15318323
Traumatic Brain
injury
- Types of traumatic brain injury
- General types
- Open TBI
- is when the skull is fractured and penetrated
- is when the skull is fractured and penetrated
- Closed TBI
- No skull fracture
- No skull fracture
- Focal TBI
- Injury is is localized
- Injury is is localized
- Diffuse TBI
- Injury of wide area of brain
- Injury of wide area of brain
- Open TBI
- Specific Types
- Skull fractures
- Linear skull fracture
- usually a mild form of fracture that is usually managed by monitoring
- 75% of these fractures occur in the parietal bones
- usually a mild form of fracture that is usually managed by monitoring
- Depressed skull fracture
- Depresses brain tissue causing increase ICP
- Increased ICP presentation
- Depresses brain tissue causing increase ICP
- Basilar skull fracture
- a very serious type of skull fracture
- Racon eyes and CSF leakage
- a very serious type of skull fracture
- Diastatic skull fracture
- It happens in the sutures of the skull that causes them to widen.
- It happens in the sutures of the skull that causes them to widen.
- Linear skull fracture
- Diffuse Axonal injury
- Diagnosed by MRI
- The movement of a part of the
brain relative to another part
this will cause damage to the
axon integrity and function.
- irreversible
- it looks like a
multiple foci of
hemorrhage
- Diagnosed by MRI
- Hematomas
- Epidural
hemorrhage
- Fracture, injury of
middle meningeal artery
- Blood collects between
the dura and internal
surface of the skull and
compresses the brain
- The lesion may expand rapidly,
cause increased intracranial
pressure and herniation
- Lucid interval
of several
hours
- Lens-shaped
- Fracture, injury of
middle meningeal artery
- Subdural
hemorrhage
- Torn superficial bridging
veins between convexities
and dural venous sinuses
- The blood
collects between
the dura and the
outer layer of the
arachnoid.
- Contain clotted blood
- Stages
- Acute
- Clotted blood
- Hyperdense
- Clotted blood
- Subacute
- Lysis of clotted blood and
granulation tissue
development
- Isodense
- Lysis of clotted blood and
granulation tissue
development
- Chronic
- Connective
tissue
capsule
- Hypodense
- Connective
tissue
capsule
- Acute
- Torn superficial bridging
veins between convexities
and dural venous sinuses
- Subarachnoid
hemorrhage
- Can lead to
communicating
hydrocephalus
- Hyperdensity in
