12862503
Descrição

FlashCards por Taylor Carre-Riddell, atualizado more than 1 year ago
|
|
Criado por Taylor Carre-Riddell
quase 7 anos atrás
|
|
| Questão | Responda |
| Separation Anxiety Disorder | Developmentally inappropriate and excessive fear or anxiety concerning separation from attachment figure. |
| What is the link between Childhood Separation anxiety disorder and Panic Attacks? | Both disorders are associated with heightened sensitivity to inhaled CO(2) and can be influenced by childhood parental loss |
| What is panic? | an abrupt experience of intense fear or acute discomfort, |
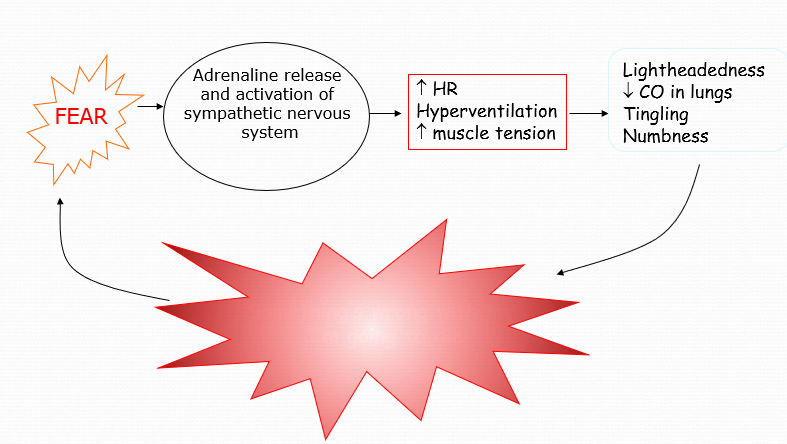
| What is the Biology of panic? |
Image:
Image (binary/octet-stream)
|
| Risk factors for panic? | Genetics; An abnormally sensitive fear network; Major life stressors; A history of sexual or physical abuse in childhood; |
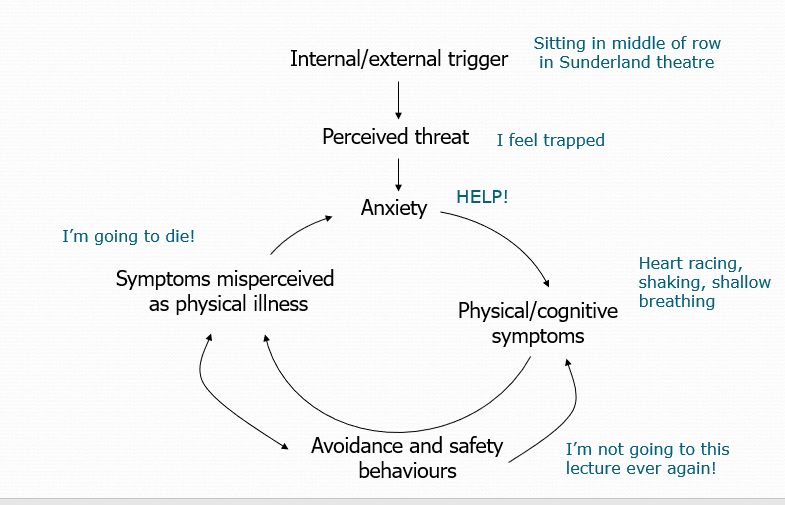
| Cognitive model of panic? |
Panic Attacks result from ‘catastrophic misinterpretation’ of bodily or mental events;
Events misinterpreted as signs of impending disaster- i.e. a heart attack or going crazy;
A vicious cycle of events is triggered- associated with rising levels of anxiety and panic.
