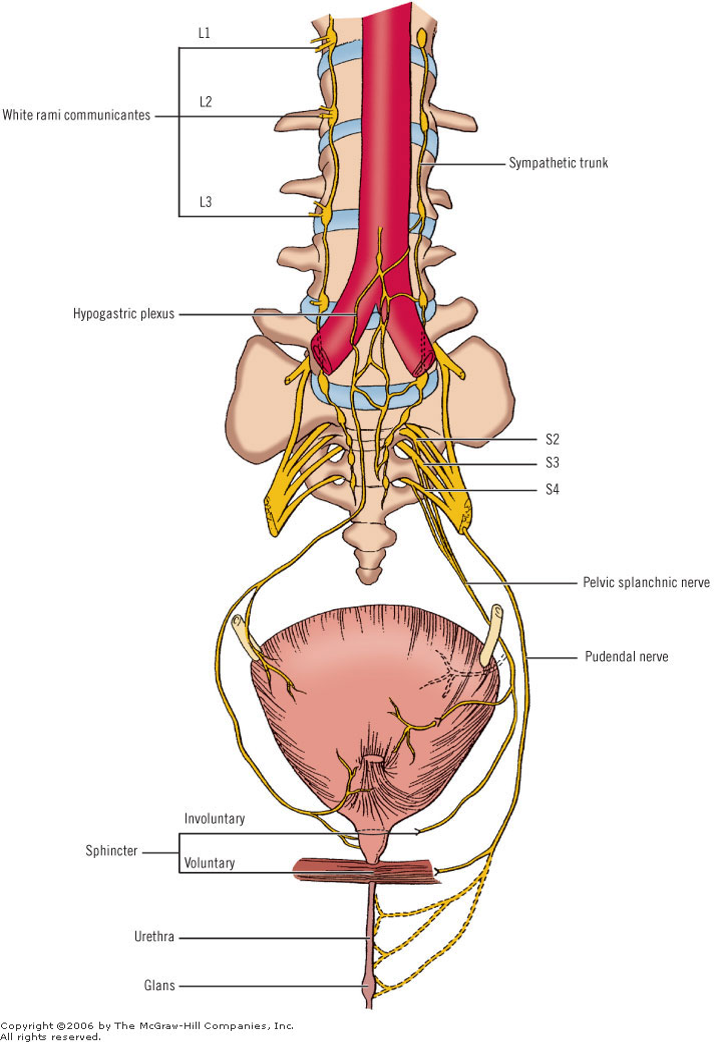
- Innervation
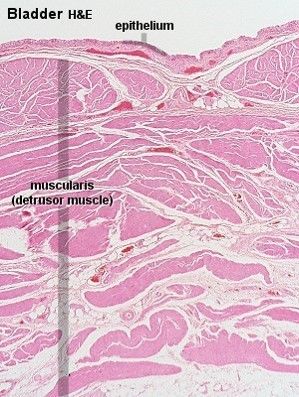
- Histology
- three layers of smooth
muscle, and a transitional
epithelium.
- The mucosa is heavily
folded - this helps to
accomodate for large
volume changes.
- The transitional epithelial lining can stretch
until it looks like stratified squamous
epithelium.
- three layers of smooth
muscle, and a transitional
epithelium.
- Blood supply
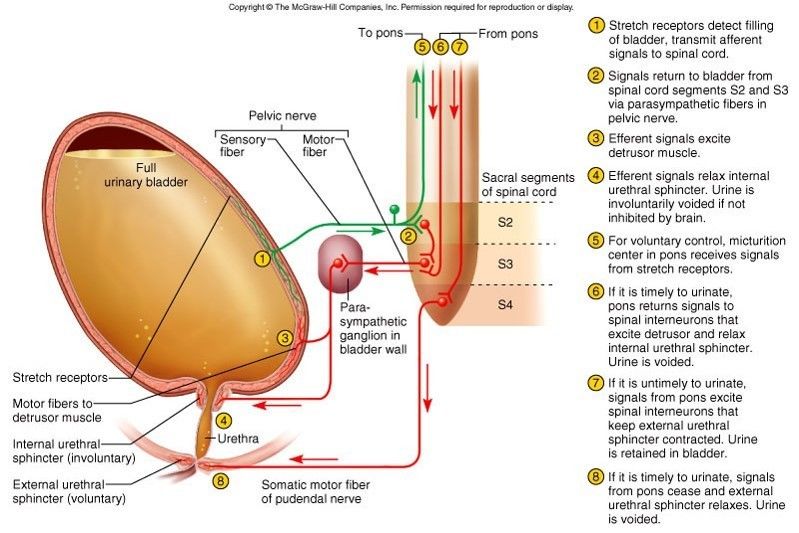
- PHYSIOLOGY OF micturition
- Micturition is the process by which the
urinary bladder empties when it becomes
filled.