falx, sulci, sylvian
fissure
- could be
traumatic
or due to
ruptured
aneurysm
- Can lead to
communicating
hydrocephalus
- Intraventricular
hemorrhage
- Most commonly due
to rupture of sub
ependymal vessel.
- Most commonly due
to rupture of sub
ependymal vessel.
- Epidural
hemorrhage
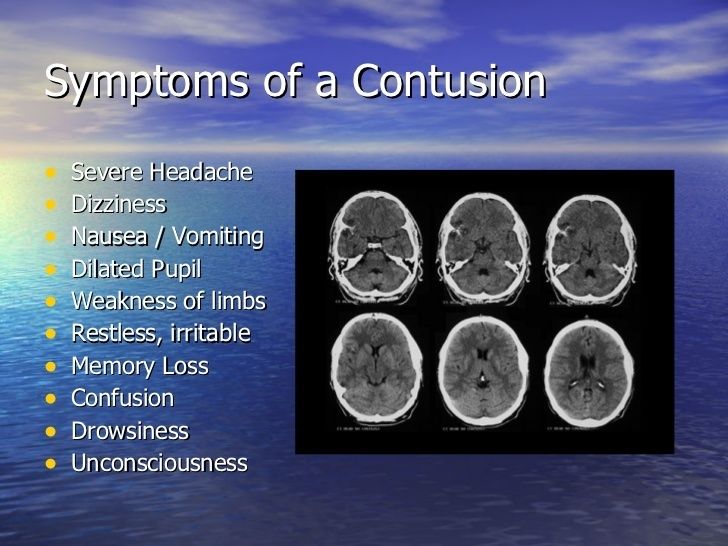
- Contusion
- bleeding on the
brain due to
localized trauma
- Focal
brain
hemorrhage
- After resolution, depressed
yellowish glial scar
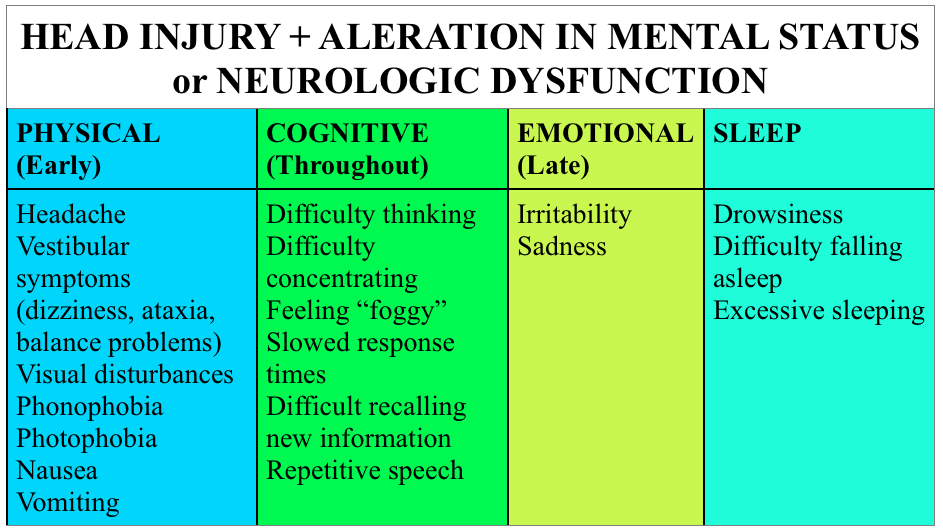
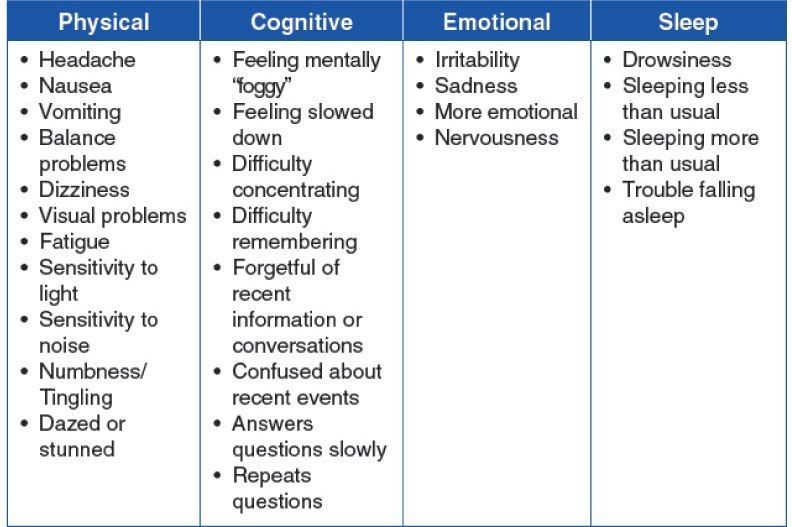
- Signs and symptoms
- Complications
- Seizures
Increased ICP
Cerebral
herniation - Loss
of memory-
Infections
- Seizures
Increased ICP
Cerebral
herniation - Loss
of memory-
Infections
- bleeding on the
brain due to
localized trauma
- Concussion
- widespread brain trauma due to a blow to the head, shaking, or a similar injury.
- Associated with
- Loss of consciousness
- Loss of refelx
- Respiratory distress
- Loss of consciousness
- No permanent structural damage
- complete recovery
- Signs and symptoms
- Complications
- Epilepsy
Post-concussion
Syndrome
Second-impact
Syndrome
Post-traumatic
headaches and vertigo
- Epilepsy
Post-concussion
Syndrome
Second-impact
Syndrome
Post-traumatic
headaches and vertigo
- widespread brain trauma due to a blow to the head, shaking, or a similar injury.
- Skull fractures
- General types
- Anatomy
- External anatomy of brain
stem
- Medulla
- Anterior surface
- The anterior median
fissure is located
ventrally and continues
into the spinal cord. On
either side of the
anterior median fissure
the pymmids are
located.
- Lateral to the
pyramid is an oval
olive
- position of the
inferior olivary
nucleus
- position of the
inferior olivary
nucleus
- The anterior median
fissure is located
ventrally and continues
into the spinal cord. On
either side of the
anterior median fissure
the pymmids are
located.
- Posterior surface
- Open medulla
- The hypoglossal
triangle lies over the
hypoglossal nucleus
- The
vestibutar
area
- The vagal
triangle covers
the dorsal vagal
nucleus
- The hypoglossal
triangle lies over the
hypoglossal nucleus
- Closed medulla
- Posterolateral to the olive is the inferior
cerebellar peduncle (connect medutla to
cerebellum). Dorsally there is a posterior
median sulcus
- On each side of the suicus Is
the gracile tubercle and
lateral to it is the cuneate
tubercle.