Image:
Image (binary/octet-stream)
|
| Panic attacks- subtypes? | Situationally-bound/cued; Unexpected/uncued; Situationally predisposed |
| Anxiety versus fear | ANXIETY -anxious apprehension and worry that is a more general reaction that is out of proportion to threats in environment -future oriented -can be adaptive if not excessive FEAR -Experienced when a person is faced with real and immediate danger. -Present-oriented -Can be adaptive |
| Specific Phobias DSM - 5 | Irrational fear of a specific object or situation; Markedly interferes with individual’s ability to function; Individual recognises fear is excessive or unreasonable; Exposure to phobic stimulus results in anxiety response; Phobic situation is avoided or endured with intense anxiety/distress; Typically lasting 6 months or more. |
| Specific phobia: DSM subtypes | Environments – heights, water, storms Situations- aeroplanes, elevators, enclosed places; Animal- spider, cat Blood, injections, injuries Other- vomiting, choking, illnesses, people in costumes |
| Specific phobia- aetiology | Psychodynamic theory Stems from Freud’s case study of Little Hans ("Analysis of a Phobia in a Five-year-old Boy“ 1909); Castration anxiety and Oedipus complex; Freud theorized that phobias were actually displaced fears or conflicts Conditioning theory of fear acquisition Watson & Little Albert Individual learns to associate a threatening stimulus with a non-threatening stimulus so that the latter by itself can trigger anxiety Fear is then maintained by avoidance- individual does not get the chance for ‘reality testing’ and new learning Problem: Many phobias have no obvious environmental cause- direct or indirect. “She has always been fearful of cats” Why are some phobias more common than others, even though few encounters with the feared object (i.e. snakes) Social learning Fear may be learnt via observation of trauma in others; Fear may be learnt by hearing of experiences of others; Fear may be modeled or ‘instructed’ Evolutionary perspective Ohman and Mineka (2001)- organisms which learned to fear environmental threats faster had a survival and reproductive advantage |
| Social Anxiety Disorder | Marked fear about 1 or more social situations Individual fears that they will act in a way or show anxiety symptoms that will be negatively evaluated Social situations almost always provoke fear or anxiety Social situations are avoided or endured with intense fear or anxiety. |
| Social Anxiety Disorder -Risk factors | Individual factors Genetics- specific or general heritability of emotional disorders? Cognitive factors- negative appraisal of social interactions- stem from adverse social interaction? Social skills deficits- “chicken or egg”? Temperament- shyness |
| What is Agoraphobia? | Marked fear or anxiety 2 or more of : using public transport, being in open spaces, being in enclosed places, standing in line or being in a crowd, being outside of the home alone. Fears that escape might be difficult or help unavailable |
| Overview of treatment for anxiety disorders | Medication Psychological treatment- esp Cognitive behavioural therapy The importance of exposure Other ABC Cross-sectional formulation of problem; Assists in describing CBT model to patient |
| ABC | Time-limited, problem focused approach based on the cognitive model; Relies on collaborative empiricism: scientist-practitioner model; Continuous measurement and evaluation of patient problems- used to test hypotheses concerning problem maintenance and to assess treatment efficacy; Homework- integral part of treatment; Socratic dialogue – important technique to enable transfer of information, and collaborative and supportive environment. Dearousal techniques Slow breathing Progressive muscle relaxation Meditation Mental grounding Exposure Imaginal Real Graded |