- 2 main steps
- Filling stage
- the bladder fills progressively until the
tension in its walls rises above a
threshold level;
- the bladder fills progressively until the
tension in its walls rises above a
threshold level;
- Micturition reflex
- empties the bladder or, if this
fails, at least causes a
conscious desire to urinate
- empties the bladder or, if this
fails, at least causes a
conscious desire to urinate
- The micturition reflex is completely autonomic
spinal cord reflex but it can be inhibited or
facilitated by centres in the brain
- Filling stage
- 2 main steps
- Micturition is the process by which the
urinary bladder empties when it becomes
filled.
- Signs and symptoms
- Blood or blood clots in the urine.
- Pain or burning
sensation during
urination.
- Frequent urination.
- Feeling the need to urinate
many times throughout the
night.
- Lower back pain on 1
side of the body.
- Blood or blood clots in the urine.
- Risk Factors
- Smoking
- Increasing age
- Exposure to
certain chemicals
- Previous cancer treatment
- Chronic bladder inflammation
- Personal or family
history of cancer
- Smoking
- Staging of bladder cancer
- Investigations
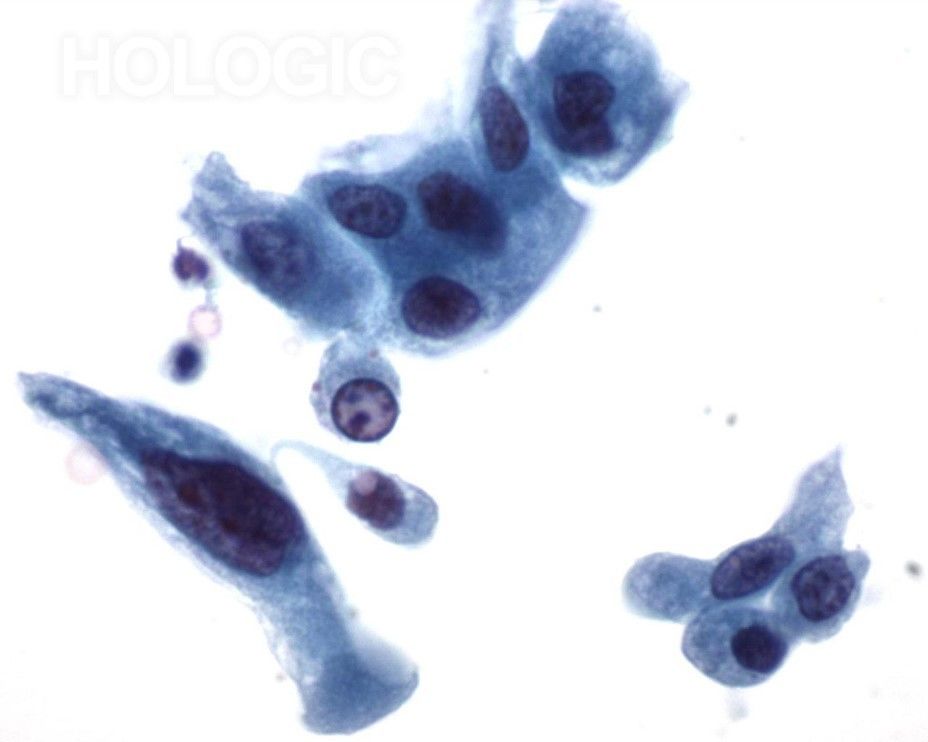
- Cytology
- most helpful in
diagnosing high-grade
tumors and
carcinoma in situ
(CIS).