- Posterolateral to the olive is the inferior
cerebellar peduncle (connect medutla to
cerebellum). Dorsally there is a posterior
median sulcus
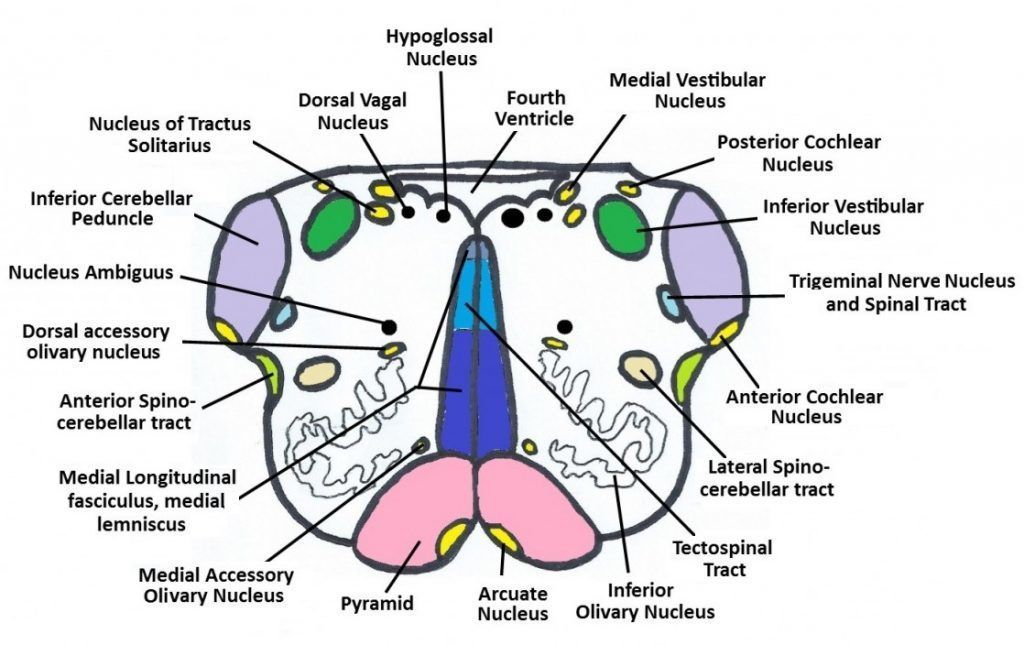
- Open medulla
- Anterior surface
- Pons
- Anterior surface
- is formed mainly Gf transversely
running fibers which pass through
the middle cerebellar peduncles
(forming a bridge [pons] between two
cerebllar hemispheres).
- is formed mainly Gf transversely
running fibers which pass through
the middle cerebellar peduncles
(forming a bridge [pons] between two
cerebllar hemispheres).
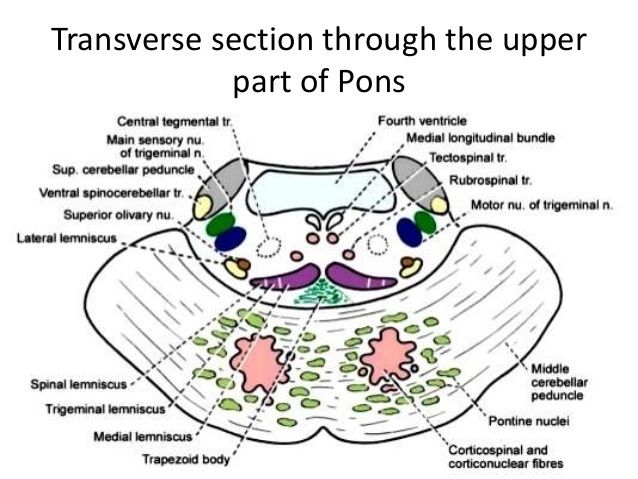
- Posterior surface
- forms part of the floor
