7287218
Physiology and Patient
Assessment
- Physiology
- 60% body weight is water
- 20% extracellular
- 5% intravascular
- Small amount of
circulating fluid c.f.
total volume
- Only a small volume we can control with fluids,
which in turn affects other fluid compartments
- Small amount of
circulating fluid c.f.
total volume
- 15% interstitial
- 5% intravascular
- 40% intracellular
- Higher in young and male animals,
lower in older and female animals
- Related to fat content
- Related to fat content
- 20% extracellular
- Electrolytes controlled by kidney
- Sodium and chloride main
extracellular ions
- Potassium main intracellular ion
- Also used glucose and urea to
control osmolality of fluid
- Sodium and chloride main
extracellular ions
- Osmotic pressure controlled by
large particles
- e.g. albumin
- Draw water into vessel
- e.g. albumin
- Hydrostatic pressure
- Physical pressure on vessel walls
- Push water out of vessel
- Physical pressure on vessel walls
- Water inputs
- Food
- Small amount from
metabolism
- Drinking water
- Water supply enough to cover normal losses
- 40-60ml/kg/24 hrs
- 40-60ml/kg/24 hrs
- Water supply enough to cover normal losses
- Food
- Water outputs
- Sensible
- Urine
- Faeces
- Urine
- Insensible
- Respiratory tract
- Skin evaporation
- Minimal in dogs and cats
- Greater in animals that sweat
- e.g. horses and cattle
- e.g. horses and cattle
- Minimal in dogs and cats
- Influenced by external
factors
- Respiratory tract
- Sensible
- Increased water
requirement
- Immature animals
- Lactation
- Pyrexia
- High ambient temperature
- Immature animals
- 60% body weight is water
- Patient Assessment
- Does the patient need fluid therapy?
- If so, are you treating hypoperfusion,
dehydration, hypovolaemia, or maintenance?
- Assess perfusion and hydration status
- Perfusion – to do with loss from circulation
- Hydration – to do with total loss from body
- Perfusion – to do with loss from circulation
- Assess perfusion and hydration status
- If so, are you treating hypoperfusion,
dehydration, hypovolaemia, or maintenance?
- Does the patient have inadequate
intake and/or excessive losses?
- What type of fluid has been lost?
- Choose a type of fluid
- Choose a route of
administration
- Calculate amounts and rates of
fluids
- Hypovolaemia
- Deficit in blood volume
- Can lead to hypoperfusion
(inadequate tissue blood flow)
- Can lead to hypoperfusion
(inadequate tissue blood flow)
- Reduced oxygen delivery to
tissues
- Failure to remove metabolic
waste products
- Causes
- Reduced cardiac output
- Maldistribution of blood
flow
- Reduced
volume
- Haemorrhage
- Fluid loss in excess of
intake
- Vomiting
- Diarrhoea
- Polyuria
- Vomiting
- Loss of plasma may be
internal
- Transduction
- Exudation to third
space
- Transduction
- Reduced cardiac output
- Deficit in blood volume
- Dehydration
- Reduction in water content of
body
- Often used to refer to combined
water and solute losses in excess of
intake
- Can lead to hypovolaemia
and hypoperfusion
- Reduction in water content of
body
- Calculating amount of fluid required -
consider continual losses
- Insensible losses
- Sensible losses
- Number of vomits per
day
- Volume of diarrhoea
- No amount of renal compensation
- No amount of renal compensation
- Insensible losses
- Does the patient need fluid therapy?
- Types of abnormal fluid loss
- Hypotonic
- e.g. cat shut in garage
- Loss of fluid (urine, sweat)
without replacing it
- e.g. cat shut in garage
- Isotonic
- e.g. haemorrhage
- First 6-8 hours of blood loss
- Little fluid movement to compensate
- Blood composition similar
- Total volume reduced
- Little fluid movement to compensate
- High impact on
blood pressure
- High heart rate
- High pulse
- Thready/no
peripheral
pulse
- Thready/no
peripheral
pulse
- High heart rate
- e.g. haemorrhage
- Hypertonic
- e.g. diarrhoea, vomit
- Loss of water, electrolytes/salts
- Lose more electrolytes than water
- NaCl
- Mg
- Effect on cardiac function
- NaCl
- Lose more electrolytes than water
- Retaining circulation is more
dilute (hypotonic)
- Water moves from circulation to
interstitial and intracellular spaces
- Oedema
- Oedema
- Greater impact on fluid loss than
interstitial loss
- Death can come quickly
- Very rapid loss of electrolytes
- Very rapid loss of electrolytes
- e.g. diarrhoea, vomit
- Hypotonic
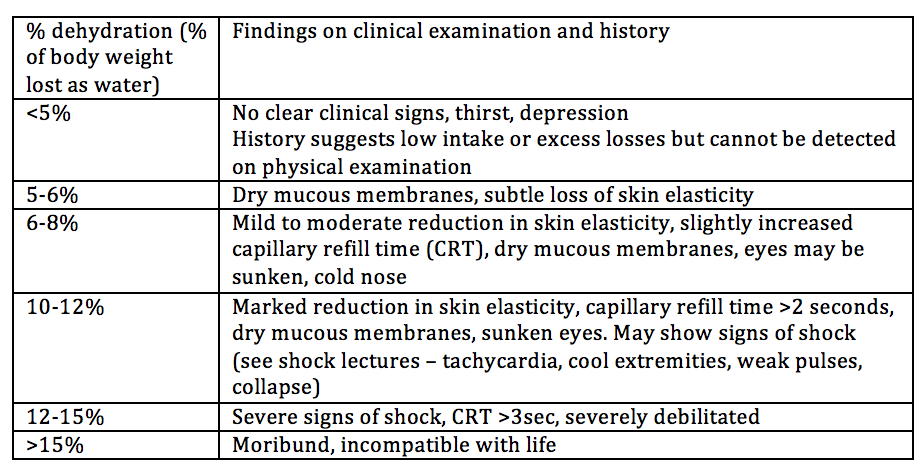
- Dehydration and hypovolaemia
- Hydration status
- Mucous membranes - moist?
