15754889
Descrição
FlashCards por Heather Edmonson, atualizado more than 1 year ago
|
|
Criado por Heather Edmonson
aproximadamente 6 anos atrás
|
|
| Questão | Responda |
| What degree of mitral regurgitation should be considered when systolic flow reversal is noted in the pulmonary veins? | Severe |
| Which of the following statements are TRUE regarding patients with coarctation of the aorta? A. Lower extremity blood pressures are usually increased as compared to the arm blood pressure B. Lower extremity blood pressures are usually decreased as compared to the arm blood pressure. C. The arm blood pressure should be obtained from the patient's right arm. D. The arm blood pressure should be obtained from the patient's left arm. E. B, C F. A, D | E. B, C The right arm pressure should be used since the left arm blood pressure may be affected by the location of the coarctation |
| Which of the following is a finding of patients with mitral stenosis? A. Flattening of the E-F slope in M-mode B. "Hockey stick" appearance of the anterior mitral valve leaflet in 2D C. "Candle-flame" appearance across the valve in color Doppler D. All of the above are findings | D. All of the above are findings |
| Cardiac output/body surface area is the calculation for ______? | Cardiac index |
| Where is the most common site for calcifications of the mitral valve annulus to form? | The posterior aspect of the annulus |
| What affect can mitral regurgitation have on the E/A ratio obtained during a Doppler examination? | Mitral regurgitation can increase the E/A ratio. High filling pressures and volume overload also increase E/A ratios. |
| Which of the following statements is true regarding exercise echocardiography? A. Exercise echocardiography may be performed after treadmill B. Exercise echocardiography may be performed during supine bicycle exercise C. Exercise echocardiography may be performed during upright bicycle exercise D. Exercise echocardiography should not be performed using bicycle exercise E. A, B, C F. A and D | E. A, B, and C |
| When performing exercise echocardiography, the imaging is most accurate when it is obtained within the first? A. 5 minutes B. 3 minutes C. 4 minutes D. 1 minute | D. 1 minute |
| Which two echocardiographic findings are associated with a right ventricular volume overload (RVVO) pattern? | RVVO is right ventricular dilation with paradoxical septal motion. |
| A parabolic flow profile can be described as? | When fluid moves through a tube the fluid layers in the center of the tube have higher velocities than the fluid along the walls. |
| What is the normal resting cardiac output? | Normal range is 4-8 L/min. Typical value is usually 5 L/min. |
| What artery perfused the interventricular septum and the apex of the heart? | The left anterior descending coronary artery. The left anterior descending coronary artery is a branch off of the left main coronary artery. |
| Which two valvular diseases will present with a right ventricular volume overload (RVVO) pattern? | Tricuspid regurgitation and pulmonic regurgitation |
| The sinus venous, cardiac loop, and the aortic and brachial arches are portions of the? | Primitive heart tube |
| What nerve supplies the fibers for the SA node and control the heart rate? | Right vagus nerve |
| The left and right bundle branches divide and sub-divide into the ______? | Purkinje fibers. The purkinje fibers are atypical muscle fibers that lie beneath the endocardium. |
| All of the following statements regarding cardiac myxomas are true except ______? A. Patients may present with symptoms of chest pain B. Patients may present with symptoms of weakness or fatigue C. Patients may have an embolism(s) D. The most common location for a myxoma is in the left ventricle | D. The most common location for a myxoma is in the left atrium |
| How many vessels drain into the right atrium? | Three 1. Superior vena cava 2. Inferior vena cava 3. Coronary sinus |
| The principle of the conservation of mass forms the basis for what equation? | Continuity equation |
| What is the characteristic triad of findings that the clinical diagnosis of pericarditis is made from ______? | 1. Chest pain 2. Electrocardiographic changes 3. Presence of a pericardial rub on auscultation |
| What are the 4 main categories of etiologies of pericarditis? | 1. Infectious - this includes viral, bacterial, mycobacteria, fungal, and protozoal causes 2. Immune-inflammatory - this includes connective tissue diseases, arthritis, post MI, and drug induced causes 3. Neoplastic - this included primary and secondary cancers 4. Intracardiac-pericardial communications - this included trauma, ruptures, and post procedure/device complications |
| What is the most common primary valvular tumor of the heart? | Papillary fibroelastoma |
| When evaluating a patient with a large pericardial effusion and suspected cardiac tamponade, inferior vena cava plethora is an indication of? A. Elevated left atrial pressure B. Elevated left ventricular pressure C. Elevated right atrial pressure D. Normal pressures in the cardiac chambers | C. Elevated right atrial pressure |
| Which pathology is associated with the "dumb-bell" appearance of the interatrial septum? | Lipatomous hypertrophy of the interatrial septum |
| What is Lutembacher's syndrome? | Mitral stenosis with an ostium secundum ASD |
| What conditions are responsible for the highest incidence of left atrial thrombus? | 1. Rheumatic mitral stenosis 2. Atrial fibrillation |