of the 4m ventricle
- Facial colliculus: undertying root of facial nerve and nucleus of abducent nerve
- Locus ceruleus: deeply pigmented nen/e cells at the floor of the upper part of the sulcus limitans.
- Area vestibulae: underiying vestibular nuclei.
- forms part of the floor
of the 4m ventricle
- Anterior surface
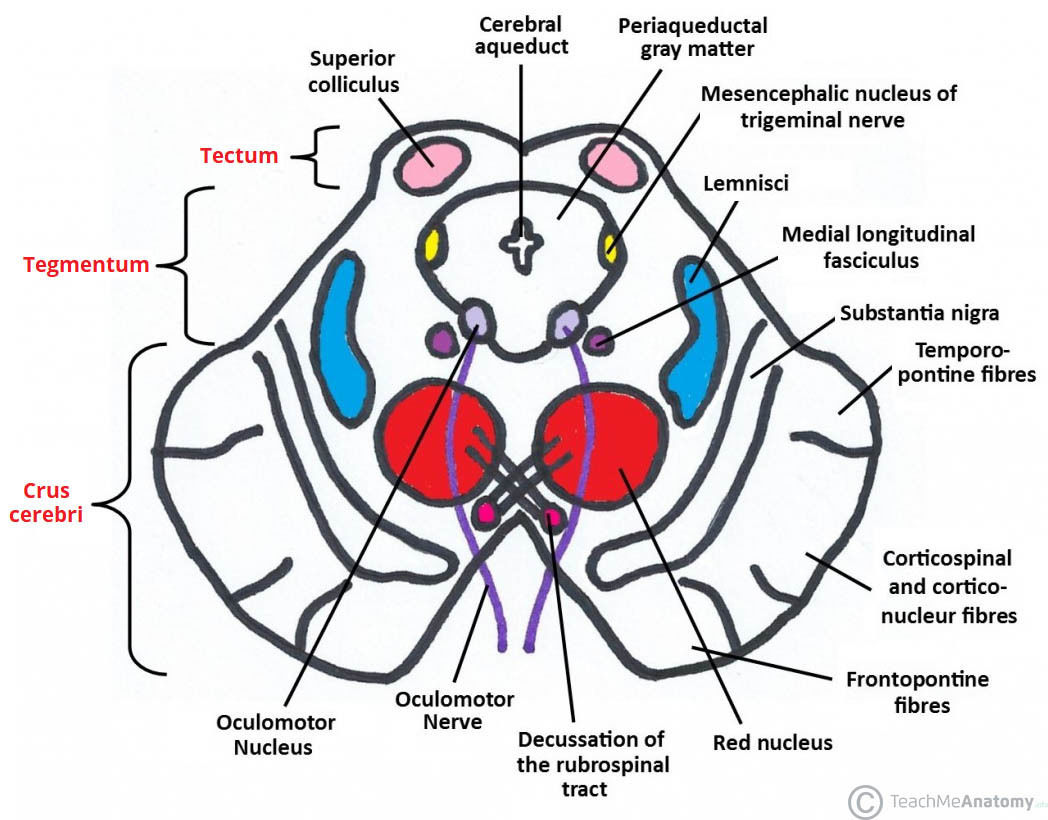
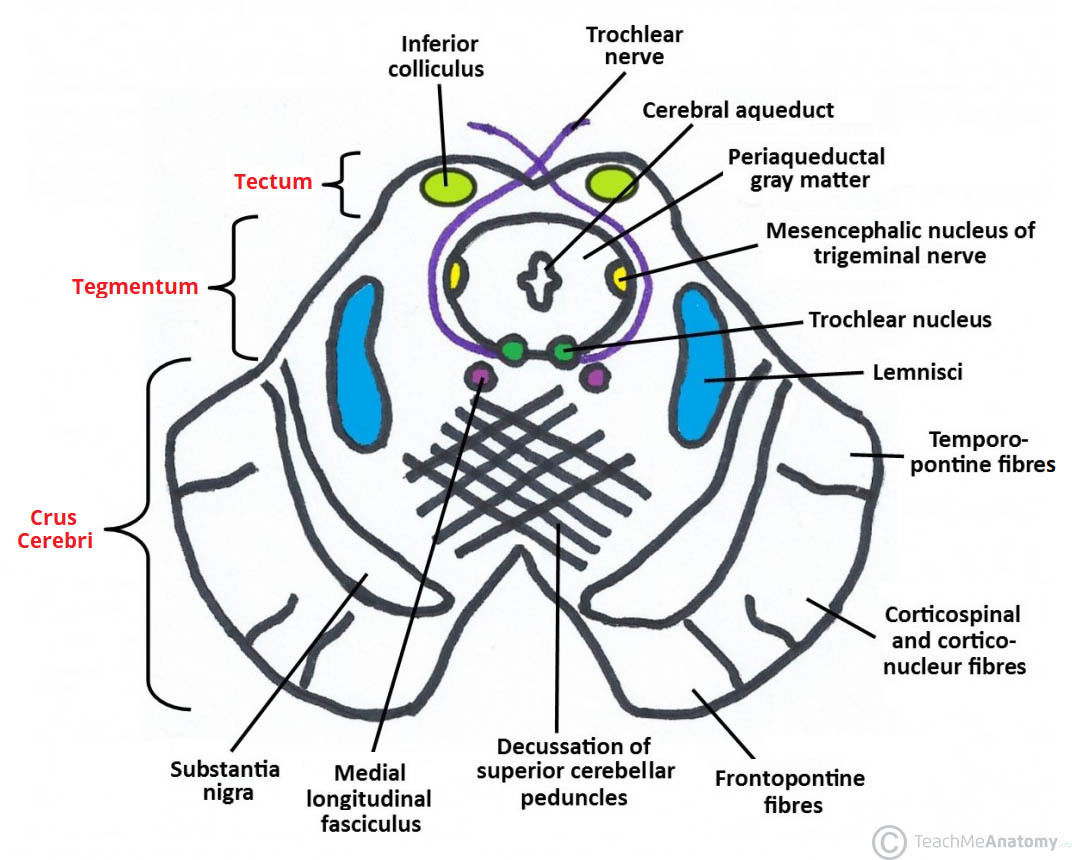
- Midbrain
- Anterior surface
- Cerebral peduncles
- Posterior perforated substance: between the
two cerebral peduncles pierced by multiple
central arteries.
- Posterior perforated substance: between the
two cerebral peduncles pierced by multiple
central arteries.