- Skin turgor
- e.g. skin tenting
- Careful in older/emaciated animals
- Loss of skin elasticity
- Loss of skin elasticity
- e.g. skin tenting
- Retraction of the globe
- Most animals between 7-10%
- Likely to make little difference if it is
7.5 or 8.5
- Add on maintenance
- Administer over 24 hours
- Make sure signs are getting better
- Make sure signs are getting better
- Likely to make little difference if it is
7.5 or 8.5
- Mucous membranes - moist?
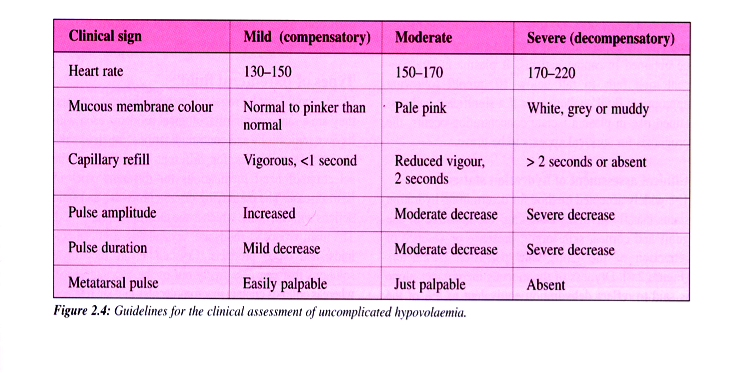
- Hypoperfusion
- Mucous membrane colour
- Capillary refill time
- Pulse quality
- Area under curve
- Area under curve
- HR and BP change more with
severe hypoperfusion
- Normal HR 60-120 depending on size of dog
- 160-200 cats
- Normal HR 60-120 depending on size of dog
- Difficult to differentiate hypovolaemia from other
causes of hypoperfusion from these signs
- Other tests may be useful
- Urine specific gravity, urine output
- Normal > 1.030 and 1-2 ml/kg/hr
- Normal > 1.030 and 1-2 ml/kg/hr
- Packed cell volume
- Increase if fluid loss not including cells
- Increase if fluid loss not including cells
- Body weight
- Urea
- Electrolytes
- Increase of pure water deficit,
may be deficits depending on
type of loss
- Increase of pure water deficit,
may be deficits depending on
type of loss
- Central venous pressure
- Useful to observe trends c.f. single result
- Urine specific gravity, urine output
- Other tests may be useful
- Mucous membrane colour
- Dehydration
- Dryness of mucous membranes
- Retraction of the globe
- Third eyelid comes across
- At this point, will tend to have
skin tenting
- At this point, will tend to have
skin tenting
- Dryness of mucous membranes
- Hydration status
- Clinical assessment and monitoring
- Monitor input and output
- Input
- IV fluids
- Bags used
- Volumes recorded on pumps
- Bags used
- Intake from drinking, wet food
- IV fluids
- Output
- Urine
- Vomit
- Dirrhoea
- Approx 20ml per 10cm puddle
- Approx 20ml per 10cm puddle
- Urine
- Aim for input slightly over output
- 10%
- Allow for respiratory and other
non-measurable losses
- If out>in, increase input/fluids
- If in is significantly greater than out,
decrease fluids and try to work out why
- 10%
- Input
- Volume depletion and overload
- Depletion
- Weak, rapid pulse
- Pale, dry/tacky mucous membranes
- Slow CRT
- Poor skin elasticity
- Cool extremities
- Sunken eyes
- Reduced urine output
- Radiographically small heart
- Weak, rapid pulse
- Overload
- Coughing
- Increased respiratory rate
- Oedema
- Ascites/pleural effusion
- Chosis
- Serous nasal discharge
- Exopthalmus
- increased urine output
- Vomiting
- Coughing
- Stop fluids if signs of overinfusion
- Depletion
- HR decreasing
- Pulse quality
improving
- Mucous membranes colour,
moistness, CRT
- Reduced skin
tenting
- Urine output
- 1ml/kg/hr indicates renal perfusion
may be inadequate
- 1-2 ml/kg/hr = normal
- >2ml/kg/hr = overinfusion
- 1ml/kg/hr indicates renal perfusion
may be inadequate
- Central venous pressure 1-5cm H2O
- Trends more important
- Trends more important
- PCV/ total protein
- Useful in serial measurements
- Care in anaemia, haemorrhage
- Useful in serial measurements
- Urine, creatinine, electrolytes
- Renal perfusion
- Renal perfusion
- Arterial blood pressure
- Systolic 100-120 mmHg
- Mean 80mmHg
- Less than 60mmHg - poor renal perfusion
- Less than 60mmHg - poor renal perfusion
- Systolic 100-120 mmHg
- When heart rate, blood pressure, pulses,
CRT etc are normal
- Maintenance phase fluid required
- Once electrolytes normal, the parient is eating, drinking, with
normal gastrointestinal and urinary function
- Stop fluids and return to normal intake
- Stop fluids and return to normal intake
- Monitor input and output
- Aims of fluid therapy
- Restore circulating blood
volume
- Replace
pre-existing
losses
- Allow for ongoing abnormal losses
- Aim to replace like for like
- Decide on type of fluid
- Decide on type of fluid
- Supply normal maintenance
requirements
- Restore circulating blood
volume
Media attachments
{kind=link}
{kind=link}
Want to create your own Mind Maps for free with GoConqr? Learn more.