| Which one of the following is NOT a primary, benign adult cardiac tumor? A. Myxoma B. Lipoma C. Angiosarcoma D. Hemangioma | C. Angiosarcoma |
| What type of cancer has the highest rate of metastases to the pericardium? | Melanoma Melanoma has the highest rate of pericardial metastases, but it is fairly uncommon. |
| What condition is most commonly associated with a sinus of Valsalva aneurysm? | Ventricular septal defect (40%) |
| Which of the following statements is NOT true regarding patients with a suspected restrictive cardiomyopathy? A. Concentric LVH may be present B. An outflow tract obstruction is typically present C. Left ventricular diastolic function is abnormal D. Right ventricular hypertrophy may be present | B. An outflow tract obstruction is typically present |
| Inhaling amyl nitrate may cause a sub aortic stenosis to increase. TRUE or FALSE | TRUE |
| In the absence of a right ventricular outflow tract obstruction, the right ventricular systolic pressure (RVSP) equals the? | Systolic pulmonary artery pressure (SPAP) |
| Right coronary artery dominance happens in about 80% of cases and is when the RCA gives rise to which coronary artery? | The PDA |
| Which ventricular septal defect would you visualize in the parasternal short axis view at the aortic valve area in the 12-3 o'clock position? | Outlet VSD |
| Sinus solitus refers to ______? | The normal relationship between the position of the heart, lobes of the lungs, and abdominal organs. |
| What are the typical changes seen on the electrocardiogram of a patient with an increase in ventricular muscle mass (hypertrophy)? | 1. Increases in R wave amplitude 2. Changes in the ST segment 3. T wave inversion 4. Pronounced Q wave |
| S4, or the fourth heart sound, can be described as? | an atrial gallop |
| When a cardiac murmur is detected, it is graded on a scale of 1-6. A 4/6 systolic murmur along the lower left sternal border accompanied by a palpable "thrill" would indicate a(n)? | ventricular septal defect (VSD) |
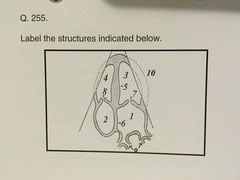
| 1. Left atrium 2. Right atrium 3. Left ventricle 4. Right ventricle 5. Inferoseptal wall 6. Interatrial septum 7. Mitral valve 8. Tricuspid valve 9. Pulmonary veins 10. Anterolateral wall | |
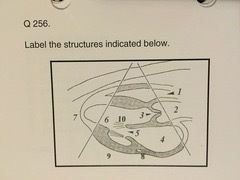
| 1. Right ventricle 2. Aorta 3. Aortic valve 4. Left atrium 5. Mitral valve 6. Left ventricle 7. Apex 8. Coronary sinus 9. Posterior wall 10. Chordae tendinae | |
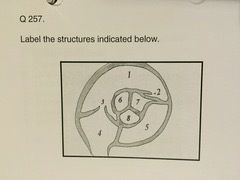
| 1. Right ventricular outflow tract 2. Pulmonic valve/pulmonary artery 3. Tricuspid valve 4. Right atrium 5. Left atrium 6. Right coronary cusp 7. Left coronary cusp 8. Non-coronary cusp | |
| Which ONE of the following statements is false regarding the Doppler waveform and flow velocity findings in a patient with mild diastolic dysfunction: A. The isovolumic relaxation time is < or = 110 msec B. The E velocity is low and the A velocity is high C. The deceleration time is > or = 240 msec D. The E/A ratio is < 1.0 | A. The isovolumic relaxation time is < or = 110 msec |
| Which of the following is NOT a view that can be used to obtain a continuous wave Doppler tracing from the ascending aorta? A. Suprasternal B. Right parasternal C. Parasternal short axis D. Apical five chamber | C. Parasternal short axis view The Doppler signal is perpendicular to flow rather than parallel |
| A congenital anomaly of the mitral valve in which there is two mitral valve leaflets but only one papillary muscle to attach to is called ______? | Parachute mitral valve |
| Which of the following is the least likely cause of calcification of the mitral valve annulus? A. Metabolic disease B. Aging C. Hypertension D. Pulmonic stenosis | D. Pulmonic stenosis |
| CSA (cm2) x VTI (cm) = | Stroke volume (cm3) |
| Which of the following is NOT considered an origin of mitral valve prolapse? A. Pulmonary disease B. Ischemic heart disease C. Valvular heart disease D. Myocardial disease | A. Pulmonary disease |
| In severe cases of aortic stenosis, the aortic root may: A. Decrease in size B. Dilate C. Hypertrophy D. Decrease in echogenicity | B. Dilate |
| An ausculatory finding in tricuspid stenosis of an increase in intensity of the diastolic murmur with inspiration is referred to as: A. DeRosier's sign B. Carvallo's sign C. Murphy's sign D. Ebstein's sign | B. Carvallo's sign |
| What is the least likely region for pulmonic stenosis to occur in a patient with Tetralogy of Fallot? A. Infundibulum B. Pulmonic valve C. Pulmonic trunk D. Subinfundibular | D. Subinfundibular |
| Which of the following is NOT a cause of mechanical valve failure? A. Pannus ingrowth B. Valve tears C. Bad design D. Loss of sutures around the sewing ring | B. Valve tears |
| Of the following, which is the primary feature on the echocardiogram of a left bundle branch block? A. Upward movement of the inter ventricular septum at the onset of electrical depolarization B. Downward movement of the interventricular septum at the end of the electrical depolarization C. Downward movement of the interventricular septum at the onset of electrical depolarization D. Flattening of the interventricular septum | C. Downward movement of the interventricular septum at the onset of electrical depolarization |
| When the aortic valve is measured from its initial opening to its closing, what calculation is being performed? A. Wall stress B. Ejection fraction C. Left ventricular ejection time D. Stroke volume | C. Left ventricular ejection time |