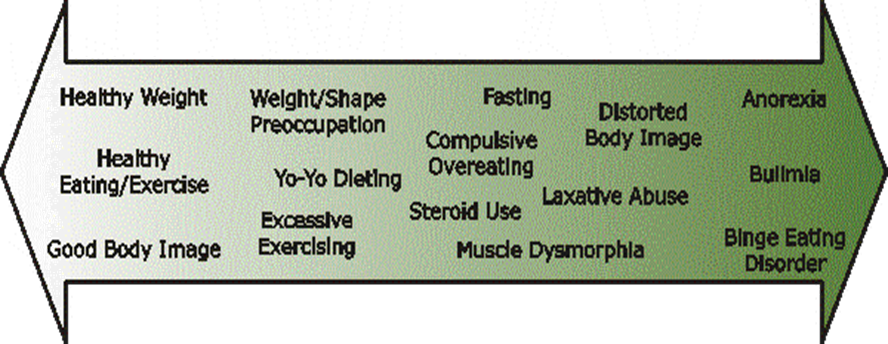
| Describe the continuum of healthy eating, disordered eating, and eating disorders |
Image:
Image (binary/octet-stream)
|
| Anorexia Nervosa (AN) | Mean age at onset is in the teens early twenties More recently late onset cases are being seen (Bueno et al., 2013) Comorbidity: 60% depression & 33% anxiety disorders (Puccio et al., 2017) Course and outcome are highly variable (Steinhausen, 2009) recover after a single episode fluctuation pattern of weight gain followed by relapse chronic deteriorating course of the illness over many years |
| Anorexia Nervosa Disordered Eating can involve: | Food rituals Cuts food in small pieces Rearranges food on plate Eliminates foods gradually 300-600 calories a day Diet pop, sugarless gum Preoccupation with food Cooks for others Hungry, but refuses to eat |
| Anorexia Nervosa Psychological Features | Perfectionism Harm avoidance Feelings of ineffectiveness Inflexible thinking Overly restrained emotional expression |
| Bulimia Nervosa | Generally occurs later than AN, late-early adulthood Frequently begins during or after an episode of dieting Course may be chronic or intermittent For a high percentage the disorder persists for at least several years Periods of remission often alternate with recurrences of binge eating Purging may become an addiction High levels of comorbidity with MDD and anxiety disorders |
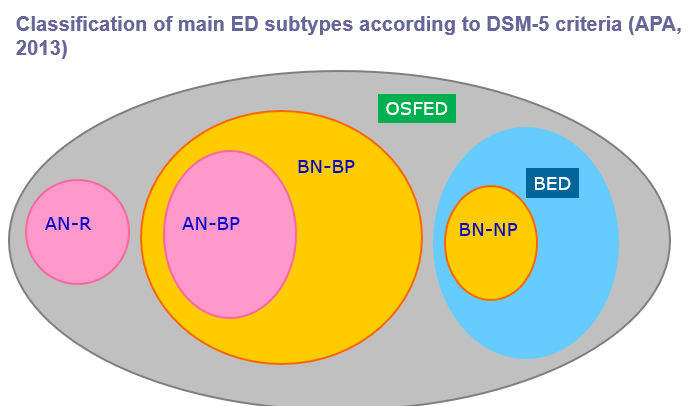
| Binge Eating Disorder (BED) | Recurrent episodes of binge eating (once/week X 3 months) 3 or more of: eating more rapidly than normal, eating until uncomfortably full, eating large, amount of food when not hungry, eating alone because of embarrassment or disgust, depressed or guilty after overeating Marked distress regarding binge eating Not associated with regular use of inappropriate compensatory behaviours |
| OSFED | Atypical Anorexia Nervosa: All criteria are met, except despite significant weight loss, the individual’s weight is within or above the normal range. Binge Eating Disorder: (of low frequency and/or limited duration): All of the criteria for BED are met, except at a lower frequency and/or for less than three months. Bulimia Nervosa: (of low frequency and/or limited duration): All of the criteria for BN are met, except that the binge eating and inappropriate compensatory behaviour occurs at a lower frequency and/or for less than three months. Purging Disorder: Recurrent purging behaviour to influence weight or shape in the absence of binge eating Night Eating Syndrome: Recurrent episodes of night eating. Eating after awakening from sleep, or by excessive food consumption after the evening meal. |
| Unspecified Feeding and Eating Disorder | behaviours causing clinically significant distress/impairment of functioning, but do not meet the full criteria of any of the Feeding or Eating Disorder criteria. |
| PICA | Persistent eating of non-nutritive substances for a period of at least 1 month The eating of non-nutritive substances is inappropriate to the developmental level of the individual |
| Rumination Disorder | Repeated regurgitation of food for a period of at least one month Regurgitated food may be re-chewed, re-swallowed, or spit out. The repeated regurgitation is not due to a medication condition (e.g. gastrointestinal condition). The behaviour does not occur exclusively in the course of AN, BN, BED, or ARFID. |
| Avoidant/Restrictive Food Intake Disorder (ARFID) | An Eating or Feeding disturbance as manifested by persistent failure to meet appropriate nutritional and/or energy needs associated with one (or more) of the following: Significant loss of weight (or failure to achieve expected weight gain or faltering growth in children) Significant nutritional deficiency |
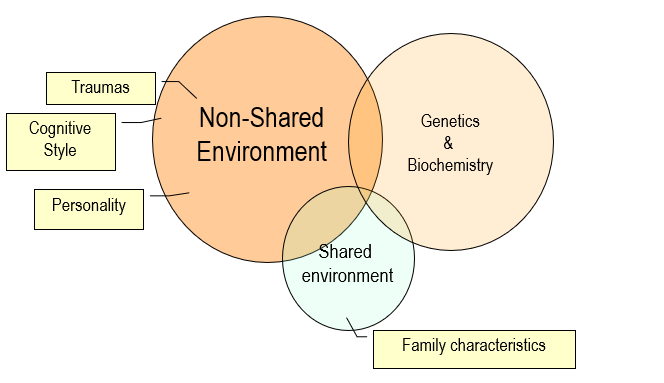
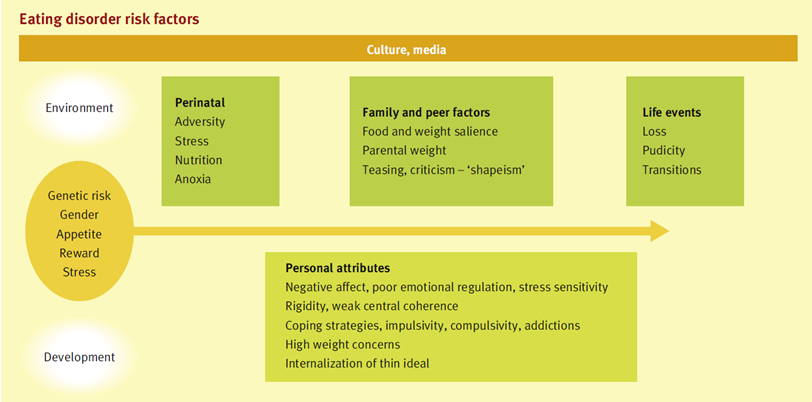