- Cerebral peduncles
- Posterior surface
- corpora quadrigemina
- Superior colliculi
- visual reflexes
- visual reflexes
- Inferior colliculi
- auditory function
- auditory function
- Superior colliculi
- corpora quadrigemina
- Anterior surface
- Medulla
- Internal
anatomy of
brain stem
- Medulla
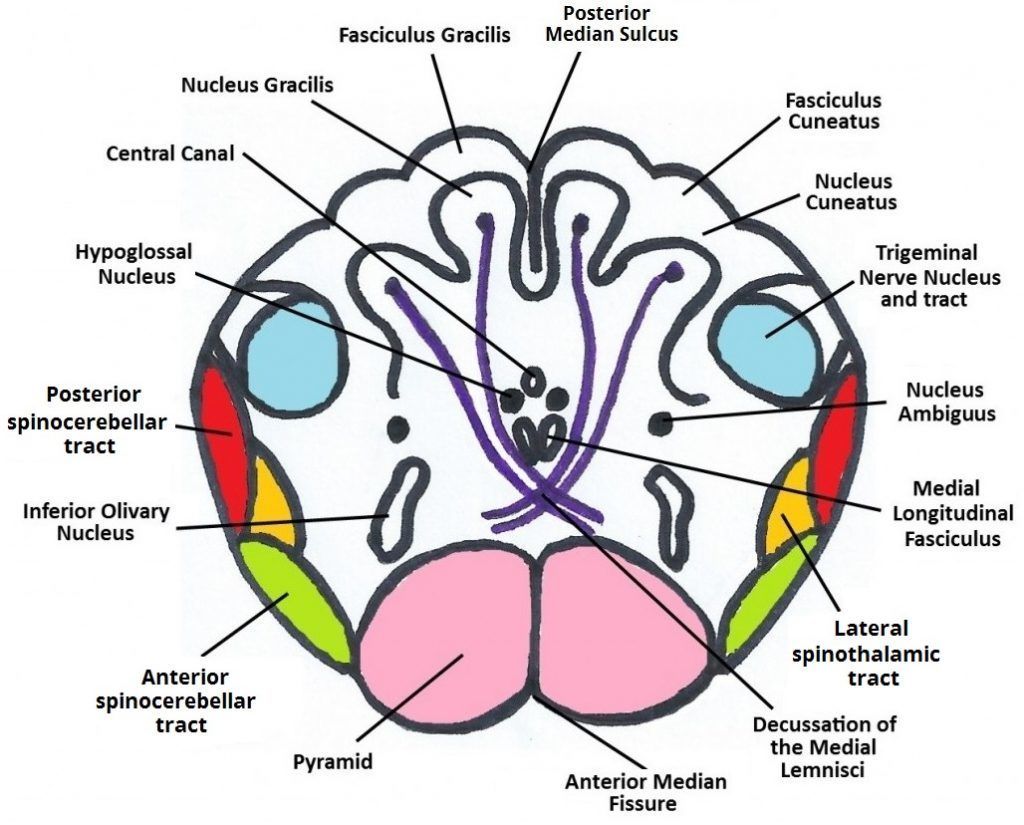
- Open medulla
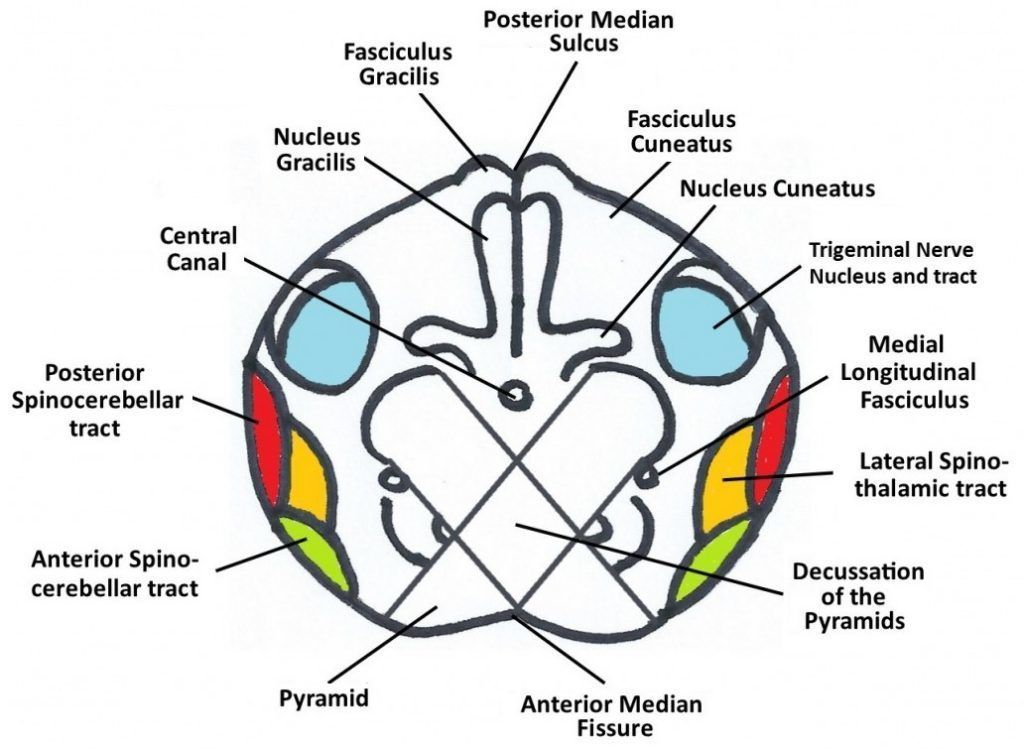
- Closed medulla
- Decussation
of the Medial
Lemniscus
- Decussation
of the
Pyramids
- Decussation
of the Medial
Lemniscus
- Open medulla
- Pons
- Midbrain
- inferior colliculi
- superior colliculus.