- cytology is the most reliable urine test for
detecting bladder cancer, a positive
cytology finding should be treated as
indicating cancer until proven otherwise.
- If cystoscopy findings are negative in the setting of positive
cytology findings, further evaluation of the urinary tract is
required.
- The upper urinary tract should be evaluated with
contrast imaging. Cystoscopy with bilateral retrograde
pyelography and bilateral ureteral washings should be
performed.
- The upper urinary tract should be evaluated with
contrast imaging. Cystoscopy with bilateral retrograde
pyelography and bilateral ureteral washings should be
performed.
- If cystoscopy findings are negative in the setting of positive
cytology findings, further evaluation of the urinary tract is
required.
- CIS exfoliates cells that have an unusual
appearance and are easy to identify via
cytologic examination, prompting further
evaluation.
- cytology is the most reliable urine test for
detecting bladder cancer, a positive
cytology finding should be treated as
indicating cancer until proven otherwise.
- high grade papillary urothelial carcinoma
- most helpful in
diagnosing high-grade
tumors and
carcinoma in situ
(CIS).
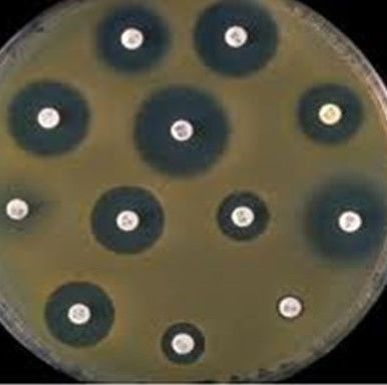
- culture sensitivity test
- Helps to find the right anti-biotic to kill an infecting
organism. This test determines the sensitivity of a
colony of bacteria to an antibiotic.
- The efficacy of an antibiotic can be
demonstrated under suitable conditions
by its inhibitory effect on micro
organisms.
- Sensitivity
analysis is a
useful tool
to help
quickly
determine if
bacteria are
resistant to
certain
drugs.
- Sensitivity
analysis is a
useful tool
to help
quickly
determine if
bacteria are
resistant to
certain
drugs.
- The efficacy of an antibiotic can be
demonstrated under suitable conditions
by its inhibitory effect on micro
organisms.
- Helps to find the right anti-biotic to kill an infecting
organism. This test determines the sensitivity of a
colony of bacteria to an antibiotic.
- Prostate specific antigen
- is a protein that is produced by the cells of the
prostate gland and enters the bloodstream.
- Raised PSA levels can indicate
several different disorders
involving the prostate, one of
which is prostate cancer.
- PSA testing is not 100% accurate. Some men who have prostate cancer will
not have elevated PSA levels (it is not 100% sensitive). Other
(noncancerous) conditions that cause the cells of the prostate to produce
higher levels of PSA include benign prostatic hyperplasia (BPH), urinary
tract infections, and prostatitis.
- PSA testing is not 100% accurate. Some men who have prostate cancer will
not have elevated PSA levels (it is not 100% sensitive). Other
(noncancerous) conditions that cause the cells of the prostate to produce
higher levels of PSA include benign prostatic hyperplasia (BPH), urinary
tract infections, and prostatitis.
- Raised PSA levels can indicate
several different disorders
involving the prostate, one of
which is prostate cancer.
- is a protein that is produced by the cells of the
prostate gland and enters the bloodstream.
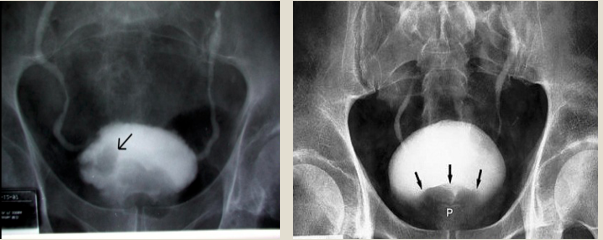
- An intravenous pyelogram (IVP)
- 1- round shadow on the right side of the urinary bladder later seen to
be a bladder cancer(LEFT).
