29146649
Descrição
FlashCards por Lourdes Khalil, atualizado more than 1 year ago
|
|
Criado por Lourdes Khalil
mais de 3 anos atrás
|
|
| Questão | Responda |
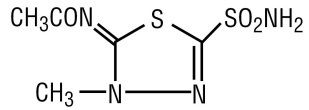
| -Acetazolamide -1,3,4-thiadiazole sulfonamide -Carbonic anhydrase inhibitor (CAI) | |
| -methazolamide -1,3,4-thiazdiazole sulfonamide -Carbonic anhydrase inhibitor (CAI) | |
| -Ethoxzolamide -sulfonamide is attached to a fused 1,3-benzothiazole ring -Carbonic anhydrase inhibitor (CAI) | |
| -Dichlorphenamide -disulfonamide derivative -Carbonic anhydrase inhibitor (CAI) | |
|
Image:
Chl (binary/octet-stream)
|
-chloraminophenamide -replaced the Cl of dichlorphenamide with NH2 -increased activity but urine not alkaline -> doesn't work through CAI |
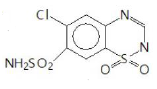
| -6-chloro-1,2,4-benzothiadiazine-7-sulfonamide-1,1-dioxide -benzothiadiazine (new class that doesn't alter urine pH) -acetylated the NH2 of chloraminophenamide and ring closure. | |
| -chlorothiazide (thiazide if no Cl, info below 3n thiazide generally) -weakly acidic -benzothiadiazinde 1,1-dioxide nucleus (sulfur is oxidized) -removal or replacement of SO2NH2 (7th pos) -> decreases activity -EWG at 6th pos (Cl, CF3) -> increases activity -EDG or H at 6th pos -> decreases activity -interchange SO2NH2 and Cl -> decrease activity -lipophilic grp at C3 (ie C of the =) -> increase potency -haloalkyl or thioether at C3 -> increase DOA -small alkyl grp 2-N -> decrease polarity and DOA | |
| -hydrochlorothiazide -reduction of double bond between C3-N4 -> increased activity 10x (this is the only difference between it and chlorothiazide) | |
| -benzthiazide -thiazide -has benzyl | |
| -bendroflumethiazide -thiazide | |
| -quinethazone -thiazide-like diuretic -quinazolinone derivative -orally active -long DOA (18-24h) 50-100mg/day | |
| -metolazone -thiazide-like diuretic -quinazolinone derivative -orally active -long DOA -more potent than quinethazone (2.5-20mg/day) | |
| -chlorthalidone -thiazide-like diuretic -Phthalimidine derivative -orally active -long DOA (48-72h), 25-100mg/3X a week | |
| -Indapamide -Indoline derivative -thiazide-like diuretic -orally active -long DOA (34-36h) -potent (2.5-5mg/day) | |
| organomercurial agents | -loop diuretics -not used anymore -have Hg (mercury) in their structure -Chloromerodrin, Meralluride USP, Sodium mercaptomerin and Mercurophylline NF XII MOA: inhibit Na+ reabsorption at the thick ascending loop of Henle (main) + inhibit Na+ and K+ reabsorption at the collecting duct |
| -Furosemide (lasix) -5-sulfamoyl-2-aminobenzoic acid -loop diuretic (new) -has furanylmethyl as R on NH -most potent | |
| -Azosemide -5-sulfamoyl-2-aminobenzoic acid -loop diuretic (new) -has furanylmethyl as R on NH but has tetrazole instead of COOH -> respectable diuretic activity | |
| -bumetanide (bumex or burinex) -5-sulfamoyl-3-aminobenzoic acid -loop diuretic (new) 50X more potent than furosemide | |
| -Piretanide -5-sulfamoyl-3-aminobenzoic acid -loop diuretic (new) -has pyrrolidine | |
| -Torsemide -sulfonylurea derivative (pyridine sulfonylurea derivative) -Loop diuretic (new) -similar effect as sulfamoyl benzoic acid -non-aryl sulfonamide -less incidence of ototoxicicty | |
|
Image:
Erthh (binary/octet-stream)
|
-Ethacrynic acid -Phenoxyacetic acid derivative -loop diuretic (new) -for max activity: alpha,beta unsaturated carbonyl + oxyacetic grp at para of = + CL or CH3 grps at C2 C3 + terminal H of the alkene is free -has greater ototoxicity and GI disturbances |
| -Spironolactone -Aldosterone dependent K+ sparing agent -Aldosterone receptor antagonist (synthetic competitive mineralocorticoid receptor A-) -orally active -prodrug (inactive) -> has 2 active metabolites | |
| -7alpha-thiomethyl-spironolactone -active metabolite (major) of spironolactone -has the lactone and has the 7th position substitution | |
| -canrenone -active metabolite of spironolactone -has a = at the 7th position + lactone -significant t1/2: 16.5h -> long DOA -is in equilibrium with potassium canrenoate | |
| -potassium canrenoate -metabolite from canrenone -ring of canrenone opened -> no lactone -> inactive -still has the chance to get active by re giving canrenone (reversible/equilibrium process the OH is nucleophilic and can attack carbonyl and form the ring again) | |
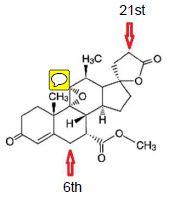
| -Eplerenone -Aldosterone dependent K+ sparing agent -aldosterone receptor antagonist -orally active -longer t1/2: 5h -NOT a prodrug -> metabolized into inactive metabolites: 6-beta hydroxy and 21-hydroxy -epoxide is specific to this drug -> conformational change -> more specific/selective to aldosterone receptor (even tho less potent than spironolactone) | |
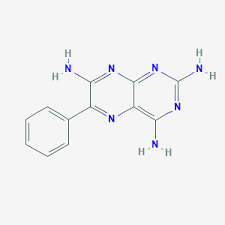
| -triamterene -pteridine derivative -Non-aldosterone dependent K+ sparing agent -non-aldosterone receptor antagonist -incomplete absorption -extensively metabolized -t1/2: 4h -20% unchanged renal excretion, 80% metabolized -2 active metabolites: 4'-hydroxytriamterene and its sulfate conjugate -AE: renal stones, hyperkalemia | |
| -4'-hydroxytriamterene -active metabolite of triamterene | |
| -amiloride -aminopyrazine derivative -Non-aldosterone dependent K+ sparing agent -non-aldosterone receptor antagonist -open chain analogue of triamterene -guanidine moiety -> quite basic mostly charged -incomplete absorption (too hydrophilic bcz of the aminos...) -t1/2: 221h -unchanged renal excretion, no renal stones, hyperkalemia | |
|
Image:
Sulf (binary/octet-stream)
|
-4'-Hydroxy Triamterene Sulfate conjugate -active metabolite of triamterene |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Quer criar seus próprios Flashcards gratuitos com GoConqr? Saiba mais.