| What are the indications for contrast to be added to an echocardiographic study? | Two or more wall segments are poorly visualized. To improve visualization of cardiac masses. To enhance conventional cardiac Doppler signals. Stress echocardiography. TEE evaluation for a source of embolism. |
| Which one of the following statements is NOT true regarding harmonic tissue imaging? A. Harmonic tissue imaging requires a high mechanical index B. Harmonic imaging of bubbles requires a low mechanical index C. Harmonic tissue imaging may make valves appear thinner than what they really are D. Harmonic tissue imaging is an excellent method when performing stress echocardiography | C. Harmonic tissue imaging may make valves appear thinner than what they really are |
| Which one of the following statements is NOT true regarding the use of tissue Doppler in echocardiography? A. It is used to quantitate wall motion B. It is used to assess systolic function C. It is used to assess diastolic function D. It is used to determine valve orifice | D. It is used to determine valve orifice |
| The appearance of contrast in the left heart after a peripheral venous injection is diagnostic of a: A. Right to left shunt B. Left to right shunt C. High grade stenosis of the aortic valve D. High grade stenosis of the mitral valve | A. Right to left shunt |
| The appearance of contrast in the right heart following a direct left-sided pulmonary venous, or capillary wedge injection indicates: A. Severe systemic hypertension B. A left to right shunt C. A right to left shunt D. Severe pulmonary hypertension | B. A left to right shunt |
| What are the three major levels of shunting typically detected using peripheral venous injections? | 1. Atrial septal defect 2. Ventricular septal defect 3. Pulmonary A-V fistula |
| The term "situs inverses" refers to ______? | The right-to-left reversal of the cardiac and abdominal viscera. |
| After determining unresponsiveness in an adult victim, the first action a rescuer should take is: A. Start CPR immediately B. Find a partner and start CPR immediately C. Activate Emergency medical services (call 911) D. Perform a finger sweep of the patient's mouth | C. Activate Emergency medical services (call 911) |
| To check the pulse on an adult victim, the rescuer should palpate the? A. Brachial artery B. Radial artery C. Carotid artery D. Subclavian artery | C. Carotid artery |
| The rate of compression during CPR on an adult should be: A. 80 per minute B. 100 per minute C. 120 per minute D. Rate doesn't matter | B. 100 per minute |
| What type of atrial septal defect may be associated with abnormal drainage of the right pulmonary vein? A. Ostium primum B. Sinus venosus C. Ostium secundum D. Ostium sinus | B. Sinus venosus |
| What calculation is used to determine the pulmonary to systemic shunt ratio? A. Dp/dt B. CSA C. Qp/Qs D. SV/CO | C. Qp/Qs |
| Which leaflet of the tricuspid valve is usually least affected by Epstein's anomaly? A. Septal B. Posterior C. All leaflets are affected the same D. Anterior | D. Anterior |
| What is the most common type of ventricular septal defect? | membranous |
| A membranous VSD, a large overriding aorta, and a right ventricular outflow tract obstruction are findings in what type of congenital abnormality? | Tetralogy of Fallot |
| A shunt from a patent ductus arteriosus will be noted from the ______ to the ______? | Aorta to the right pulmonary artery |
| Which one of the following syndromes has a high association with endocardial cushion defects? A. Down's syndrome B. Marfan's syndrome C. Eagle-Barrett syndrome D. Fitz-Hugh Curtis syndrome | A. Down's syndrome |
| Which of the following tumors invade the heart via extension through the IVC? A. Renal cell carcinoma B. Rhabdomyoma C. Wilm's Tumor D. Teratoma E. A and C F. B and C | E. A and C |
| One of the most likely sources for a thrombus in the right side of the heart is ______? | Venous thrombus that has embolized to the heart |
| What is the most common tumor found in children? | Rhabdomyoma |
| What type of tumor occurs on the AV node? | Mesotheliomas |
| What valve is most commonly affected after a myocardial infarction? | Mitral valve Often times after a MI, patients present with a new murmur due to mitral valve dysfunction. |
| The basal LV is divided into ______ segments of ______ degrees each. | 6, 60 The basal LV is divided into 6 segments of 60˚ each. They are the basal anterior, basal anteroseptal, basal inferoseptal, basal inferior, basal inferolateral, and basal anterolateral. |
| What is the normal range for the diameter of the left ventricular posterior wall in diastole? | 0.6 to 1.1 cm |
| The mid LV cavity is divided into ______ segments of ______ degrees each. | 6, 60 The mid LV cavity is divided into 6 segments of 60˚ each. They are the mid anterior, mid anteroseptal, mid inferoseptal, mid inferior, mid inferolateral, and mid anterolateral. |
| The apical LV is divided into ______ segments of ______ degrees each. | 4, 90 The apical LV is divided into 4 segments of 90˚ each because of the myocardial tapering. There are the apical anterior, apical septal, apical inferior, and apical lateral. |
| What is the apical cap? | The apical cap represents the true muscle at the extreme tip of the left ventricle where there is no longer cavity present. |