- 2- benign prostatic hyperplasia. White = bladder , black = benign enlargement of the prostate,
pushing down on the inferior bladder. (RIGHT)
- 1- round shadow on the right side of the urinary bladder later seen to
be a bladder cancer(LEFT).
- Cytology
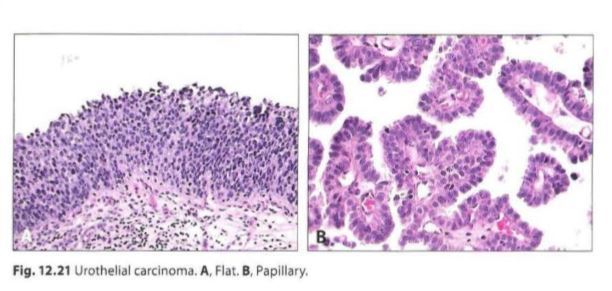
- Transitional cell carcinoma
- Malignant tumor arising from the urothelial lining of the renal
pelvis, ureter, bladder, or urethra
- Risk factors
- Cigrette smoke
- naphthylamine, azo
dyes, and long-term
cyclophosphamide or
phenacetin use.
- Cigrette smoke
- Arises via two distinct pathways
- Flat- develops as a high-grade flat
tumor and then invades; associated
with early p53 mutations
- Papillary-develops as a low-grade
papillary tumor that progresses to a
highgrade papillary tumor and then
invades; not associated with early p53
mutations
- Flat- develops as a high-grade flat
tumor and then invades; associated
with early p53 mutations
- Risk factors
- Malignant tumor arising from the urothelial lining of the renal
pelvis, ureter, bladder, or urethra
- SQUAMOUS CELL CARCINOMA
- Malignant proliferation of
squamous cells, usually
involving the bladder
- Arises in a background of squamous
metaplasia (normal bladder surface
is not lined by squamous
epithelium)
- Risk Factors
- chronic cystitis (older woman)
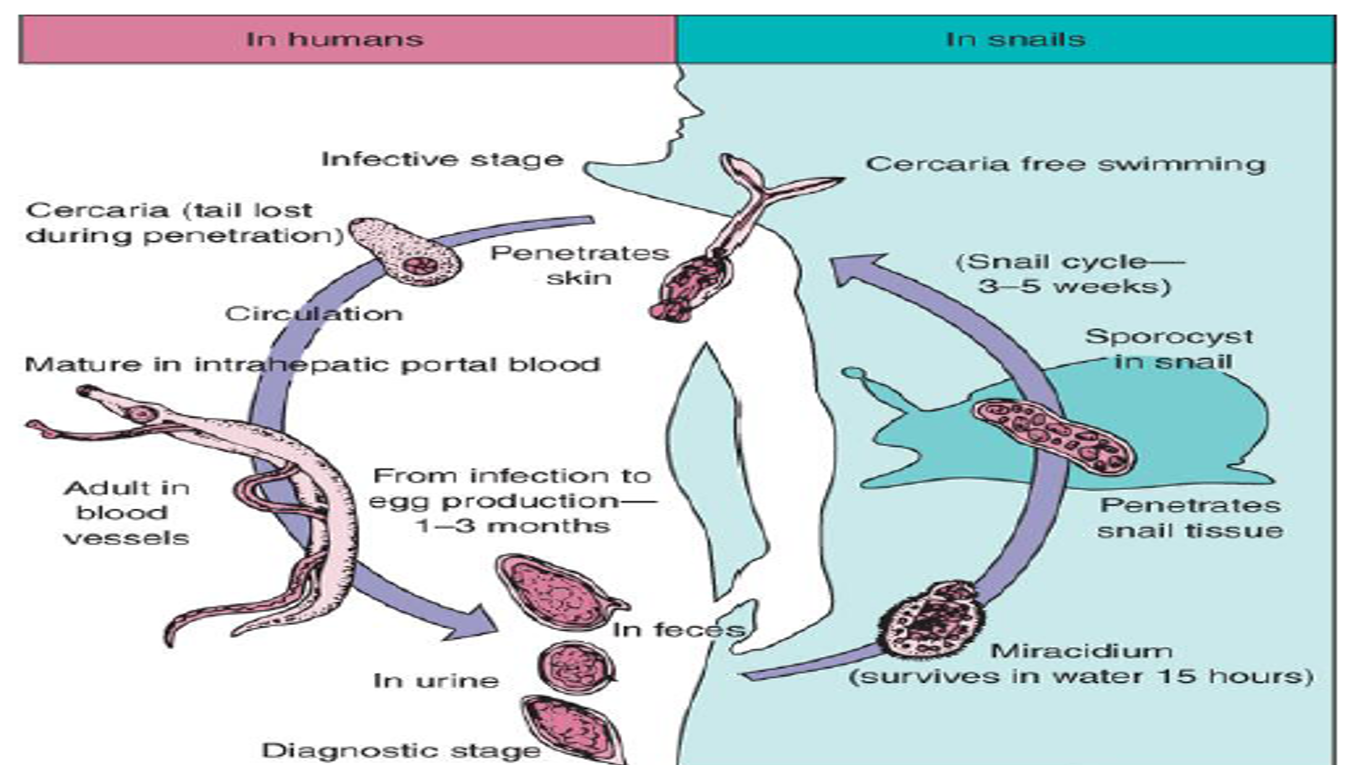
- Schistosoma hematobium infection (Egyptian male)
- S. haematobium:
eggs are laid in
small venules of
the vesical &
pelvic plexus
- eggs make their way from the venules
to bladder lumen for S. haematobium
- eggs make their way from the venules
to bladder lumen for S. haematobium
- Painless terminal haematuria
- Chronic cystitis with frequency of micturition & dysuria
- Generalised hyperplasia & fibrosis of
the bladder mucosa with a granular
appearance (Sandy patch)
- Formation of bladder stones due to deposition of oxalate & uric acid crystals
- Hydronephrosis
- Granuloma formation around schistosoma
