Description
|
|
Created by Sara Wagner
about 9 years ago
|
|
Page 1
{kind=link}
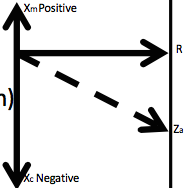
The picture above shows the vectors for the components of impedance (Z). Resistance (R) is in phase of velocity (direction of motion). This makes sense because R represents the dissipation of energy into heat as it enters the system, and the faster something is going, the more heat it generates. Mass reactance (Xm) leads resistance by 90 degrees. Since it LEADS, it is POSITIVE. Stiffness, or compliant reactance (Xc) , lags resistance by 90 degrees. Since it LAGS, it is NEGATIVE. Putting that together, Xc lags Xm by 180 degrees.
Page 2
Stiffness elements in the ear Ligaments Tendons Tympanic membrane The air enclosed in the canal and middle ear space Mass elements in the ear Pars flaccida of the tympanic membrane Ossicles Perilymph in the cochlea Mesenchyme (unsolved fetal tissue, amniotic fluid, debris in the ME or OE) clinging to the ossicles in infants Friction (resistance) elements in the ear Tympanic membrane Tendons and ligaments The narrow passage b/w the ME cavity and the mastoid The viscosity of the perilymph and the mucus lining of the ME cavity
{kind=link}
Page 4
{kind=link}
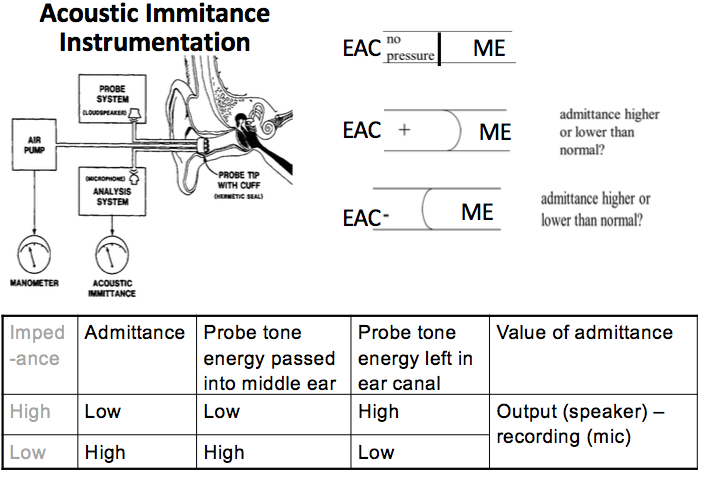
A calibrated probe tone stimulus is presented to the outer ear canal with a microphone. Air pressure in the ear canal is varied above and below atmospheric pressure. As the air pressure is increased or decreased in the ear canal, the admittance flowing into the middle ear is decreased, so more sound pressure remains in the ear canal. At the microphone, this is read as an increase in probe sound pressure level. When we do immittance testing, we put pressure into the canal and manually push the tympanic membrane inward. Then we "pull" pressure out of the canal and manually pull the tympanic membrane outward. As you push and pull the TM, you are tightening the entire ossicular chain. This tightening increase impedance and decreases admittance, so less sound is able to get through to the middle ear space as compared to having no pressure at all. What we are measuring is the amount of energy left in the ear canal. There is an air pump that changes the pressure in the canal and a microphone that records what is "leftover" in the canal. The difference between the incident sound and what is left in the canal is a measure of admittance.