| The wall of the heart is composed of three distinct tissue layers. Name and describe them. | Endocardium - inner layer composed of simple squamous epithelium and is continuous with the endothelium lining all blood vessels Myocardium - middle layer composed of striated cardiac muscle tissue Epicardium - outer layer of tough fibrous connective tissue covered by epithelium. The epicardium is also known as the visceral pericardium. |
| Which LV walls are seen in the apical long-axis view? | Anteroseptal and inferolateral |
| The Valsalva maneuver ______ venous return to the right heart. A. Decreases B. Stops C. Increases D. Doubles | decreases |
| Improper setting (too high) of the mechanical index, will cause what artifact when using ultrasound contrast agents? A. Swirling B. Attenuation C. No contrast effect D. None of the above | A. Swirling The majority of the swirling artifacts are caused by improper system settings such as high mechanical index or incorrect focal zone placement. A high mechanical index causes microbubble destruction and, therefore, swirling. |
| Besides the mechanical index, what other system control can potentially cause microbubble destruction? A. Dynamic range B. Overall gain C. TGC D. Focus | D. Focus |
| What will occur as a result of using multiple focal zones? A. Frame rate decreases B. Reduces dynamic range C. Increases frequency D. Decreases compression | A. Frame rate decreases Multiple transmit focal zones greatly expand the focal region, however, frame rate is sacrificed (decreases temporal resolution). |
| If the sonographer wants to improve temporal resolution, this can be accomplished by: A. Using a shallower image depth B. Decreasing the sector width C. Increasing the frequency D. Both A and B E. Both B and C | D. Both A and B |
| Lowering the mechanical index is required when using transpulmonary contrast agents. This is accomplished by: A. Decreasing frequency B. Decreasing output power C. Increasing dynamic range D. Increasing compression | B. Decreasing output power |
| What is the function of the receiver gain? | This control affects all areas of the image equally by controlling the amount of amplification performed by the receiver. |
| To correct a swirling artifact from contrast, you can: A. Increase the amount of contrast B. Decrease the mechanical index C. Reposition the focal point D. All of the above | D. All of the above |
| Attenuation is one of the most common artifacts when using ultrasound contrast. This is usually a result of: A. Rapid administration B. Low concentration C. Low mechanical index setting D. Improper focal zone placement | A. Rapid administration |
| What are the risks of esophageal intubation associated with a TEE? | Dental Trauma Esophageal trauma or perforation Bleeding Aspiration Dislodgment of endotracheal tube Displacement of nasogastric tubes |
| The role of the sonographer during TEE includes all of the following except: A. Preparing the patient B. Monitoring the patient C. Assisting with ultrasound equipment D. Inserting the probe | Inserting the probe (this should only be down by a licensed physician trained in performing this procedure). |
| M-mode displays ______ on the horizontal axis. A. Length B. Area C. Time D. Depth | Time |
| Increasing the depth of the image ______ the frame rate. A. Increases B. Decreases C. Doubles D. Does not affect | decreases |
| In order to increase the depth of penetration, one would: A. Decrease sector width B. Decreased transducer frequency C. Increase Dynamic range D. Increase transducer frequency | B. Decreased transducer frequency |
| Post processing of the ultrasound single is performed ______ image storage. A. Before B. During C. After D. All of the above | After |
| In order to increase axial resolution, one would: A. Increase transducer frequency B. Increase depth C. Decrease transducer frequency D. Decrease sector width | A. Increase transducer frequency |
| What is the most common reason for a papillary muscle rupture? | Post myocardial infarction |
| A "spanish notch" is visualized with which pathology? | Constrictive pericarditis |
| Which organs in the body are the most affected by systemic hypertension? | Heart, brain, and kidneys |
| What are the types of ventricular hypertrophy? | Concentric hypertrophy - equally distributed increase in wall thickness with normal chamber dimensions Concentric remodeling - increase in wall thickness, normal chamber dimensions and elliptical ventricular chamber shape Eccentric hypertrophy - increased ventricular dimensions, spherical ventricular chamber size Asymmetric hypertrophy - non-uniform increase in wall thickness |
| What are the reasons that a sonographer might get a false positive for pericardial effusion? | A false positive diagnosis of pericardial effusion on the echocardiogram can occur in pleural effusions, pericardial thickening, increased pericardial fat (especially the anterior epicardial fat pad), atelectasis, and mediastinal lesions. |
| In constrictive pericarditis, the most characteristic finding is: | Abnormal septal motion, described as "septal bounce" |
| What is the purpose of the pericardium? A. Minimize friction B. Provide protection C. Keep heart contained in chest cavity D. All of the above | All of the above |
| How is pulmonary hypertension diagnosed by Doppler echocardiography? | By obtaining a tricuspid regurgitation signal or a pulmonary valve signal. To obtain the degree of the pulmonary hypertension, we would perform the modified Bernoulli equation on the valve and then add the RAP. These two together are considered the RVSP. |