| Risk factors for Eating Disorders |
Image:
Image (binary/octet-stream)
|
| Classification of EDs |
Image:
Image (binary/octet-stream)
|
| Summary Twin Studies in EDs | Twin studies show heritability of 50-60% for broadly defined AN Heritability for BN ~ 58 - 83% Heritability for BED ~ 82% Heritability for obesity in teenagers ~ 86% |
| Further Biological Factors in EDs | Chemical imbalances in the neuroendocrine system imbalances control hunger, appetite, digestion, sexual function, emotions, and thinking etc. Serotonin & norepinephrine in acutely ill AN and BN patients representing a link between depression & EDs or a result of starvation?????? Excessive levels of cortisol in both AN & depression caused by a problem that occurs in or near the hypothalamus Brain Structures Parietal cortex is overestimate their own weight, lack insight about it, but could be caused by starvation |
| EDs and cognition | General intellectual ability- average to high average AN individuals whilst acutely unwell: Mild cog deficits in executive functioning, memory, verbal and visuospatial processing- not in recovered patients Deficits in cognitive flexibility & central coherence seen in BN and AN Cognitive Remediation Therapy |
| Personality in Anorexia | AN-R: obsessional, perfectionistic, socially inhibited, harm avoidance and emotionally restrained AN-BP: impulsive & extroverted personality style, more like BN |
| Personality in Bulimia | Impulsive, interpersonally sensitive, low self-esteem Elevated rates of DSM Cluster B and Cluster C personality disorders especially BPD |
| BN Environmental Factors: Interpersonal & Social | Interpersonal Factors troubled family and personal relationships difficulty expressing emotions and feelings history of being teased or ridiculed based on size or weight High parental expectations & maladaptive parenting (cause and effect ????) Childhood feeding difficulties History of trauma, sexual, physical and/or mental abuse |
| BN Environmental Factors: Cultural Factors | Social Factors (media and cultural pressures) Cultural pressures that glorify "thinness" & place value on obtaining the "perfect body” Narrow definitions of beauty only women & men of specific body weights and shapes Cultural norms: value people on the basis of physical appearance NOT inner qualities & strengths People pursing professions or activities that emphasize thinness are more susceptible i.e. Modeling, dancing, gymnastics, wresting, long distance running |
| Specific ED risk factors for males | Dieting is a less common risk factor for men Men whose job requires a particular body “look” such as models, actors or entertainers Male athletes are at a higher risk of developing an ED (e.g. gymnasts, swimmers, jockeys, weightlifters, wrestlers and body builders as restrictive dieting, extreme exercise regimes and/or anabolic steroid abuse. Present with more premorbid obesity and overweight. |
| Further environmental factors |
Image:
Image (binary/octet-stream)
|
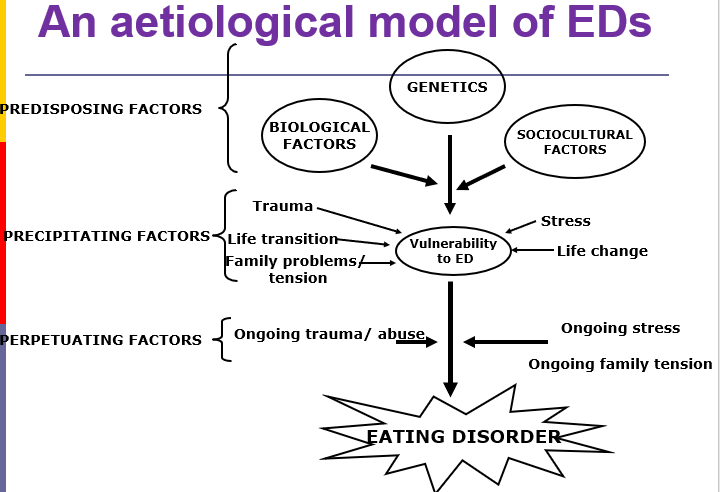
| An aetiological model of EDs |
Garner and Garfinkel (1997)
Predisposing: contribute towards a vulnerability towards EDs
Precipitating:(stressors) lead to weight loss and the gains associated with weight loss are discovered
Perpetuating: maintain weight loss, trapping the individual into an inescapable situation
Image:
Image (binary/octet-stream)
|
| Obsessive-compulsive disorder is... | Obsessions and compulsions are recurrent and persistent; Individual recognises they are excessive or unreasonable; Obsessions/compulsions cause marked distress, are time consuming (>1 hr/day) and significantly interfere with functioning and relationships. Persistent ideas, thoughts, impulses, or images that are experienced as intrusive and inappropriate and cause marked anxiety or distress; |