- inferior colliculi
- Medulla
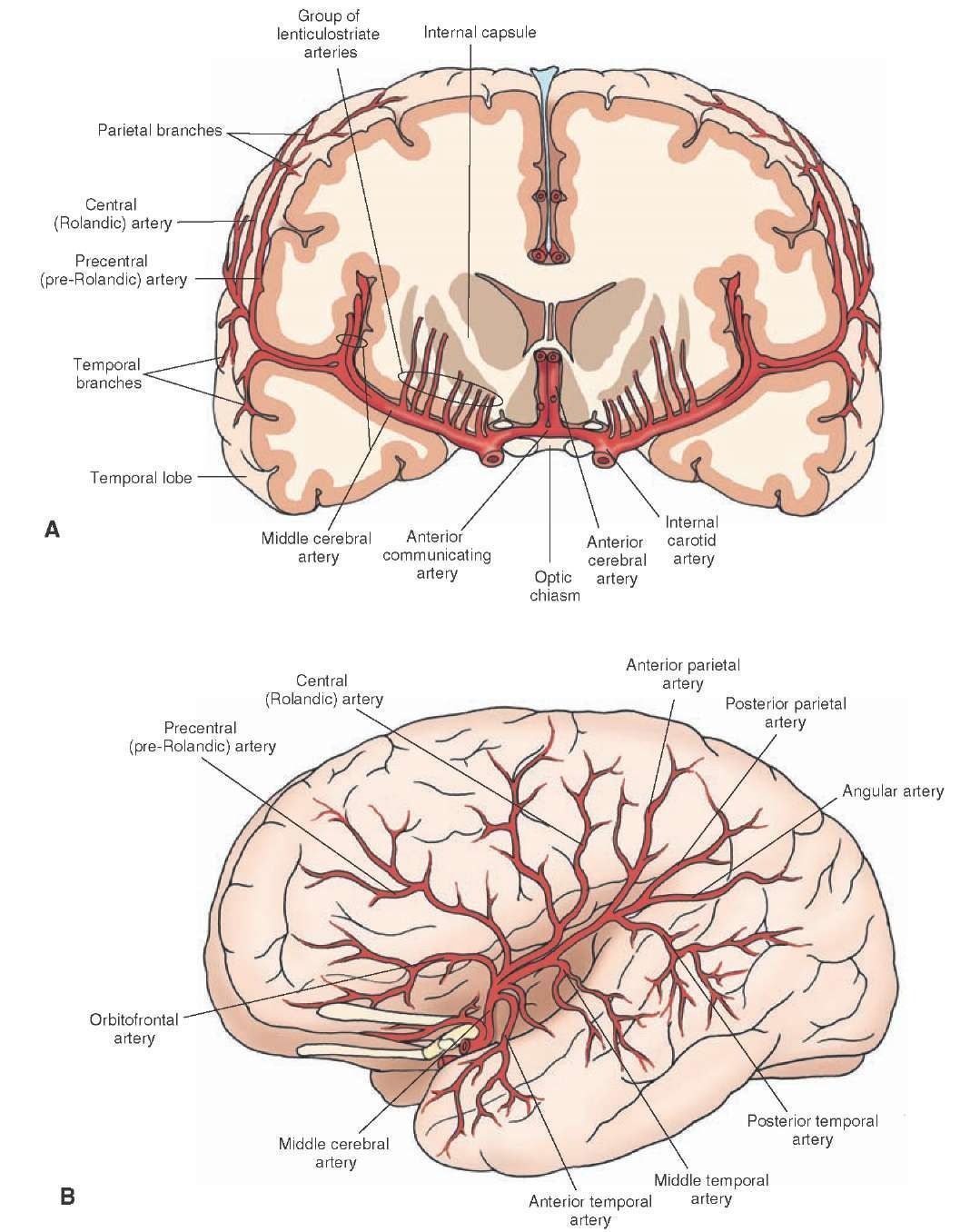
- middle cerebral artery
- External anatomy of brain
stem
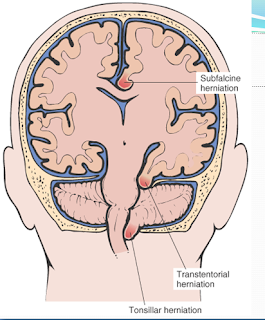
- Types of herniation
- Clinical presentation of TBI
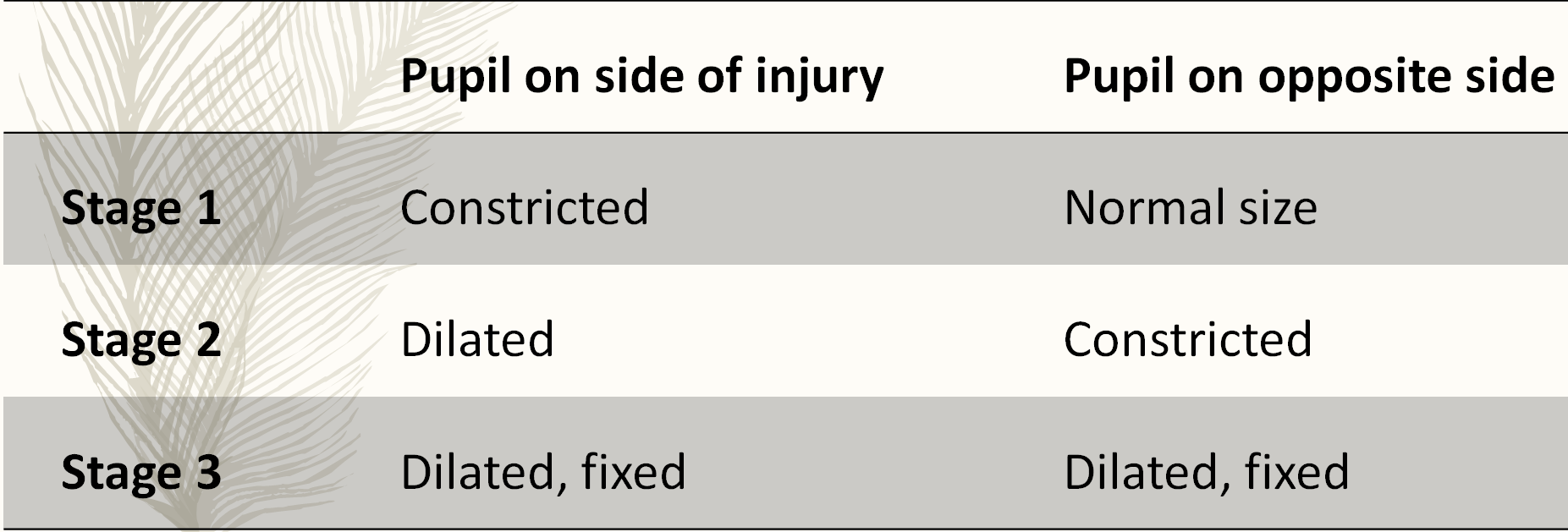
- Hutchinson’s pupil
- Hutchinson’s pupil
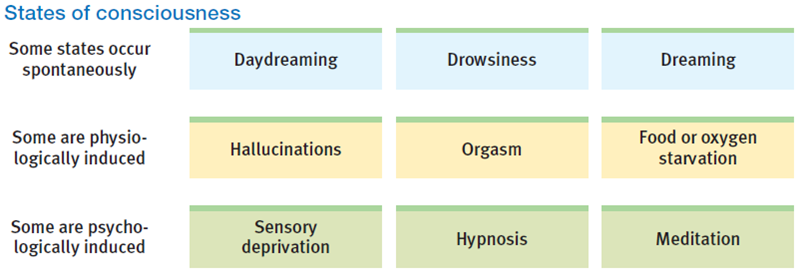
- Consciousness
- arises as the brain forms a
model of the world that
combines external stimulation
with internal experience.
- States
- Sleep cycle
- arises as the brain forms a
model of the world that
combines external stimulation
with internal experience.
- Glasgow Coma Scale
- Cushing Reflex