| What are the most common secondary findings on the 2D echocardiogram in a patient with pulmonary hypertension? | Right ventricular hypertrophy and dilation and right atrial enlargement. |
| Pulmonary artery flow patterns recorded in patients with pulmonary hypertension demonstrate: A. A late onset of flow B. An early peak velocity C. An abrupt reduction of flow in mid-systole (notching) D. All of the above | D. All of the above |
| In the absence of pulmonic stenosis, RV systolic pressure should be equivalent to: A. PA systolic pressure B. PA diastolic pressure C. Systemic pressure D. None of the above | A. PA systolic pressure |
| What are the three most common types of cardiomyopathy? | Dilated Hypertrophic Restrictive |
| What are the most common causes of dilated cardiomyopathies? | Most cases of dilated cardiomyopathy are idiopathic. Other causes include viral infections, alcohol and other toxic substances, poor nutrition, inflammation (myocarditis), pregnancy and childbirth, heredity, acquired immune deficiency syndrome (AIDS), ischemic heart disease. |
| What is/are the most common 2D echo feature(s) of dilated cardiomyopathy? A. Dilated LV cavity B. Decreased global systolic function C. Increased LV mass D. All of the above | D. All of the above |
| What are the most common M-mode echo-features of a dilated cardiomyopathy? | Dilated LV (possible LA, RA, and RV dilation) Increased mitral EPSS Diminished aortic root motion B-notch on mitral valve |
| Restrictive cardiomyopathy is characterized by mitral inflow velocities that show: A. Increased E velocity B. Decreased A velocity C. Shortened deceleration time D. All of the above | D. All of the above |
| The echocardiographic features listed below most likely represent which form of cardiomyopathy? -LV hypertrophy -Hypertrophy of other cardiac structures including intertribal septum -"Granular sparkling" appearance of ventricular myocardium -Normal or small-sized ventricles with dilated atria | A restrictive cardiomyopathy due to amyloidosis. |
| What are the most common etiologies of hypertrophic cardiomyopathy? | The most common cause of hypertrophic cardiomyopathy is hereditary with about half transmitted by autosomal dominant mechanism. Other causes included hypertension (with disproportionate LV hypertrophy occur in setting of hypertensive patient), valve disease. |
| What are the common 2D features of hypertrophic cardiomyopathy? | LV hypertrophy, which is usually asymmetric and involves the ventricular septum. The pattern of hypertrophy can range from "classic" septal hypertrophy to isolated apical hypertrophy. The LV size is usually normal or decreased and there is usually normal LV systolic function. LA enlargement is usually present. |
| What are the common Doppler features of hypertrophic cardiomyopathy? | Impaired ventricular diastolic function. Mitral insufficiency is typically present and a subset of patients will have LV outflow tract (LVOT) obstructions. |
| What are the provocative maneuvers used in patients with hypertrophic cardiomyopathy? | Valsalva maneuver and amyl nitrate |
| What is the most likely cause for a reduced dP/dt? | Decreased systolic function With systolic dysfunction, rise in ventricular pressure is reduced so MR shows a reduced rise to maximum velocity. |
| RV infarction occurs most commonly when there is an occlusion of which coronary artery? | Right coronary artery |
| Which view is best for assessing RV infarction? A. Parasternal long-axis B. Parasternal short-axis C. Apical 4-chamber D. Apical long-axis | Parasternal short-axis The parasternal short-axis view has been shown to have the highest sensitivity (82%), with a specificity ranging from 62-93% for hemodynamically important RV infarction. |
| The ability of the RV to pump equivalent cardiac output as the LV is due to: | Low pulmonary vascular resistance |
| Besides myocardial infarction, other causes of segmental LV dysfunction include: | RV pressure/volume overload (paradoxical) Post-cardiac surgery Left bundle branch block (LBBB) WPW syndrome Pacemaker |
| The rate of LV pressure change during the isovolumic contraction period is called ______. | dP/dT |
| Approximately what percentage of primary cardiac tumors are benign? A. 25% B. 50% C. 75% D. 100% | C. 75% |
| Where are myxomas most commonly found? | Approximately 75% of myxomas are found in the LA, with 20% in the RA and the remaining 5% equally distributed between the LV and RV |
| Describe the echocardiographic features of papillary fibroelastomas. | Papillary fibroelastomas are generally small (< 1 cm); usually single, almost always attached to valve surfaces (most often to the aortic valve) and may be pedunculated with some mobility. Round, oval, or irregular in appearance with well-demarcated borders and a homogeneous texture. |
| What is the vena contracta? | The narrowest central flow region of a jet that occurs at, or just downstream to, the orifice of a regurgitant valve. |
| How can you differentiate Lambl's excrescences from papillary fibroelastomas by echocardiography? | Papillary fibroelastomas are larger and more gelatinous than Lambl's excrescences, and they are present anywhere on valvular surfaces away from the lines of closure. Lambl's excrescences are, by definition, at the sites of valve closure. |