Page 5
{kind=link}
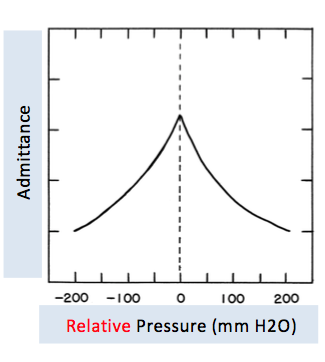
What this picture is showing is a graph of the notes on the previous page. The peak shows that admittance is highest when there is no pressure being put in or taken out of the canal. As the pressure decreases from -200 to 0, admittance slowly increases to its peak; as the pressure increases from 0 to 200, admittance slowly decreases. The pressure is relative to atmospheric pressure
Page 6
Equivalent Ear Canal VolumeThe purpose of tympanometry is to measure the middle-ear admittance under varying ear canal air pressureHowever, admittance measured at the probe tip reflects the COMBINED admittance of the external auditory canal and and the admittance of the ME.Accuracy of the ME admittance relies on obtaining an accurate estimate of the "equivalent" ear canal volume. If the admittance of the ear canal can be measured independently of the admittance of the ME, then just the admittance of the tympanic membrane can be measured.Ear canal volume is compensated using a baseline method by subtracting out the admittance at either the positive or negative "tail" of the tympanogramMost clinical immittance units provide a baseline correction feature when measuring tympanometry. It subtracts the equivalent ear canal volume so that the tympanogram is plotted with admittance starting at 0 mmho.Baseline compensation may be done either at an extreme positive value, usually +200 daPa, or an extreme negative value, such as -400 daPa. At these values, it is assumed that the middle ear is stiff enough to cause its admittance to be 0, so the admittance measured at the probe tip is just from the ear canal. So at these pressures, 1 cubic centimeter of trapped air = the acoustic admittance of 1 mmho. -Basically, the admittance at an extreme positive value (like +200 daPa) or an extreme negative value (-400 daPa) is just the admittance of the ear canal and so that value is the ECV and is then subtracted out to give you just the admittance of the ME Clinical measurements of ear canal admittance (volume) are most commonly taken from the admittance positive tail with a 226-Hz probe tone, which overestimates ECV by 40%
Page 7
Peak-Compensated Static Acoustic AdmittanceStatic admittance is the most often measured feature of the 226-Hz tympanogram and is commonly referred to as "compliance." The peak of the tympanogram after subtracting ECV is called the "peak-compensated static acoustic admittance," or more commonly static admittance (Ytm)Ytm is derived through the formula Ypeak - Y+400 for the positive tail method or Ypeak - Y-400 for the negative tail method. Measurement of static admittance can be affected by different procedural variables. The compensated static admittance is typically higher when extreme negative (rather than extreme positive) pressure is used to estimate ear canal volume because of tympanometric asymmetry Faster pump speeds produce higher static admittance Decreasing the pressure from positive to negative produces lower static admittance
Page 8
Tympanometric Gradient and WidthBoth measures provide an index of the shape of the tympanogram in the vicinity of the peak and quantify the relative sharpness or roundness of the peakThe presence of MEE decreases the gradient and increases the width of the tympanogram TW is measured by drawing a horizontal line halfway between the peak admittance and the baseline. The intersection of the line with either side of the tympanogram is the width, measured in daPa; a small TW results when the tympanogram has a sharp peakTympanometric gradient is a ratio measure of the steepness of the slopes on either side of the peak. Done by calculating the difference in admittance at the peak and the average of admittance at ± 50 daPa. A line is drawn at this admittance and then the value is divided by the peak height of either the positive or negative tail.
Page 9
Tympanometric Peak Pressure With ET dysfunction, the most effective operating point of the ME is near the pressure contained within the ME Ytm reaches its highest value when the pressures on both sides of the TM are equal, TPP is an indicator, but not a direct measure, of the pressure in the ME space Measuring TPP can detect the presence of negative or positive ME pressure because of ET dysfunction. Positive pressure may occur in the early stages of AOM As the infection progresses, the ET is blocked and the fluid cannot naturally drain out of the ear into the throat, thus a negative TPP develops. As the MEE increases and thickens, the tympanogram flattens and widens into a type B pattern
Page 10
Tympanogram ShapesA: TPP: ± 150 daPa; static admittance: 0.3-1.7 mmhoAs: TPP: ± 150 daPa; low static admittance: < 0.2 - 0.3 mmho Indicative of a stiff ME otosclerosis (but not a good diagnostic sign). Why is it indicative? Because a low admittance (compliance) means the TM is not moving very much. Ad: TPP: ± 150 daPa; high static admittance ( > 1.7 mmho)TM is more flaccid than normal; monomeric (thin) TM or an ossicular chain discontinuity B: Flat with no identifiable peak Low ECV: Otitis media High ECV: TM perforations or PE tubes - measuring ear canal and ME volumes Extremely low ECV: Clogged probe tip or probe up against ear canal wall C: TPP < -150 daPa; static admittance is sometimes within normal limitsTympanogram NormsAdult:ECV: 0.9-2.0 mLTPP: ±150 daPACompliance (static admittance): 0.3-1.7 cm3 Children:ECV: 0.4-1.0 mLTPP: ± 150 daPACompliance (static admittance): 0.2-0.9 cm3
Want to create your own Notes for free with GoConqr? Learn more.