eggs is a result of delayed hypersensitivity
reaction mediated by T-cell immune response
- S. haematobium:
eggs are laid in
small venules of
the vesical &
pelvic plexus
- long-standing nephrolithiasis
- chronic cystitis (older woman)
- Arises in a background of squamous
metaplasia (normal bladder surface
is not lined by squamous
epithelium)
- Malignant proliferation of
squamous cells, usually
involving the bladder
- ADENOCARCINOMA
- Malignant proliferation of glands, usually involving bladder
- Arises from a urachal remnant
(tumor develops at the dome of
the bladder), cystitis glandularis,
or exstrophy (congenital failure
to form the caudal portion of the
anterior abdominal and bladder
walls)
- Arises from a urachal remnant
(tumor develops at the dome of
the bladder), cystitis glandularis,
or exstrophy (congenital failure
to form the caudal portion of the
anterior abdominal and bladder
walls)
- Malignant proliferation of glands, usually involving bladder
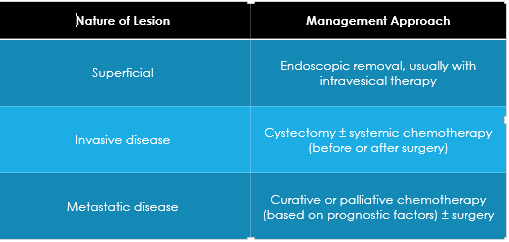
- Management
- Intra-vesical therapies are used in two general contexts: as an adjuvant to a complete endoscopic
resection to prevent recurrence
- invasive is to control of the primary tumor and, depending on the pathologic findings at surgery, systemic
chemotherapy to treat micro-metastatic disease
- Radical cystectomy - bladder-sparing approach
- Chemotherapy Alone is inadequate (radical cystectomy or
radiation therapy)
- complete endoscopic resection
- partial cystectomy
- combination of resection, systemic chemotherapy, and external beam
radiation therapy
- Chemotherapy Alone is inadequate (radical cystectomy or
radiation therapy)
- Intra-vesical therapies are used in two general contexts: as an adjuvant to a complete endoscopic
resection to prevent recurrence
- prognosis is affected by
- stage
- type
- tumors size
- age and general health
- stage
Media attachments
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Mind Maps for free with GoConqr? Learn more.