| What is the most common echocardiographic finding in metastatic disease? A. Pericardial effusion B. Left ventricular hypertrophy C. Right ventricular enlargement D. Mitral insufficiency | A. Pericardial effusion |
| List some normal anatomic variants that can be confused with cardiac tumors. | Moderator band Crista terminalis Eustachian valve Chiari network Hiatal hernia Pectinate muscles False tendon |
| Paradoxical septal motion on the m-mode echocardiogram is most commonly seen with: A. Right ventricular volume overload B. Left ventricular volume overload C. Right ventricular pressure overload D. Left ventricular pressure overload | A. Right ventricular volume overload |
| Right ventricular volume overload is commonly seen with: A. Ventricular septal defects B. Pulmonary stenosis C. Mitral insufficiency D. Atrial septal defects | D. Atrial septal defects |
| What is afterload? | Afterload is the pressure that the chamber of the heart has to generate in order to eject blood. Everything else held equal, as afterload increases, cardiac output decreases. |
| What are the four types of pulmonary stenosis? | -Valvular - the valve leaflets are thickened and/or narrowed -Supravalvular - the pulmonary artery just above the pulmonary valve is narrowed -Subvalvular (infundibuluar) - the muscle under the valve area is thickened, narrowing the outflow tract from the RV -Branch peripheral pulmonic stenosis - the right or left pulmonary artery is narrowed, or both may be narrowed |
| What is the most common cause of pulmonic stenosis? | Congenital Disease of the pulmonary valve are most often congenital, and only rarely do acquired disorders such as carcinoid and rheumatic fever affect the pulmonary valve. |
| Secondary findings on the echocardiogram in a patient with pulmonic stenosis may include: A. Left ventricular hypertrophy B. Left atrial enlargement C. Right ventricular hypertrophy D. All of the above | C. Right ventricular hypertrophy |
| What congenital anomaly produces an "hourglass" deformity of the ascending aorta? A. Bicuspid aortic valve B. Supravalvular aortic stenosis C. Coarctation of the aorta D. Tetralogy of Fallot | B. Supravalvular aortic stenosis |
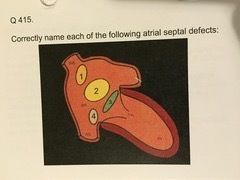
| Name the types of atrial septal defects. | Atrial septal defects are divided into four types according to their location: secundum, premium, sinus venosus, and coronary sinus defects. |
| 1 = Sinus venosus - the least common type of ASD and is located in the upper portion of the atrial septum. A sinus venous ASD often has an abnormal pulmonary vein connection associated with it 2 = Ostium secundum - the most common type of ASD and it occurs in the center of the septum between the right and left atrium - the area of the fossa ovalis. A variant of this type of ASD is called a patent foramen ovale – PFO 3 = Ostium primum - the next most common type and is located in the lower portion of the atrial septum. This type of ASD often will have a cleft mitral valve associated with it 4 = Coronary sinus - result from direct communication of the coronary sinus and the left atrium | |
| Which ASD is most commonly associated with endocardial cushion defect? | Ostium primum |
| What is Qp/Qs? | The ratio of pulmonary-to-systemic flow. The amount of shunt through any defect may be expressed as a ratio of pulmonary to systemic flow or Qp/Qs. It can be measured using both 2D and Doppler. - Measure the area of both the aortic and pulmonary valves using the equation: (pi)(r)(2) (r=annulus diameter/2). - Trace the Doppler flow through each valve to get the time-velocity integral and express the product of these two numbers as a ratio. Normally, with no shunt, the Qp/Qs is 1. A Qp/Qs > 1.5 is a significant shunt. |
| What echocardiographic feature(s) is/are associated with ASD? A. Right ventricular volume overload B. Left ventricular volume overload C. Left ventricular volume overload D. All of the above | A. Right ventricular volume overload |
| What is the Myocardial Performance Index? | It is the ratio of total LV isovolumic time to ejection time, and can be used as a global measure of systolic and diastolic function. MPI = IVRT + IVCT/SEP |
| How is contrast (agitated saline) used to detect an atrial septal defect? | A right-to-left shunt can be detected by visualizing bubbles in the left atrium and the left ventricle. A left-to-right shunt can be detected as a negative contrast washout effect in the right atrium. |
| Inlet VSD's are best seen in which view. A. Apical 4-chamber B. Apical 2-chamber C. Apical 5-chamber D. Apical long-axis | A. Apical 4-chamber |
| Muscular VSD's are best seen in which view: A. Parasternal long-axis B. Parasternal short axis C. Apical 4-chamber D. Apical 5-chamber | Parasternal short-axis view Muscular (trabecular) VSD's can be seen anywhere along the septum from this view. |
| Describe the hemodynamics associated with a ventricular septal defect. | A left-to-right shunt occurs because pulmonary vascular resistance is less than systemic vascular resistance. RV pressure is raised to systemic levels if the defect is large. As a result, pulmonary arterial pressure may be greatly elevated. |
| What are the two types of congenital subaortic stenosis? | Discrete, membranous, and tunnel subarotic stenosis |
| Name the three layers of the artery wall. | Intima, media, and adventitia The wall of the aorta is made up of three layers: a thin inner layer of smooth endothelial cells called the intimal, a muscular middle layer which has elastic fibers in it called the media, and a tough outer layer called the adventitia. |