- Cushing reflex occurs in response to increase in the intracranial pressure.
- It is a triad of hypertension, bradycardia, and irregular breathing (Apnea).
- Cushing reflex indicates that brain herniation and death is imminent, so it is an emergency situation.
- Cushing reflex occurs in response to increase in the intracranial pressure.
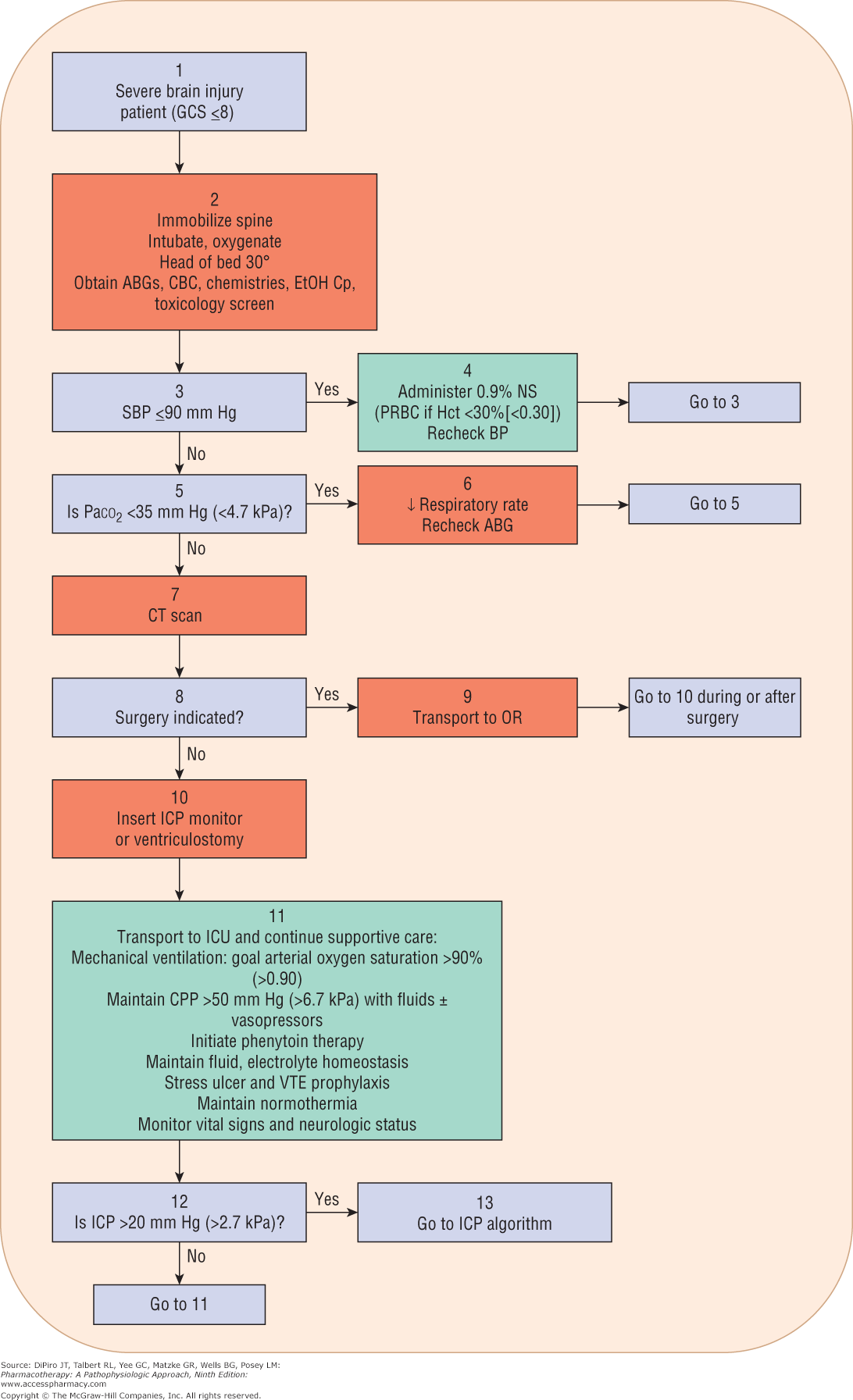
- Management of Traumatic Brain Injuries
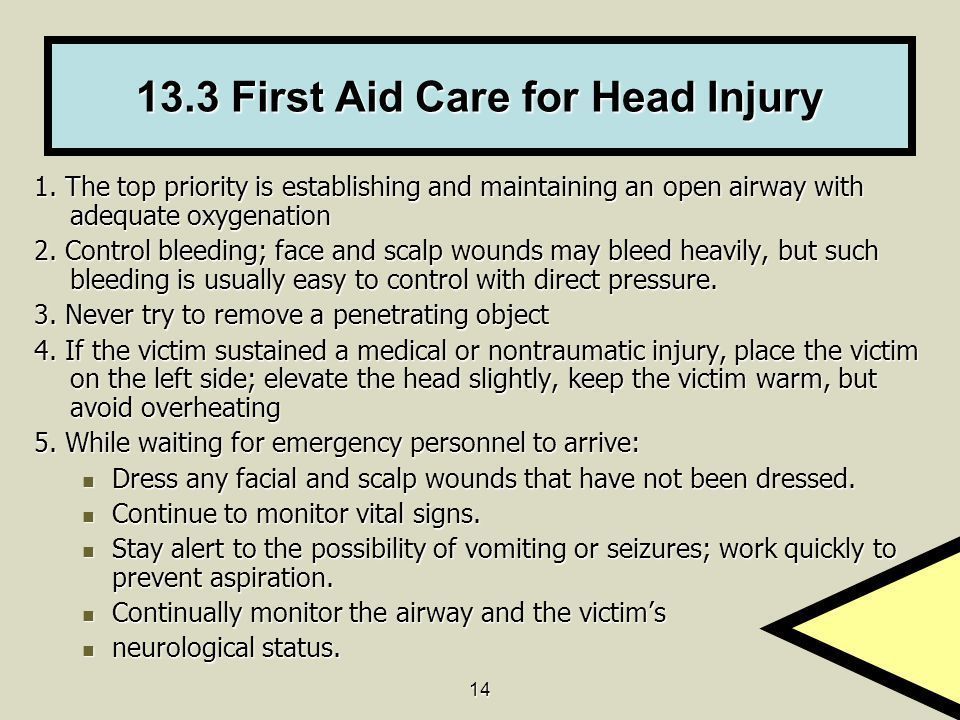
- First AID
- Algorithm for the acute
management of the TBI patient.
- Treatment of
Intercraial
hypertension
- Analgesics and sedatives
- Hyperventilation
- Hypothermia
- Osmotic agents
- Decompressive craniotomy
- Analgesics and sedatives
- Prophylaxis of
complications
- Antiseizure
- Decrease
incidence of
EARLY
seizures
(<7days)
- Phenytoin
- Decrease
incidence of
EARLY
seizures
(<7days)
- Deep venous
thrombosis
prophylaxis
- Antiseizure
- Burr hole Surgery
- Indications
- acute
subdural
hematoma
- chronic
subdural
hematoma
- brain cancer
- pus around
the
meninges
- Hydrocephalus
- acute
subdural
hematoma
- Complications
- Bleeding
Infection
Blood clots
Brain injury
Another
surgery
required
- Bleeding
Infection
Blood clots
Brain injury
Another
surgery
required
- Indications
- First AID
Media attachments
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Want to create your own Mind Maps for free with GoConqr? Learn more.