| Risk Factors | • Family history with evidence of dominant or codominant mode of transmission (Jenike, 2004); • Early childhood experiences and critical learning incidents maladaptive beliefs about responsibility and threat (Clark & O’Connor ,2005); • Personality factors- neuroticism, psychoticism and sensitivity to punishment (Fullana et al., 2004). |
| Obsessions: Common types | • Fears of contamination • Repeated doubts (safety, scruples) • Need to have things in a particular order • Sexual, horrific or blasphemous imagery • Aggressive or inappropriate impulses • Nonsensical thoughts or images |
| Compulsions are | • Repetitive behaviour (handwashing, checking) or mental acts (praying, counting, repeating words silently) the goal of which is to prevent or reduce anxiety; • Can include rigid/stereotyped acts according to elaborate rules without any real explanation of them. |
| OCD Cognitive Factors | • Intrusive thoughts might become obsessions if they are evaluated as: o Overly important (‘if I’m thinking this way, it must be important’); o Highly threatening (‘if I continue to think like this, something bad will happen’); o Requiring complete control (‘I’ve got to stop thinking this way’); o Necessitating a high degree of certainty (‘I need to be certain that nothing bad will happen’) o Associated with a state of perfection (‘I can’t stop thinking about this until I do it perfectly’) |
| Cognitive Behavioural Model | 1. Begins with the premise that intrusive thoughts are normal 2. However, certain individuals place meaning on these thoughts, and thus respond to them in some way (avoid, suppress, ritualise etc). 3. These responses increase vigilance for the intrusive thoughts and protects the meaning of the intrusion. |
| Body Dysmorphic Disorder | . Preoccupation with one or more perceived defects or flaws in physical appearance that are not observable or appear slight to others. A. At some point during the course of the disorder, the individual has performed repetitive behaviors (e.g., mirror checking, excessive grooming, skin picking, reassurance seeking) or mental acts (e.g., comparing his or her appearance with that of others) in response to the appearance concerns. B. The preoccupation causes clinically significant distress or impairment in social, occupational, or other important areas of functioning. • Specify if:With muscle dysmorphia: The individual is preoccupied with the idea that his or her body build is too small or insufficiently muscular. This specifier is used even if the individual is preoccupied with other body areas, which is often the case. |
| Impact on functioning | Impact on functioning • Can range from moderate (e.g., avoidance of some social situations) to extreme and incapacitating (e.g., being completely housebound); o job, academic, or role functioning (e.g., as a parent or caregiver), which is often severe (e.g., performing poorly, missing school or work, not working) o social functioning (e.g., social activities, relationships, intimacy), • psychiatric hospitalisation |
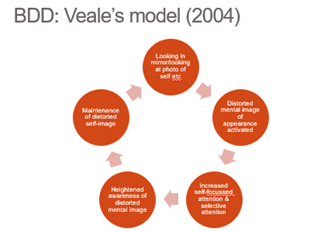
| BDD Veale's model |
Image:
Image (binary/octet-stream)
|
| Cognitive processes of BDD | • Compared to healthy controls individuals with BDD: o Evaluate appearance more negatively o Endorse assumptions about appearance such as “If my appearance is defective then I am worthless” o Overvalue physical appearance and attractiveness o Experience more anxiety and discomfort after mirror gazing o Experience more distress and self-focussed attention after mirror gazing o Engage in ruminative thinking- such as ‘Why am I so ugly’ o Engage in repeated reviews of past-appearance related experiences |