| Describe the difference between a true aneurysm and pseudoaneurysm. | When the aneurysm involves all three layers, they are called true aneurysms. A pseudoaneurysm is contained only by the two outer layers of the blood vessel wall and clot. |
| Aortic aneurysms are classified by: A. Shape B. Location C. Cause D. All of the above | D. All of the above Aortic aneurysms are classified by shape, location along the aorta, and how they are formed. |
| A fusiform aneurysm: A. Involves only the adventitia B. Involves the entire circumference C. Is a form of dissecting aneurysm D. Separates the intima and media | B. Involves the entire circumference Fusiform aneurysms involves the entire circumference and symmetrical. |
| What are the common etiologies for aortic aneurysm? | Atherosclerosis Hypertension Marfan's (connective tissue disorder) Inflammation (vasculitis) Trauma |
| Where is the most common site for an aortic aneurysm? A. Ascending thoracic aorta B. Descending thoracic aorta C. Aortic arch D. Abdominal aorta | D. Abdominal aorta |
| What shape are most aortic aneurysms? | Fusiform Most aortic aneurysms are fusiform with widening all around the circumference of the aorta. Saccular aneurysms are not as common and involve just a portion of the aortic wall. |
| Where is the most common site for coarctation? A. Ascending aorta B. Aortic arch C. Descending aorta D. Abdominal aorta | Descending aorta |
| What is the most common congenital anomaly associated with coarctation? A. Bicuspid aortic valve B. Ventricular septal defect C. Atrial septal defect D. Tricuspid atresia | A. Bicuspid aortic valve |
| What are the causes of sinus of Valsalva aneurysm? | Primary cause – Congenital Secondary Causes: Atherosclerosis Syphilis Marfan's syndrome Blunt or penetrating chest injury Infective endocarditis |
| What are the pitfalls in using the modified Bernoulli equation? | 1) A velocity proximal to the stenosis greater than 1.5 m/s 2) The presence of two stenotic areas proximal to each other 3) The presence of a long tunnel-like stenotic lesion |
| What is the continuity equation? | The continuity equation states that the flow passing through a stenotic valve is equal to the flow proximal to the stenosis. |
| What is PISA? | Proximal isovelocity surface area (PISA) |
| "Switching" can occur at three levels. They are: | 1. Atrial-venous 2. Atrioventricular 3. Ventriculoarterial |
| In laminar flow, the velocity of blood is: A. Lowest in the center of the vessel B. Lowest at the vessel wall C. Highest at the vessel wall D. Directly proportional to the vessel diameter | Lowest at the vessel wall Flow is highest in the center and lowest at the vessel wall. |
| The Doppler angle yielding the highest Doppler shift is: A. 0˚ B. 60˚ C. 90˚ D. 180˚ | A. 0˚ |
| Continuous wave Doppler: A. Provides information on depth B. Cannot measure high velocities C. Does not alias D. All of the above | C. Does not alias There is no aliasing with CW Doppler but it cannot determine the depth from which a signal originates. |
| Gating determines the: A. Sample volume length B. Doppler frequency C. Frame rates D. Aliasing velocity | A. Sample volume length |
| The highest blood flow velocities present can be best evaluated by: A. Color Doppler B. Pulsed wave Doppler C. Continuous wave Doppler D. High PRF Doppler | C. Continuous wave Doppler |
| Theta is the angle between ______ and ______. | blood flow the ultrasound beam |
| The Nyqvist limit ______ when the sample volume is placed at 12 cm than when at 4 cm (implying transducer frequency is unchanged). A. Does not change B. Is lower C. Is higher D. None of the above | B. Is lower |
| List some of the common indications/objectives for stress echocardiography. | Evaluation of patients with suggestive or known Coronary Artery Disease Risk stratify patients before surgery, after myocardial infarction, and prior to starting an exercise diet program To evaluate systolic function To identify viable, hibernating, or stunned myocardium To evaluate hemodynamics |
| When performing treadmill stress echocardiography, post exercise imaging must be accomplished within: A. 5 minutes B. 3 minutes C. 90 seconds D. 30 seconds | C. 90 seconds |
| How would you calculate the target heart rate for a pharmacologic stress echocardiogram? | For a pharmacological stress echo, you would like to reach 85% of the maximal heart rate. The maximal heart rate is 220 minute the age of the patient. |
| Name the stress modalities used for stress echocardiography. | Exercise - treadmill, supine bicycle, upright bicycle Pharmacologic - dobutamine, dipyridamole, adenosine Other - atrial pacing - direct or esophageal |
| Which protocol is most commonly used for treadmill stress echocardiography? | The Bruce protocol is the most widely adopted protocol and has been extensively validated. The protocol has seven stages, each lasting three minutes, resulting in 21 minutes of exercise for a complete test. |
| What are some endpoints of a stress echocardiogram? | Achieved target heart rate Patient unable to continue due to fatigue ECG tachyarrhythmias Severe angina pectoris ST segment changes Increases in blood pressure to unsafe levels |
| List some of the contraindications for stress testing. | - Acute myocardial infarction - Uncontrolled unstable angina - Uncontrolled heart failure - Acute myocarditis or pericarditis - Acute systemic infection - Deep vein thrombosis - Uncontrolled hypertension (systolic blood pressure > 220 mmHg, diastolic > 120 mmHg) - Severe aortic stenosis - Severe hypertrophic obstructive cardiomyopathy - Untreated life threatening arrhythmia - Aortic dissection - Acute pulmonary embolism or infarction |
| If a wall of the left ventricle was scored with a "2", that would mean the wall was _______. | hypo kinetic |
| A normal response to exercise is: A. An increase in left ventricular contractility B. A decrease in systolic wall thickening C. Myocardial ischemia D. Dyskinetic wall motion | A. An increase in left ventricular contractility |
| Where is the SA node located? | Right atrium |
| What do the following waves represent on the ECG? P wave QRS complex T wave | -The P wave represents atrial depolarization -The QRS represents vent. depolarization -The T wave represents vent. depolarization -Atrial repolarization occurs during the QRS complex and produces such a low signal amplitude that it cannot be seen apart from the normal ECG. |
| Propagation of the electrical signal from the AV node to the ventricles is provided by the: | Bundle of HIS The bundle of HIS branches into the three bundle branches: the right, left anterior and left posterior bundle branches that run along the interventricular septum. |
| Describe Frank-Starling law. | - The ability of the heart to change its force of contraction and therefore stroke volume in response to changes in venous return. |
| What is stroke volume? | The amount of blood pumped during each cardiac contraction. |
| Cardiac output equals: A. Stroke volume x heart rate B. End-diastolic volume - end-systolic volume C. Left ventricular end-diastolic volume - left atrial end-diastolic volume D. None of the above | A. Stroke volume x heart rate |
| What is isovolumic contraction? | During this phase, the LV pressure abruptly increases as a result of the contraction of the heart. All valves are closed during this phase, thus, no blood is ejected from the ventricles and volume remains the same. This phase begins with the closing of the AV valves and ends with the opening of the semilunar valves, is preceded by atrial systole and followed by the rapid ejection phase. |
| What is isovolumic relaxation? | LV pressure abruptly decreases as a result of the relaxation of the heart. All valves are closed. This phase begins with the closing of the semilunar valves and ends with the opening of the AV valves. Ventricular pressures decrease; however, volumes remain constant because all valves are closed. Left atrial pressure continues to rise due to venous return from the lungs. |
| What is ejection fraction and what is a normal value? | Fraction (percentage) of blood pumped out a ventricle with each heartbeat. Healthy individuals typically have ejection fractions 55 to 70%. |
| What is S1? | First heart sound |
| What is S2? | The second heart sound marks the beginning of ventricular diastole. It is produced by closure of the aortic and pulmonic (semilunar) valves when the intraventricular pressure begins to fall. |
| What are the two main uses of Doppler in echocardiography? | 1. To detect flow 2. To be able to quantitate flow velocities |
| What is the advantage of pulsed wave Doppler over continuous wave Doppler? | Pulsed wave Doppler has range resolution, which means it is able to sample velocities from a specific area. |
| How can PA diastolic pressure be measured when pulmonic insufficiency is present? | The velocity of PR reflects the instantaneous gradient between PA and RV. Thus, the PR velocity at end-diastole may be used to derive the PA diastolic pressure with the 4V2 equation and adding to the pressure gradient an estimate of mean RA pressure. |
| What is the Doppler effect? | Doppler effect is the apparent change in observed sound frequency caused by relative motion between the sound course (or scatterer) and the observer. The frequency is lowered when the source is moving away from the observer and raised when it is moving toward the observer. In diagnostic ultrasound, three classes of Doppler detectors are used: continuous wave Doppler, pulsed wave Doppler and color Doppler. |
| Describe laminar flow. | Laminar flow occurs when all the red cells in an area are moving at approximately the same speed and in the same direction. Due to friction, flow is always slightly slower near the walls of a vessel. |
| Describe the turbulent flow. | Turbulent or disturbed flow occurs when there is obstruction that results in a disruption of the normal laminar pattern. When flow is turbulent, there are many different velocities detected at any one time (a wide spectrum of velocities). Such turbulence results in the spectral broadening (display of velocities that are low, mid and high) and an increase in peak velocity. |
| What is the main disadvantage of pulsed wave Doppler? | It is not able to measure high velocities. |
| What is the main advantage and disadvantage of continuous wave Doppler? | Advantage = ability to measure high velocities Disadvantage = no range resolution |
| All Doppler flow systems encode the directions of flow into two primary colors. What are they? | Red and blue. Red and blue are chosen because they are primary colors of light (together with green). |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Quer criar seus próprios Flashcards gratuitos com GoConqr? Saiba mais.