| Hoarding Disorder is | A Persistent difficulty discarding or parting with possessions, regardless of their actual value. B This difficulty is due to a perceived need to save the items and to distress associated with discarding them. C The difficulty discarding possessions results in the accumulation of possessions that congest and clutter active living areas and substantially compromises their intended use. If living areas are uncluttered, it is only because of the interventions of third parties (e.g., family members, cleaners, authorities). D The hoarding causes clinically significant distress or impairment in social, occupational, or other important areas of functioning (including maintaining a safe environment for self and others). |
| Cognitive factors associated with Hoarding Behaviour | • Control over possessions • Concern about memory • Responsibility over possessions; (After age, mood (depression and anxiety), OCD symptoms and other OCD-related cognitive variables controlled for) |
| Trichotillomania (hair pulling) is | Trichotillomania (hair pulling) A. Recurrent pulling out of one’s hair, resulting in hair loss. B. Repeated attempts to decrease or stop hair pulling. C. The hair pulling causes clinically significant distress or impairment in social, occupational, or other important areas of functioning. D. The hair pulling or hair loss is not attributable to another medical condition (e.g., a dermatological condition). |
| Functional consequences of Trichotillomania | Functional consequences • Social/occupational impairment • musculoskeletal injury (e.g., carpal tunnel syndrome; back, shoulder and neck pain), • blepharitis, • dental damage (e.g., worn or broken teeth due to hair biting). • Swallowing of hair (trichophagia) may lead to trichobezoars, with subsequent anemia, abdominal pain, hematemesis, nausea and vomiting, bowel obstruction, and even perforation (taken from DSM5) |
| Excoriation (skin-picking) disorder is | • Recurrent skin picking resulting in skin lesions. • Repeated attempts to decrease or stop skin picking. • The skin picking causes clinically significant distress or impairment in social, occupational, or other important areas of functioning. • The skin picking is not attributable to the physiological effects of a substance (e.g., cocaine) or another medical condition (e.g., scabies). • The skin picking is not better explained by symptoms of another mental disorder (e.g., delusions or tactile hallucinations in a psychotic disorder, attempts to improve a perceived defect or flaw in appearance in body dysmorphic disorder, stereotypies in stereotypic movement disorder, or intention to harm oneself in nonsuicidal self-injury). |
| Functional consequences of Excoriation (skin-picking) disorder | • Functional consequences Social and occupational impairment tissue damage, scarring, infection frequently requires antibiotic treatment for infection, and on occasion it may require surgery |
| Trichotillomania and Excoriation: Psychological aspects | • Motivated by stimulation of positive mood or feelings (i.e., pleasure, gratification or relief) or regulation of states of high or low arousal (i.e., anxiety or boredom); • Approximately 1/5- 1/3 people with SPD or trich report being in a trance/feeling mesmerized/ experiencing depersonalisation while picking/ hair pulling; • Substantial proportion of sufferers in both groups report little or no reflective awareness of the act as it occurs • Two subtypes proposed • “automatic pulling/picking” that occurs out of reflective awareness in sedentary situations; • “focused pulling/picking”, happens in full awareness in response to urges or negative affective states. |
| Trichotillomania and Excoriation: Psychological Consequences | • Shame, distress, embarrassment; • BUT • Hair pulling and scratching also reduce unpleasant emotions |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Quer criar seus próprios Flashcards gratuitos com GoConqr? Saiba mais.